

It has been suggested that the clinical examination of a patient is a dying art (Uddin, 2019), and that clinicians' loss of aptitude in this area has contributed to an inability to formulate an appropriate differential diagnosis and hampered the ability to diagnose (Asif et al, 2017). Within the context of modern medicine, where investigations using radiology and ultrasound abound, it could be argued that the need for a thorough clinical examination has been diminished (Elder et al, 2017; Elzanaty et al, 2019). However, such investigative modalities are not globally available and, where they are, access to them is neither unlimited nor without expense. In some cases, reliance on such investigations has been highlighted as a ‘significant threat to patient safety’ (Asif et al, 2017). Furthermore, we know that incomplete or faulty clinical examinations are a source of incorrect diagnoses (Graber et al, 2005) and that omitting examination techniques altogether can lead to diagnoses being missed (Bordage, 1999), with some researchers specifically noting that:
‘Most errors in the physical examination … [which lead to adverse outcomes] … are related to not performing an examination.’
This study sought to explore the experiences of allied health professionals who had trained to work at an advanced practice level, in relation to a range of clinical examination skills (Box 1).
Box 1.Selected clinical examination skills
Respiratory
| Clinical examination skill | ||
|---|---|---|
|
|
|
Background
‘Advanced practice’ is a term encompassing a number of specialist or advanced roles fulfilled by nurses and allied health professionals (including paramedics, physiotherapists and radiographers). There is a growing number of advanced practice courses being taught across the UK (Nadaf, 2018; Health Education England (HEE), 2019). Although some specific roles may be specialist in nature, clinicians working at advanced practice level are expected to:
‘Undertake a comprehensive and sophisticated physical … assessment of patients with complex … healthcare needs.’
Furthermore, any time a patient is examined is an opportunity to detect serious pathology (Elzanaty et al, 2019). To examine patients with potentially complex conditions safely and effectively it would be reasonable to expect clinicians trained as advanced practitioners to be competent in a range of standard clinical examination skills. Furthermore, there is a clear patient safety issue related to poorly performed, or poorly understood, clinical examination skills, where errors or omissions can lead to harm through delayed or missed diagnoses (Bordage, 1999; Graber et al, 2005; Verghese et al, 2015; Asif et al, 2017; Elzanaty et al, 2019). There is no current consensus list of what such a range of standard skills or scope of practice for advanced practitioners should encompass, and ‘no standardisation exists’ to guide advanced practice education (Nadaf, 2018:91). However, Ward and Barratt (2009) suggested the following examinations as core skills that can be evaluated in relation to assessing nurses completing their master's level courses in advanced practice:
- Ear, nose and throat
- Respiratory, cardiac and peripheral vascular
- Abdominal
- Pelvic (including vaginal)
- Musculoskeletal (including back, neck, shoulder and knee) Neurological (including peripheral and cranial nerve examinations).
Other authors, writing in relation to nurses and allied health professionals educated to advanced practice level, have included those examinations listed above with some additions, for example:
- Prostate examination (Abbott and Ranson, 2017)
- Male genital examination (Altman, 2004)
- Breast and thyroid examinations (Rhoads and Jensen, 2015).
Rawles et al (2017) suggested a wide range of examinations, including all those listed above.
Although advanced practice clinicians may be employed in a specific specialist area, there is international consensus that clinical examination skills have been found to cross disciplines and are likely to be useful in any area of clinical practice (Elder et al, 2017). As a specific example, thyroid pathology necessitating a thyroid examination, could present to general practice (as a goitre), acute medicine (toxic crisis), urgent care (hoarseness), psychiatry (mania or psychosis), an emergency department (palpitations), or could present while an inpatient as a result of general anaesthesia or physiologic stress from surgery, and could be a presenting complaint for a paediatric patient (commonly as a goitre), or during obstetric or post-partum care (thyroiditis). Using such an example, it would be reasonable to expect an advanced practitioner in any of these specialties, or settings, to be conversant with a basic thyroid examination and be able to undertake one, despite not being an endocrine specialist, as would be expected of a doctor working in any of these areas.
There is a current paucity of evidence relating to which clinical examination skills are considered essential or core knowledge in advanced practice; however, those included in Box 1 are common across a number of texts on this subject from experts in advanced practice education and practice.
This study aimed to assess the perceived practical and theoretical instruction received in relation to these clinical examination skills on advanced practice courses in the UK by a number of nurses and allied health professionals, through use of a survey.
Method
This study was assessed against the Medical Research Council (MRC) and Health Research Authority (HRA) assessment tool (MRC and HRA, 2013) and did not require formal approval from an ethics board. Participants were free to terminate their involvement with the survey at any time and no personal or identifiable information was requested. Any personal identifiable information provided in free-text responses was anonymised.
An online survey using the Google Forms platform was opened to responses for 1 month between 23 July 2019 and 23 August 2019, with the link being placed on two UK advanced practice forums on the Facebook social media platform. This methodology was chosen for this exploratory work to allow a broad convenience-based sample across a large population. Participants were not asked to detail specifically where they had received their training and education to facilitate honest feedback about their experiences, and any mention of such identifying details in the free-text comments were anonymised. Answers to closed questions are presented with simple statistical analysis and free-text responses are presented using a thematic analysis approach. Thematic analysis is a commonly used and flexible method of coding qualitative data to express the content of such free-text responses in a meaningful and accessible manner (Willig and Rogers, 2017).
Free-text results were reviewed a number of times by the author following the standard pattern of familiarisation, coding, theme development and reviewing themes to produce the final six themes presented (Willig and Rogers, 2017). Inductive semantic coding was used, which produced initial code lists that were later developed into themes. It was felt that, for such exploratory work into the provision of education to practitioners, overtly interpretive coding was beyond the scope of the study, and that this inductive approach would be less prone to researcher bias (Medelyan, 2021).
The clinical examination skills chosen (Box 1) were selected to represent a broad spread of clinical examination skills, all of which are taught and assessed on medical degrees in the UK and worldwide (Smith et al, 2016; Danielson et al, 2019). It is important to note that the list of skills shown in Box 1 is not exhaustive and it is likely that further examinations, and examination modalities, such as point-of-care ultrasound, are likely to become important components of the core undergraduate curriculum for doctors if not all allied health professionals in the coming years (Dinh et al, 2015).
Results
Ninety-six (n=96) responses were received during the 1 month duration of the online survey, with 92% (n=88) of these currently working in an advanced practice role. The majority of respondents identified their professional registration as being adult or general nursing (n=63, 66%), with the next common registration being paramedic (n=26, 27%). Responses were also received from physiotherapists (n=2) and paediatric nurses (n=3). With a single response in each of the following groups: mental health nurse, radiographer, podiatrist, community public health nurse, general practice nurse, primary care specialist nurse and health visitor. The majority of respondents identified themselves as advanced practitioners (n=39, 41%) or advanced clinical practitioners (n=38, 40%), with fewer identifying as practitioners (n=13, 14%) or specialist practitioners (n=5, 5%)
When asked at what level their training and education had been to allow them to practise at an advanced practice level, the majority indicated that they had undertaken a master's-level qualification (n=71, 74%), with 10 respondents (10%) indicating postgraduate diploma level and only small numbers indicating education to a postgraduate certificate (n=4, 4%) or bachelor's level (n=9, 9%).
In relation to clinical examination skill education, the survey asked about 12 examinations (Box 1). Specifically, it sought to understand where clinicians had received education and training in both the theoretical basis and practical undertakings of these examinations. The results from the quantitative phase show a clear discrepancy between the prevalence of teaching provided in relation to the core body systems (respiratory, cardiovascular and so on) and the more specific or intimate examinations (prostate, breast, genitalia and so on) in both theoretical (Figure 1) and practical (Figure 2) teaching.
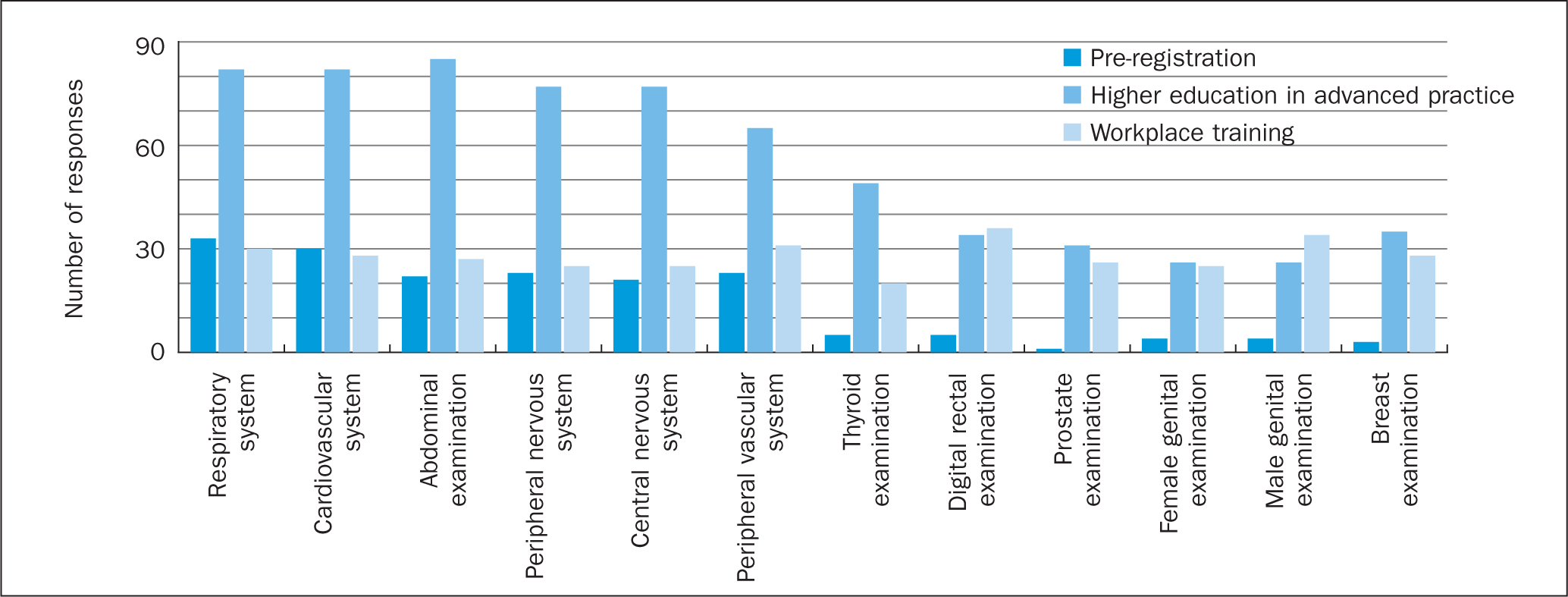 Figure 1. Theoretical teaching in clinical examination
Figure 1. Theoretical teaching in clinical examination  Figure 2. Practical teaching in clinical examination
Figure 2. Practical teaching in clinical examination
As a direct comparison, 85% (n=82) of respondents were taught the theory surrounding a cardiovascular and a respiratory examination during their higher education advanced practice training, while far fewer were taught the theory of a female or male genital examination (n=26, 27%) or a breast examination (n=35, 36%). This meant that the majority of advanced practice clinicians surveyed here had received no theoretical teaching on these subjects during their advanced practice university course/module. Even among those who had received some theoretical teaching of these examinations at university, fewer had received practical teaching in relation to these intimate examinations. Only 19% (n=18) of the cohort surveyed had received practical instruction during their higher education modules on how to undertake an examination of female genitalia, and only 20% (n=19) for the equivalent male examination. In relation to practical training at university in breast examination, only 27% (n=26) of respondents had received such educational input. Similar numbers and trends are presented for rectal and prostate examination, with a slightly higher number receiving theoretical and practical education in thyroid examination (51% theoretical, n=49; 43% practical, n=41) in a higher education setting.
In addition, around a quarter of respondents indicated having never been taught the theory or practice around thyroid, rectal, prostate, genital or breast examinations during pre-registration training, advanced practice training in higher education, or in the workplace (Figure 3). All respondents reported being taught the theoretical and practical elements in relation to the examination of the respiratory and cardiovascular systems, as well as an abdominal examination. It is worth noting that, despite these system examinations appearing to be widely taught, previous research into advanced practice has found that nurse practitioners highlighted their lack of confidence in performing cardiac, abdominal and respiratory examinations as significant hindering factors to their practice (McElhinney, 2010), despite having been taught these assessment skills. If these results are extrapolated to the larger advanced practice population in the UK, this may suggest that a quarter of such practitioners are unable to, or are entirely self-taught in relation to, their examination of the thyroid, rectum, prostate, genitalia and breasts. However, larger scale research would be necessary to make such generalisations with a high degree of certainty.
 Figure 3. Clinical examinations never taught
Figure 3. Clinical examinations never taught
In a further, qualitative phase of this study, participants were asked whether they felt the clinical examination skills documented in Box 1 should all be taught on advanced practice courses. This question received 92 responses (96% of total respondents), of whom 85% felt that they should all be taught as part of an advanced practice course, with 10 people disagreeing and four agreeing with caveats. Space was also provided for free-text comments in relation to the teaching of clinical examination skills at advanced practice level. These were analysed using thematic analysis.
Discussion
Quantitative phase
A significant lack of theoretical and practice-based teaching and a heterogeneity of experiences is demonstrated by these results in relation to the intimate examinations (digital rectal examinations, prostate, breast and genital), with a related lack of teaching on the thyroid, when compared with the major organ systems. Similar results have been found in medical students, with Abdulghani et al (2016) finding that around 80-90% of their sample had never performed a genital examination prior to graduation. This is concerning because all of these examinations can easily reveal findings necessitating urgent investigation for serious disorders, including cancer (NHS Scotland, 2019). With many advanced practice clinicians now working in areas where they see an undifferentiated caseload of increasingly complex patients in their daily practice (HEE, 2017) such a lack of education and experience begins to be a cause for concern. This lack of educational provision is also an area of which to be mindful in relation to workforce planning, because allied health professionals are increasingly working in roles traditionally undertaken by medical doctors (Baileff, 2015), for whom all of these clinical examination skills should have been taught and assessed at medical school.
We know from previous studies that medical students find gaining competence in male and female intimate examination challenging (Dabson et al, 2014), and that when focused teaching is provided for these examinations, confidence and competence increases (McBain et al, 2016). It is therefore concerning that advanced practitioners are finding these skills rarely taught in theory, or in practice, during their higher education in advanced practice.
When considering why some clinical examinations appear not to be taught, it is worth looking at the guidance provided by the professional bodies of the clinicians working in such roles in relation to their expectations of scope of practice. Many such documents avoid being too prescriptive in relation to the skills required to work at advanced practice level, and instead make general statements such as that practitioners will be able to ‘use a range of different … assessment methods’ (Royal College of Nursing, 2018:6) or deliver ‘enhanced patient assessment skills’ (College of Paramedics, 2018:6). This leaves room for interpretation and subsequent variation in advanced practice curricula across the country as has previously been noted (Clever Together, 2019). The other extreme also exists where documents related to advanced practitioners list a selection of specific clinical examinations that would be expected of an advanced practitioner. This is the case in the collaborative document from the College of Paramedics and Skills for Health (2018), which states that specialist paramedics should:
‘Apply a range of physical assessment techniques appropriately … including, as appropriate, neurological, cardiovascular, respiratory, musculoskeletal or abdominal examination.’
College of Paramedics and Skills for Health, 2018:21
The same document does make specific reference to being competent in digital rectal examination; however, it does not mention genital examination or thyroid examination at all, yet expects specialist paramedics in primary care to be familiar with ‘breast … swelling and/or lumps’ (2018:39), while not mentioning that breast examination skills are essential. A separate document from the College of Paramedics published 1 year later (2019) added that the armamentarium of specialist or advanced paramedics might include rectal and vaginal examination, and a selection of other examination techniques, but did not set a minimum or desired scope of practice. With such guidelines being produced by professional bodies whose members are working at advanced practice level, it would be unsurprising if educational institutions are unclear about which core clinical examinations skills are required to be taught on advanced practice modules.
Thematic analysis: qualitative phase
Emergent coding and subsequent thematic analysis of the free-text responses revealed six recurring themes (Box 2).
Box 2.The six themes extrapolated from qualitative data
| 1 | These skills are essential in practice |
| 2 | Intimate examinations are not being taught |
| 3 | Teaching is not at an appropriate level |
| 4 | Teaching in a clinical setting is vital |
| 5 | Underpinning theory and clinical reasoning are not well taught |
| 6 | There is an impact on patients |
Comments relating to the importance of consolidating theoretical knowledge in practice, in an effort to close the theory–practice gap were common across the themes. It is important, however, to be mindful that, for learning in practice to be effective in closing this gap, comprehensive theoretical teaching must have already taken place. Furthermore, for some examinations (such as female genital examination) there may be a discrepancy between the experiences of learners based on their own sex once in the clinical setting (Wallbridge et al, 2018), making the theoretical teaching phase vitally important.
Discussion: qualitative phase
1. These skills are essential in practice
‘On my MSc-level course the training did not include all physical examination elements that are essential to work in general practice.’
Nurse educated to master's level
‘I think you should be able to perform the full range of basic assessments—which are essentially listed above.’ [list presented in Box 1]
Paramedic educated to master's level
A number of free-text responses reaffirmed that the clinical examinations skills presented in Box 1 represent a standard baseline of assessment skills likely to be required for most clinicians, other than those in highly specialised roles who may struggle to maintain ongoing competence in examination skills not used in their day-to-day practice. This expressed view aligns well with teaching for the medical profession, where all of these skills are taught on medical undergraduate curricula in the UK to allow an individual to work as a doctor on the foundation programme and subsequently progress to specialist practice (General Medical Council (GMC), 2013; 2016; 2020). Currently, there is no standardised list of core clinical examination skills required of advanced practitioners, as discussed above. However, it appears that the respondents in this study would view the included examination skills as among those essential for advanced practice.
The formulation of a standard curriculum for advanced practice in the UK would align with the goals of a number of organisations that have been clear that a consistent approach to advanced practice education is essential (HEE, 2017; NHS Wales and National Leadership and Innovation Agency for Healthcare, 2010; College of Paramedics and Skills for Health, 2018). It was also highlighted in responses that there is significant variation between advanced practice courses, with one respondent highlighting that they:
‘… did two clinical exam modules at different universities and [they] were completely different’
Nurse educated to master's level
This lack of consistency is concerning and warrants further investigation.
2. Intimate examinations not being taught
‘Gynae examination and diagnostic skills are a significant part of primary care but have never been touched upon in any part of my training.’
Paramedic educated to master's level
‘… physical assessment of adults course … genitalia, breast and DRE [digital rectal examination] not taught or discussed.’
Nurse educated to master's level
‘… rectal exam not covered at all …’
Nurse educated to postgraduate diploma level
Multiple free-text responses highlighted the omission of intimate examinations from the advanced practice patient assessment modules attended by the respondents. Four free-text responses specifically highlighted a lack of teaching around digital rectal examination (DRE) and prostate examination, with one respondent commenting:
‘There is a strange aversion to teaching PR [per rectum] examination in advanced practice courses, as it is a core skill.’
Paramedic educated to postgraduate certificate level
This is not a unique finding, and other authors have highlighted paucities in teaching rectal examination to medical students (Hennigan et al, 1991; Lawrentschuk and Bolton, 2004; Trzeciak et al, 2019). Although a DRE is limited in its ability to estimate prostate volume, it is still a useful examination for identifying an enlarged prostate (Christie et al, 2019), and is advocated in the examination for anorectal tumours (Hillman et al, 2019) and other important pathologies (Royal College of Surgeons, 2017). Therefore, the omission of such a core examination procedure from advanced practice education is surprising and potentially harmful for future patients (Dabson et al, 2014).
There are of course significant ethical considerations related to teaching intimate examinations using either the student cohort (Rees et al, 2009) or patients (Wilson, 2005), and it may be that the use of volunteers, ‘professional patients’ or manikins may offer a solution to these concerns (Wånggren et al, 2005; Hendrickx et al, 2006; Janjua et al, 2018). However, each of these alternatives come with drawbacks; a programme using trained volunteers and professional patients may be more financially costly (Janjua et al, 2018) as generally a ratio of 3-4 learners per volunteer is used (Wånggren et al, 2005), but this is likely to represent a more effective teaching modality than manikins (Hendrickx et al, 2006), which may lack the realism required to truly learn a diagnostic examination or procedure.
Such statements from advanced practice respondents describing intimate examinations as being essential to their clinical role but excluded from their education are concerning. This is certainly an area of advanced practice education that requires further review.
3. Teaching content not at an appropriate level
‘The level of neurological … and musculoskeletal examination is not taught at an advanced level for nurses, it doesn't even really cover the basics I was taught as a physio.’
Physiotherapist educated to master's level
A number of responses raised concerns about the quality and rigour of teaching received on advanced practice degrees and modules. Some responses highlighted some serious omissions from teaching sessions, such as lack of any teaching to examine:
‘… for femoral/inguinal hernias.’
Nurse educated to master's level
or that a:
‘… rectal exam [was] not covered at all.’
Nurse educated to postgraduate diploma level
Such omissions are potentially harmful to future patients (Dabson et al, 2014), especially where an omitted or incomplete examination (faulty data gathering) causes harm through a missed diagnosis (Graber et al, 2005). This also brings us back to the issues around consistency of advanced practice education discussed earlier, with such variations making it difficult to take a standardised approach to advanced practice roles across an organisation or nation.
Concerns around teaching being pitched at an incorrect level, or excluding examination techniques felt to be essential, can also be seen as a direct result of the lack of standardisation in terms of which clinical examination skills are considered core knowledge for an advanced practitioner. A consensus curricula across the four nations of the UK would be a useful starting point to ensure such standardisation.
4. Teaching in a clinical setting is vital
‘Teaching and practice combined whilst assessing in practice helps the theory–practice gap.’
Paramedic educated to postgraduate diploma level
‘Clinical skills are then built on in clinical practice.’
Nurse educated to master's level
‘Practical skills are best taught and learnt in practice.’
Nurse educated to master's level
Practice-based learning was highlighted by respondents as essential to learning and consolidating clinical skills. Although the exact nature of the theory–practice gap is still actively debated, it would be safe to assert that such a phenomenon exists, and that education in both settings can be used to bridge this gap. Despite this clear acknowledgement by some respondents of the importance of education in the workplace, others highlighted a complete lack of instruction in practice to accompany the theoretical teaching they had already received.
5. Underpinning theory and clinical reasoning are not well taught
‘The theory should be covered not just “you should do this as part of your examination”. What are you looking for or ruling out as a differential? What information will it add to your history? etc.’
Nurse educated to master's level
A number of free-text comments were critical of the theory-based teaching the respondents had received in terms of limited coverage of the underpinning knowledge related to clinical examination, with some responses highlighting a lack of detail, such as not being given a rationale for undertaking a specific examination technique, with a lack of further discussion around what pathology might be elicited and how this may alter a management plan. One respondent was clear that within advanced practice education:
‘The focus should be more upon interpretation of findings and clinical reasoning [than the] psychomotor skills.’
Paramedic educated to bachelor's level, working as an advanced practitioner
This highlighted the importance of such underpinning knowledge. Another respondent was critical of their master's level teaching, in that it did not cover the basics they had previously learnt at undergraduate level, with another commenting that core elements of a systems examination were completely omitted. This lack of teaching in relation to the supporting theories and knowledge base behind clinical examinations is a concern, and could leave practitioners open to making errors of judgement when caring for patients (Graber et al, 2005).
6. Impact on patients
‘In the areas … not taught I find it particularly hard to work up a patient and this means I avoid them. I would like to be able to competently assess these patients.”
Paramedic educated to master's level
‘[I] really struggle with female genital examination and cannot safely complete [an] episode of care for this patient [group] …’
Nurse educated to bachelor's level, working as an advanced practitioner
The final theme identified was that of the adverse impact on patients, and such concerns are not new. Past authors have highlighted that a paucity of clinical examination skills is a patient safety issue because it can lead to incorrect and missed diagnoses, causing a subsequent delay or omission of appropriate treatments (Bordage, 1999; Graber et al, 2005; Verghese et al, 2015; Asif et al, 2017).
Comments from respondents related to this theme highlighted that a lack of skills and knowledge in relation to some presenting complaints led to advanced practitioners being unable to provide the care they wanted to give to some patients and, in some cases, led to them avoiding certain patients or presenting complaints as a result. This is concerning because it severely limits the range of patients that can be safely assessed by such an advanced practitioner and leaves them open to ‘unknown unknowns’, which may present additional risks for patients in terms of missed or incorrect diagnoses. Graduating from an advanced practitioner course with insufficient skill and knowledge related to clinical examinations has the potential to have a significant negative affect on the future patients seen by that clinician (Graber et al, 2005; Dabson et al, 2014; Verghese et al, 2015). It is also interesting to note that these free-text responses support the earlier work of researchers such as Donelan et al (2013), who found that 88.9% of primary care physicians surveyed believed that nurse practitioners defer some of their workload to a primary care physician. If the UK continues to pursue its programme of advanced practice education across the gamut of allied health professionals, it would seem appropriate that clinical examination skills are taught in a consistent manner by different universities, and with an appropriate breadth and depth to facilitate high-quality clinical practice and ensure patient safety.
Conclusion
This exploratory research, which collated the experiences of 96 practitioners from various parent specialties, has highlighted gaps in postgraduate advanced practice education as perceived by advanced practice clinicians, which may represent a patient safety issue. This study suggests that multiple basic examinations are not adequately taught consistently on UK advanced practice courses, with, for example, only around a fifth of respondents being taught about genital examination and only round a half being taught how to undertake a thyroid examination. These findings should prompt investigation to further quantify the areas of clinical examination practice not being adequately taught, and ought to direct educators to assess their advanced practice courses in relation to the clinical examination skills discussed here.
Furthermore, it has previously been highlighted in a report by Clever Together (2019:45), commissioned by HEE, that there is a pressing need to ‘address confusion and variation in the advanced clinical practice MSc’ and the findings of this study demonstrate the clear heterogeneity of learners' experiences of advanced practice programmes. It may be that the development of a list of essential clinical examination skills, through a consensus process, may facilitate standardised curricula development for advanced practice and thereby help to reduce such variation between programmes.
The findings of this survey will also inform employers in relation to what training may be required for both new and established advanced practitioners in relation to these examination skills, where education appears to be lacking on some programmes. Employers should also be mindful that clinicians lacking appropriate theoretical and practical training in these examination skills will need additional support and mentoring in clinical settings, to allow them to consult safely and effectively with patients who may require such examinations.
KEY POINTS
- There is variability in the way that clinical examination skills are taught to advanced clinical practitioners on university courses
- Intimate examinations (breast, genital, rectal/prostate) are less likely to be taught than standard systems examinations (respiratory, cardiovascular, neurologic, abdominal)
- There appears to be significant variation in the teaching of clinical examination skills on advanced practice courses across the UK
CPD reflective questions
- In your practice, how do you support students to close the theory− practice gap?
- What additional examination skills would you like to undertake to benefit your patients?
- What would you consider to be core examination skills of someone practising at an advanced level?