

A parastomal hernia is a common complication associated with the creation of a faecal or urinary abdominal stoma (colostomy, ileostomy or urostomy). Parastomal herniation occurs when a loop of bowel protrudes outside the muscular abdominal wall, through the gap created to allow the passage of the stoma (Figure 1). This presents as a bulge under the peristomal skin, which may change in size or disappear and reappear as the ostomate moves.

Impact
Ostomates may be distressed by the visual appearance of the hernia, compounding the body image issues associated with having a stoma. The bulging also creates an uneven abdominal surface, making it more difficult for a stoma appliance to form a tight seal. A poor seal increases the risk of leakage and, consequently, peristomal moisture-associated skin damage (MASD), which is often a source of considerable discomfort, pain and distress. Consequently, parastomal hernias can have a profound negative impact on a person's psychosocial wellbeing and overall quality of life, as well as limiting their activities of daily living, with financial implications. This all also increases the care burden and financial costs for the healthcare system (Shiraishi et al, 2020).
Incidence
Parastomal hernias most often occur within 2 years of the creation of a stoma, but the possibility of diagnosis continues for 20 years after surgery (Londono-Schimmer et al, 1994). Parastomal herniation is also often associated with other stoma-related complications, such as peristomal skin complications (Shiraishi et al, 2020).
The precise reported risk of a person living with an ostomy developing a parastomal hernia varies considerably (Table 1). The incidence of developing a parastomal hernia after stoma surgery has been reported to be as high as 81% (Shiraishi et al, 2020). A recent systematic review by Harries et al (2021) concluded the incidence of symptomatic parastomal hernias to be as high as 58% and asymptomatic hernias 25.6%. This has led some writers to assert that some degree of parastomal hernia is practically inevitable over an ostomate's lifetime (Carne et al, 2003; Stylinski et al, 2018).
Table 1. Incidence of parastomal hernia by stoma type
| Type of stoma | Incidence range (%) |
|---|---|
| Loop ileostomy | 0–6.2 |
| Loop colostomy | 0–30.8 |
| End ileostomy | 1.8–28.3 |
| End colostomy | 4–48.1 |
| Urostomy | 5–28 |
Intra-abdominal pressure
The risk of parastomal herniation is closely linked to intra-abdominal pressure. This is the pressure inside the abdominal cavity and the way the body manages volume. Stoma formation typically weakens the abdominal musculature around the stoma, potentially providing a path of least resistance through which excessive intra-abdominal pressure can escape, causing herniation or stomal prolapse (a separate complication where the stoma itself protrudes further from the abdomen). The risk is greater in people with lower core strength.
Risk reduction
Parastomal herniation, despite being common, is potentially avoidable (Husain and Cataldo, 2008). Several studies have shown that the incidence of parastomal hernia development can be effectively lowered with risk-reduction strategies, with a positive impact on people's quality of life (Thompson and Trainor, 2007; North, 2014). These strategies involve techniques, including physical activity and abdominal exercises, intended to both regulate intra-abdominal pressure and increase tolerance of higher pressures.
Little advice is given to ostomates on how to understand and manage intra-abdominal pressure. There is a signficant difference in intra-abdominal pressures between laying supine, sitting and standing. Thus there is a need for instruction during postoperative progressive mobility, such as appropriate supine-to-standing procedures and considerations throughout the recovery process. Lack of advice might mean that ostomates inadvertently cause unnecessary damage when they cough, sneeze, strain, vomit, blow their nose or hold their breath in the early postoperative period and beyond. To moderate intra-abdominal pressure, ostomates should certainly be taught and encouraged to use safe techniques to move in certain ways and lift, push and pull objects, especially heavy ones. This should help them go about their normal lives, as well as engage in more formal exercise.
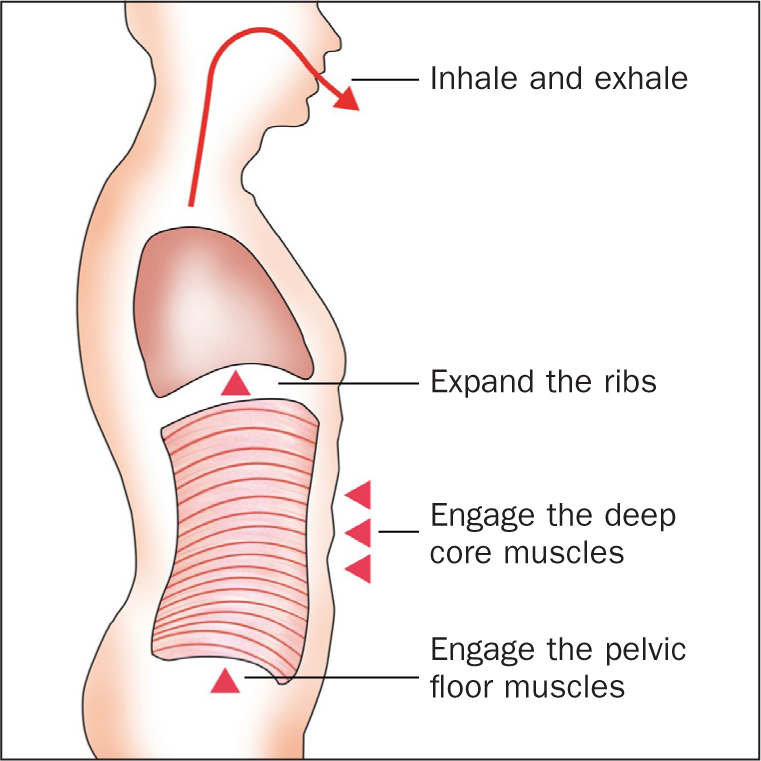
Intra-abdominal pressure can also be regulated through diaphragmatic breathing exercises (Figure 2). These exercises involve expanding the ribs and engaging the deep core and pelvic floor muscles while inhaling and exhaling. This diaphragmatic breathing pattern optimises movement and increases awareness of the deep core muscles, which prepares the person for everyday movement and lays the foundation for specific core exercises.
Strong, co-ordinated core muscles provide a supportive scaffold against herniation. Strengthening and increasing the co-ordination of the abdominal core muscles will increase their tolerance for higher levels of intra-abdominal pressure, making them better able to cope with things such as coughing or sneezing. This strength and co-ordination can be built with appropriate core muscle exercises, making this training a very important part of hernia risk reduction and management after any kind of abdominal surgery. The exercises should involve connecting with the deep core muscles. The deep core can be understood as a muscular container, with a top (diaphragm), bottom (pelvic floor) and sides (abdominal wall), all working together in synergy (Figure 3). When breathing, the diaphragm and pelvic floor move up and down together as the muscles contract and relax. The exercises teach the person to engage/contract and relax these muscles, helping to improve their breathing and moving patterns and thus regulate intra-abdominal pressure, reducing the risk of herniation.

These exercises should ideally be begun soon after surgery strategies but are still valuable many years after. Ostomates who have already developed a hernia should also perform these core muscle exercises to prevent the hernia from worsening and improve the chance of lasting successful repair.
Perils of inactivity
Despite the importance of exercise in minimising the risk of herniation, people recovering from abdominal surgery are traditionally recommended to avoid strenuous activity and exercise. Moreover, even after the recovery period, many ostomates avoid physical activity out of fear that it could result in a parastomal hernia (North, 2014).
This inactivity can cause several problems that negatively impact the person's quality of life. Being physically inactive puts people in danger of worsening health from chronic conditions, such as cardiovascular disease, cancer, obesity and diabetes, and it can increase people's risk of anxiety and depression (Russell, 2017; World Health Organization; 2018). Meanwhile, findings from a 2023 systematic review suggested that muscle loss after surgery increases the risk of herniation (Schutte et al, 2023).
A survey of more than 2500 people with a stoma in the UK found that half of those surveyed were doing less exercise after surgery than before, often because of a fear of hurting themselves (Russell, 2017). Almost all people surveyed (90%) did not meet UK guidelines for physical activity. Many had been instructed not to do any exercise (Russell, 2017).
When patients are often told not to lift anything heavier than a kettle for 3 months after surgery, this can make them apprehensive about any kind of exercise for a long time. The evidence suggests that surgeons and other health professionals are recommending that their patients avoid exercise altogether just because they have an ostomy. This incorrect response to an understandable concern represents a significant problem for ostomates and stoma care professionals, as being active is a major net positive for reducing hernia risk, as well as for general health and wellbeing.
Active recovery
Rehabilitation exercises can fit into existing enhanced recovery after surgery (ERAS) pathways, starting before surgery and picking up the day after surgery with gentle movements and exercises. Support for structured exercise should continue beyond the immediate postoperative period into the patient's foreseeable future. Eventually, people with a stoma can engage in almost any kind of physical activity, including lifting weights, so long as they take an appropriate approach to exercise. This means going through a step-by-step recovery process to rebuild muscles in the right way. Moreover, any recommended physical exercise should be tailored to the individual person's needs, as it must be something that they can engage with and stick with. People have different abilities and aspirations; some ostomates may aspire to be able to carry their own shopping or play with their grandchildren, while others run multiple marathons.
This exercise can be structured with Convatec's me+ recovery series, co-developed by Sarah Russell, a clinical exercise physiologist with a professional background in cardiac rehabilitation and a prolific endurance runner with an ileostomy. The series, which has been running since 2017, is based on gentle, evidence-based movement and breathing exercises for managing intra-abdominal pressure. The aim is not only for these exercises to support, guide and empower patients through the immediate recovery period after ostomy surgery, but also for them to be embedded into everyday life in the long term. This avoids postoperative patients being left alone after a few months of inactivity without direction or support for further physical recovery.
Engaging teams
Health professionals should be as good at telling people what they can do as what they can't do. It is important that patients receive similar advice from the entire multidisciplinary team (MDT), including the surgeon, physiotherapists and ward nurses. This likely requires only a relatively small change in mindset for members of the MDT. However, this change may need to be driven by specialist stoma care nurses, engaging their colleagues and getting them to work together.
Changing ingrained mindsets within the healthcare professions can be a challenge. To assist with this, Convatec is launching a new set of me+ recovery tools and modules focused on engaging the MDT and implementing patient recovery programmes. With the evidence showing the positive impact physical activity can have on people's lives, professionals should focus on telling patients what they can do after surgery – and how to do it safely.