

Intravenous (IV) therapy is an essential aspect of modern healthcare and commonly used within the NHS. Its advantages include improved patient outcomes and, in some cases, the IV route is the preferred option because it ensures consistent drug bioavailability and reliable therapeutic drug levels in the blood (Price and Patel, 2020). Unfortunately, the use of IV therapies is not without risks. While the benefits usually outweigh such risks, all staff involved in the administration of such therapies need a sound knowledge of potential complications. Infection associated with IV therapy and vascular access devices (VADs) is well known (Munoz-Mozas, 2023) and great efforts have been taken throughout the NHS to mitigate this risk in recent years. However, there are some complications that are less recognised and well known, including infiltration and extravasation.
Infiltration and extravasation are complications often associated with chemotherapy agents; however, non-chemotherapy drugs have been reported as having a greater rate and risk of serious complications (NHS Resolution (NHSR), 2022).
Infiltration is the inadvertent leakage of IV fluid or medication into extravascular tissue from a dislodged IV device, such as a peripheral cannula or central venous catheter (National Infusion and Vascular Access Society (NIVAS), 2024). The resulting injury can be minor depending on the volume of fluid infiltrated but large volumes of infiltrated fluid can lead to compartment syndrome (NIVAS, 2024).
An extravasation occurs if the fluid or medication involved in the infiltration is a vesicant; when extravasation occurs, the risk of tissue damage and serious injury can be very high (Atay et al, 2023; Nickel et al, 2024) because vesicants are drugs or solutions with the potential to cause serious skin or tissue damage including blistering, ulceration and necrosis (David et al, 2020; Nickel et al, 2024).
Four main groups of vesicant drugs are commonly used (NIVAS, 2024): Systemic anti-cancer therapy (SACT); drugs with non-physiological pH; vasopressors; and hyperosmolar solutions.
SACT is perhaps the best known IV therapy in relation to extravasation risk. This is so much so that, in order to administer SACT, oncology nurses need to undertake specialist administration training, including how to reduce the risk of extravasation and recognise when such an injury occurs. In the UK, SACT nurses need to update this knowledge annually; this is the primary reason why the rates of SACT extravasation are lower than in other IV therapy groups (NHSR, 2023).
Drugs with non-physiological pH can have a high or low pH. Every IV drug has a pH and osmolarity and its these chemical characteristics that classify the drug as a vesicant or non-vesicant. A pH range outside of neutral pH of blood (7.35–7.45) has the potential to cause irritation or damage to the tunica intima or the surrounding tissue. The higher or lower the pH range, the more damage extravasation can cause. It is generally considered that a pH value of between 5 and 9 is suitable for peripheral vein administration because the pH value is more likely to be tolerated by the peripheral veins (David et al, 2020; Couissi et al, 2023). Comparison of pH values between IV therapies and common household chemicals is an impactful tool to raise awareness in those giving IV therapy about the extreme pH values of some of the most common IV therapies given in clinical practice (Table 1). IV phenytoin (pH 12) and acyclovir (pH 10–11) have a pH value equivalent to bleach and hand soap. Vancomycin (pH 2.4–4.5) and gentamycin (pH 3–5.5) have a pH values equivalent to cola or vinegar (NIVAS, 2024).
Table 1. pH values of common IV therapies given in clinical practice
| pH | IV infusion | |
|---|---|---|
| Stomach acid | 1.5–2.0 | Glucagon pH: 2.5–3Vancomycin pH: 2.4–4.5Gentamycin pH: 3–5.5Glyceryl trinitrate pH: 3.5–6.5Metoclopramide pH: 3–5Amiodarone pH: 3.5–4.5Glucose 5% pH: 4–4.2Chlorpheniramine pH: 4–5.2Potassium pH: 40.9% Saline solution pH: 7Tazocin pH: 5–7AnnInophylline pH: 8.8–10Frusemicle pH: 8.3–9.3Acyclovir pH: 10–11Phenytoin pH: 12 |
| Cola | 2.5 | |
| Vinegar | 2.9 | |
| Orange juice | 3.5 | |
| Coffee | 5.0 | |
| Healthy skin | 5.0 | |
| Urine | 6.0 | |
| Pure water | 7.0 | |
| Human saliva | 6.5–7.5 | |
| Blood | 7.3–7.5 | |
| Sea water | 7.7-8.5 | |
| Baking soda | 8.4 | |
| Hand soap | 9.0–10.0 | |
| Bleach | 12.5 |
Vasopressor drugs such as noradrenaline and dopamine carry an extremely high risk of serious extravasation injuries if inadvertently administered into tissue. These drugs can also damage fragile peripheral vessels because of their potent vasoconstrictive effects and cause injury following effusion into the tissues with increasing hydrostatic pressure (Stefanos et al, 2023). For this reason, the safest way to administer vasopressors is via a central vein where the tip of the catheter is situated in the lower third of the superior vena cava (NIVAS, 2024).
Hyperosmolar solutions such as parenteral nutrition and contrast media used in CT scanning cause extravasation injuries because of their osmolarity. Studies suggest that hyperosmolar solutions above 600 mOsm/l (normal range 285-310 mOsm/l) should not be administered via a peripheral vein (Manrique-Rodríguez et al, 2021; Pittiruti et al, 2023) because they are associated with a higher risk of tissue damage. Calcium chloride 10% has an osmolarity of 2040 mOsm/l; this extremely high osmolarity can cause devastating damage to limbs if an extravasation occurs during administration into a peripheral venous catheter.
In 2022, NHSR published data in a document called, Did you know? Extravasation. Publication coincided with the start of a project by NIVAS (2024), which has produced a national extravasation and infiltration toolkit to enable hospitals in the UK to become more aware of these and put protocols and guidelines in place to prevent them or recognise them early (NHSR, 2022).
From 1 April 2011 until 31 March 2021, NHS Resolution received 444 claims relating to extravasation injuries. Of those 444 claims, 138 remain open, 197 have settled with damages paid and 109 have closed with nil damages. These have cost the NHS £15.6 million. This includes payment for claimant legal costs, NHS legal costs and damages.
Reviewing the data highlighted trends in infiltration and extravasation injuries. SACT extravasations accounted for only 24% of closed, settled claims; the other 81% were associated with non-SACT drugs. Paediatric injuries accounted for the largest group of non-SACT injuries at 23%. Infiltration of IV iron accounted for 9% of settled claims; these injuries were associated with permanent orange staining of skin rather than extravasation.
NIVAS extravasation and infiltration toolkit
The NIVAS extravasation and infiltration toolkit focuses on the prevention, awareness, treatment, reporting and follow-up of these injures.
NIVAS recognised that non-SACT extravasation injuries are often misdiagnosed in the early stages as cellulitis or phlebitis; this misdiagnosis often leads to IV antibiotic or dermatology referrals when the extravasation injury requires urgent treatment, often by the plastics surgical team. After the first few hours since extravasation, the chance of successful treatment is lost and the injury has the potential to evolve into something more serious.
Most extravasations and infiltrations occur when a peripheral IV cannula (PIVC) is involved and often arise because of a placement issue with the vascular access device (VAD). It seems that most of these issues occur in patients who have difficult IV access, often with very limited peripheral vein options. Deeper veins that are more difficult to visualise or palpate require deeper cannulation, which limits the amount of catheter situated in the vein, especially when using a standard length (10 mm-32 mm) cannula. This makes the cannula unstable and can lead to the catheter becoming dislodged from the vein but remaining in the subcutaneous tissue, which is when extravasation occurs (Bahl et al, 2021; NIVAS, 2024). Points of flexion in the wrist or, in particular, in the antecubital fossa are at high risk of causing an infiltration or extravasation owing to mechanical friction from the joint moving the catheters and damaging the tunica intima or causing catheter displacement (Welyczko, 2020).
Different VADs have different risks and complications associated with them; the length of the catheter, the material the catheter is made of and the securement of the device are all risk factors. One complication that all VADs are prone to is the formation of fibroblastic sleeves. Fibroblastic cells can grow along the catheter from the point of vessel entry, so that eventually the catheter tip becomes encased by a closed sleeve of tissue (Rousslang et al, 2020; Passaro et al, 2021; Cutuli et al, 2023). Consequently, the infused fluid flows back between the fibroblastic sleeve and the outside of the catheter to the catheter exit site and can potentially infiltrate into the subcutaneous tissue just below the catheter insertion site (Figure 1) (Pittiruti et al, 2023).

Consent
IV therapy administration has become routine and is so commonplace in healthcare that, unless SACT is being administered – which requires fully informed written consent – patients receiving non-SACT IV therapy will, at best, give implied consent. The justification for this is often that IV treatment is being given in an emergency or the clinical team looking after the patient may have discussed the need for IV therapy and the patient has agreed in general to IV therapy without ever being told that in some cases they may experience an extravasation.
Intravenous iron is an infusion that is routinely given in clinical practice. While it is not considered a vesicant, if IV iron infiltrates into the tissue, it will leave a permanent orange stain to the skin. When this occurs, it is often a surprise to the patient, when they realise they will have to live with the orange staining for life. Litigation often follows and the first questions asked by the court are: did the patient give consent to have this treatment, and were they informed about the possible side effects? As IV iron is usually an elective treatment, using the defence that it was given in an emergency will not be enough. The NIVAS extravasation toolkit (NIVAS, 2024) has highlighted data from NHS Resolution's (NHSR, 2022) extravasation work and recommends written consent from all patients receiving elective IV iron infusions.
NIVAS white paper
Choosing to administer IV therapy via a peripheral vascular access device is not always an easy decision, especially when the service to place a central vascular access device is not readily available and pathways for patients with difficult IV access are not in place.
Reducing extravasation injuries and other IV-related complications can be difficult in a hospital without a dedicated team to lead in the standardisation of clinical practice and act as a point of contact and clinical expertise. In 2022, NIVAS published a white paper, which supports the effectiveness of standardised vascular access teams with the NHS.
The aim of the white paper was to highlight the additional benefits of having a dedicated team who can support the insertion of all vascular access devices, from long term-devices to managing patients with difficult IV access. According to a NIVAS (2022) survey, so far in the NHS, approximately 55 hospitals have dedicated vascular access teams. Hospitals that do not have a dedicated full-time vascular access service team are less able to provide fast vascular access solutions. Fast, reactive teams who can place reliable vascular access devices can reduce the risk of infiltration and extravasation by reducing the numbers of attempts at peripheral cannulation or are able to place long-term vascular access devices without delay to coincide with the start of the patient's IV treatment, which is especially important for vesicant IV therapy regimes. A vascular access service is also more likely to embed standardised practice and use the most up-to-date technology to make IV therapy administration safer. They can also act as the organisation's extravasation lead.
A protocol for patients with difficult IV access can reduce complications and also improve safety and patient satisfaction (Rodriguez-Calero et al, 2020) (Figure 2). Having a simple pathway in place that leads to ultrasound placement for peripheral catheters can make a huge difference to patient experience. Ultrasound-guided placement of peripheral cannulae can increase the success rate and reduce the risk of dislodgement (Tran et al, 2021; Schoch et al, 2023). Multiple attempts at placing a PIVC are painful and distressing to the patient and may damage the vessel and surrounding tissue and therefore increase the risk of extravasation (Sweeny et al, 2022), the use of ultrasound for PIVC placement should be considered for all patients with difficult IV access.

The risk of extravasation can be further reduced if the most suitable VAD is selected (Meyer et al, 2020). A VAD decision making tool can be used to ensure that the most suitable vascular access device is selected based on the intended IV therapy (Moureau and Chopra, 2016; Ray-Barruel et al, 2020) (Figure 3). NIVAS's (2024) infiltration and extrasvastion toolkit provides a simple example of a VAD decision tool that ward based nurses and doctors can use to ensure they choose the safest device for the intended IV therapy.

Outdated, historical clinical practices associated with IV therapy and peripheral cannulation can play a part in increasing the risk of extravasation. In the absence of a central venous vascular access device, using a large-bore cannula in the antecubital fossa as a substitute for the administration of a vesicant is not safe practice and must be avoided. The use of small-bore catheters in the lower forearm should be the first choice for peripheral IV therapy; this practice is followed for SACT administration. VADs with a smaller diameter allow turbulent blood flow around the outer catheter lumen, thereby reducing the risk of injury to vessel wall caused by repeated pistoning or micromovement. Ideally, a catheter-to-vessel occupancy of less than 45% is recommended (Spencer and Mahoney, 2017; Sharp et al, 2015). Vascular access devices should be inspected at least once a shift and flushed at least daily; they should be removed if not working properly or no longer required (Lv and Zhang, 2020; Welyczko, 2020).
Even when systems are in place to reduce complications with IV therapy and VADs such as dedicated vascular access teams, difficult IV access pathways and vessel health decision-making tools, infiltrations and extravasations will still occur. When these do occur, reducing the level of harm is the next best thing to preventing them in the first place.
Recognising when an extravasation has occurred is vital and, according to Helm et al (2015), the published incidence of infiltration, occlusion, and accidental removal is disturbingly high. Up to 90% of catheters fail before therapy is complete, and catching extravasation early can reduce the amount of tissue damage. This is particularly important for infiltrations of neutral infusions because large volumes of infiltrated fluids can cause compartment syndrome.
Patient story
A patient had a 20 g closed-system cannula inserted in the cephalic vein in the wrist. They had difficult IV access, had COVID and were in a higher-level care unit. The patient had a single dose of IV vancomycin, which has a pH of 2.8–4.5. During the IV administration, the cannula became dislodged and the vancomycin extravasated into the subcutaneous tissue at the IV cannula site. The extravasation was not immediately noticed. The cannula was removed because it had failed to work properly, there was some erythema and swelling at this time and phlebitis was diagnosed. A peripherally inserted central catheter was inserted because the patient had difficult IV access. Seven days later, the injury had evolved into a grade 4 (NIVAS, 2024) extravasation (Figure 4). On investigation, the infusion of vancomycin was found to have taken less than 1 hour so was not within the 1-hour time frame to be visually checked by a nurse, which is the infusion protocol in the hospital. The patient was too unwell to alert staff about any pain at the infusion site. An infusion pump was used; however, the pump alarm pressure was set high and, because the patients' hands and arms were oedematous, the change in infusion pressure was not sufficient enough to set off the alarm before most of the vancomycin had been administered.

It is not possible to visually monitor every infusion with the human eye; some clinical units may be infusing over 20 patients at any one time. It is recommended by the NIVAS infiltration and extravasation toolkit (NIVAS, 2024) that IV infusions sites are monitored at least hourly and that infusions are given via a pump where possible, especially when a vesicant is being administered—but even an infusion pump cannot reduce the risk of infiltration or extravasation on its own.
With the application of new technology, for the first time a device is available in clinical practice that can continuously monitor IV infusion sites and indicate when an infiltration is occurring, often even before the patient or nurse is aware. The device is called ivWatch and its application in clinical practice could revolutionise IV infusion safety.
ivWatch is an IV infusion site monitoring device that applies advanced signal processing at the IV device site that can detect infiltrations in as little as 0.2 ml of IV fluid, with an average detection volume of 2–3 ml (Figure 5).

The ivWatch device uses a SmartTouch Sensor, which has two emitters and a detector to transmit and receive light signals to measure the changes in the optical properties and diffuse reflectance of the tissue near a peripheral IV site. The emitters transmit light to the tissue, and the detector, located a few millimetres away from the emitters, measures the reflected light signal. The reflected light signal primarily depends on the scattering and absorption properties of the monitored tissue. The ivWatch device detects the change in photon scattering in the diffuse reflectance signal and issues a check IV notification. When infiltrated fluid is present in the subcutaneous skin tissue, a significantly different diffuse reflectance signal occurs. Changes to diffuse reflectance are received by the SmartTouch Sensor and are analysed by ivWatch's proprietary algorithm to determine whether conditions indicate that an infiltration event may have occurred.
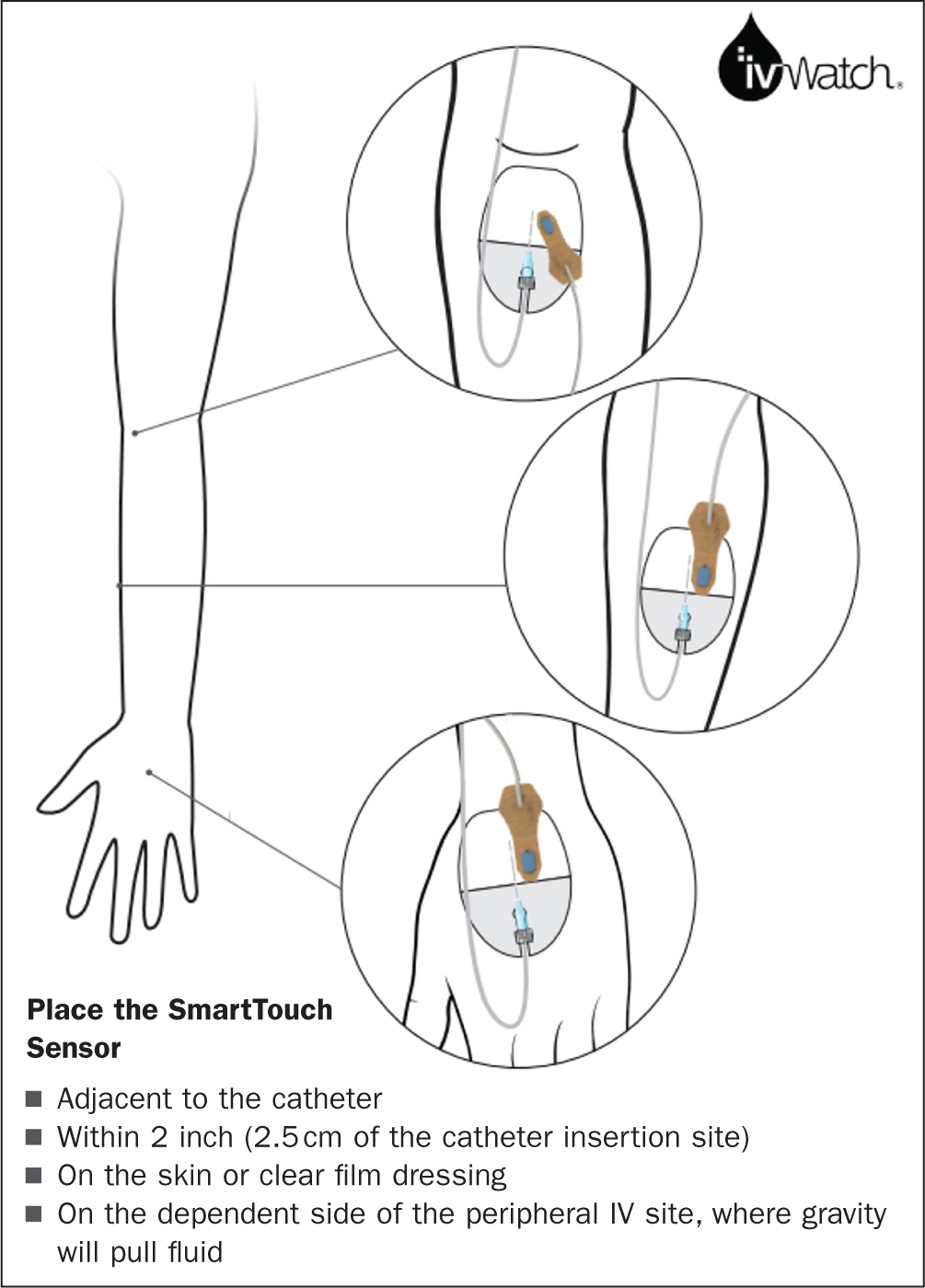
The sterile SmartTouch Sensor has an adhesive to apply to the skin in the area around the insertion point of the IV catheter; the sensor can be attached on top of the transparent part of the IV film dressing. The sensor can then detect when an infiltration occurs in the tissues around the indwelling part of the catheter.
The technology involved in the ivWatch and SmartTouch Sensor relies in light that scatters when a photon, or particle of light, is redirected because it interferes with a structure or particle in the tissue. Scattering structures in the tissue can include cells (eg blood cells and keratinocytes), fibres (eg collagen and elastin fibres) and cellular components (eg. mitochondria and nuclei). When there are more scattering structures in the tissue, more energy will be reflected back to the surface. Likewise, if there are fewer scattering structures in the tissue, less energy will be reflected back to the surface. Absorption occurs when the energy of the photon is absorbed by a structure in the tissue such as haemoglobin in the blood or melanin in the epidermis. When there are more absorption structures in the tissue, less energy will be reflected back to the surface. Likewise, fewer absorption structures result in more energy being reflected back to the surface. Diffuse reflectance refers to the measurement of photons that enter the skin tissue and then reflect back out after many scattering events.
When the SmartTouch Sensor detects an infiltration at the IV device site it will alert on the ivWatch monitor in two ways: a yellow alert, which means there is a potential infiltration; or a red alert, which indicates an infiltration is highly likely. A visible and audible notification from the iv Watch monitor then immediately alerts the practitioner, allowing them to stop the infusion and visually inspect the catheter site and make an assessment about continuing the infusion or resiting the peripheral IV catheter. Previous studies of the ivWatch have shown a high device reliability (ivWatch, 2023) and low false notification frequency, which has also been noted in previous studies (ivWatch, 2023). The quality and high level of clinical evidence available enables the ivWatch to be used with a high degree of confidence.
IV therapy and vascular access services ivWatch study
The first clinical study of the ivWatch infusion monitoring technology in the UK was undertaken at an infusion unit in a large NHS hospital between 14 August 2023 and 22 January 2024. The unit operates Monday to Friday 8am–6pm. The infusion unit administers a range of IV therapy infusions, including monoclonal antibodies, immunoglobulin, blood transfusion and blood products, antibiotics, zoledronic acid, Ferinject iron, electrolyte fluids and other disease-modifying therapies for long term conditions.
The infusion unit is part of a larger IV therapy and Vascular Access Services (IVAS), unit which also encompasses the home infection management service and the inpatient/outpatient vascular access service. Extravasation governance for the hospital falls under the remit of the IVAS unit and the lead for the unit is also the organisational lead for extravasation. Extravasation and infiltration injury reduction is an ongoing focus of the IVAS unit. Preventing iron infusion infiltration was a particular goal for the IVAS unit because the majority of the hospital's elective iron infusions occur in the IVAS unit.
The IVAS study and evaluation of the ivWatch was initially planned for 2 weeks. In that time, it was agreed that all IV therapy infusions in the IVAS unit that met the study criteria would be monitored with the ivWatch. The infusion unit has 23 infusion chairs, and the nursing model is three chairs to one infusion nurse, meaning an infusion nurse could be setting up and monitoring up to three patients at any one time. Infusion times ranged from 30 minutes to 7 hours depending on the drug therapy. Only patients having infusions via a peripheral cannula were selected for ivWatch monitoring. The ivWatch device used in the study is not designed for central venous device infusion monitoring because the SmartTouch Sensor is only effective in subcutaneous tissue because of the depth the sensor can reach.
The ivWatch team supported the infusion unit for the initial 2-week study to ensure the infusion nurses were given real-time, patient-facing education on how to place the adhesive sensors correctly and how to use the device so practice was standardised as much as possible. The ivWatch team also collected the data from each infusion to ensure they were valid and verified. At the end of the 2 weeks, the ivWatch team were able to produce a report containing the downloaded data from each device.
Every patient was given information about the ivWatch and gave consent for the device to be used during their infusion and for the infusion information to be anonymously collected and collated for the study evaluation. Ethical approval for the trial was not required because the use of the ivWatch did not change or increase the risk associated with the infusions, which was scheduled to take place. Before the study, the hospital's medical engineering department undertook an assessment of the 20 ivWatch devices and certified them safe to use in the infusion unit for the study.
The IVAS lead nurse asked that any yellow warnings be managed in the same way as a red alert; this meant resiting the peripheral cannula. This decision was made because, if a yellow alert was given by the ivWatch, there was a high probability that the infusion would go on to infiltrate and cause a red alert. Minimum yellow and red detection volumes were 0.20 ml and 0.21 ml. Average detection volumes were 2.02 ml and 2.13 ml for yellow and red, respectively.
The infusion unit staff continued to use ultrasound to place peripheral cannulas for the majority of the patients' infusions. Before the study and despite the use of ultrasound for cannula placement, the infusion unit rate of extravasation and infiltration was an average of five out of a mean 250 infusions per week that were between stage 1 and 3 (Figure 6) (NIVAS, 2024). The infusion unit has a policy of written informed consent before iron infusions so patients are aware of the risk of skin staining if infiltration occurred.

Results
During the first 2 weeks of the study, 20 ivWatch Model 400 monitoring systems were studied. A total of 206 infusions and 214 peripheral IV sites were monitored with the ivWatch for a total of 357 hours. The device captured 15 site infiltrations in the 214 peripheral IV sites monitored with an infiltration rate of 7.0%. All 15 infiltrations had been caught in the very early stages, so much so that the majority of patients had felt little if any pain or discomfort. No stageable infiltration or extravasation injuries reported.
All the patients who returned for multiple infusions during the 2-week study requested the use of ivWatch. The feedback from them was that the use of ivWatch made them feel more safe about receiving their infusion. The infusion nurses also felt reassured by the use of ivWatch as it gave them peace of mind too. One member of staff said it was like having a second pair of eyes to monitor the infusion site.
Because of the extraordinary success of the ivWatch study, the positive feedback from staff and patients and the reliability of the technology, it was agreed that the trial would continue.
Extended study results
The infusion unit continued to collect data on every peripheral infusion administered between 14 August 2023 and 22 January 2024. A total of 3507 hours of monitoring time was collected (Figure 7).

The average monitoring time per peripheral IV was 1.5 hours with the longest run time being 8.0 hours.
One hundred and twenty-two cases of red check IV notifications occurred in the 2254 monitoring runs, corresponding to a 5.4% check IV notification rate.
In addition, 59 cases with a yellow notification were also recorded. These were potential infiltrations, which the infusion unit staff acted on and resited the peripheral cannula.
Conclusion
The ivWatch study was a great success for the infusion unit. The results showed a higher-than-expected infiltration rate within the infusion unit which was due to the sensitivity of the ivWatch SmartTouch Sensor. When the data was analysed the highest percentage of drugs infiltrations were IV Ferinject (iron) at 45 infusions and zoledronic acid at 26 infusions, which has a pH of 2 (Figure 8). An extravasation of iloprost, which has a pH 8.4, was also detected before an injury occurred. In all but one of the cases, the ivWatch device prevented a stageable, noticeable or serious extravasation occurring.

There was one case of iron infiltration occurring during the study that resulted in a noticeable skin staining injury and this was attributed to incorrect placement of the ivWatch SmartTouch Sensor. In this case, the SmartTouch Sensor was applied too far away from the cannula insertion point so, by the time the ivWatch detected the infiltration and a red alert occurred, 10 ml of the iron had infiltrated into the skin. Following this infiltration, further training was given to the infusion nurses and a visual aid was produced to assist in the placement of the SmartTouch Sensor (Figure 9).
Discussion
The use of ivWatch has overwhelmingly improved infusion safety within the infusion unit. In a unit where peripheral vascular access devices are placed with ultrasound as a standard of practice, vessel assessment is routinely undertaken and longer length PIVCs are used, the risk of extravasation is already mitigated. For the ivWatch to identify and prevent injuries occurring in 5.4% of the infusion activity is compelling. The patients and staff have even higher confidence in the safety of the infusion therapy they are giving and receiving. The ivWatch study has demonstrated how successful the technology is, with 122 definite infiltration and extravasation injuries prevented and further potential yellow alerts averting 59 more. Based on this outcome, extravasation and infiltration injuries during IV therapy can be prevented.
KEY POINTS
- Infiltration or extravasation is a complication when a drug or IV therapy leaks into the tissues surrounding the vascular access device
- Extravasation is often associated with systemic anti-cancer therapy but non-chemotherapy drugs have been reported as having a greater risk of serious complications
- ivWatch can monitor IV infusion sites and indicate when an infiltration is occurring
- The indications for use at the time of this study were for optically clear solutions
- The SmartTouch Sensor is sterilised; however the device label may not include that depending on marketing area