

The cardiac examination is a fundamental part of clinical assessment. Therefore, it is important to be aware of the common presentations and the history to elicit important clinical information, and also appreciate how to examine the patient thoroughly in order to support or refute potential diagnoses. The heart is a complex organ, with the potential for dysfunction in the ventricular pumping mechanism, in the layers of the heart, the valves, the coronary arteries and the conduction system (Bickley, 2017). It is important to have some knowledge of the clinical investigations used in cardiac assessment—the basic tools used in the emergency department being the electrocardiogram (ECG) and blood tests including high-sensitivity troponin tests (Collet et al, 2021). If a cardiac condition is suspected, further investigations following admission may include echocardiography and diagnostic coronary angiography.
Cardiac anatomy refresher
Structure of the heart
The heart consists of four chambers: two atria and two ventricles. Deoxygenated blood flows from the venous system to the right side of the heart and enters the right atrium via the inferior and superior vena cava. From there, blood flows through the tricuspid valve to the right ventricle and then to the lungs via the pulmonary artery. Oxygenated blood then flows back into the left atrium via the pulmonary veins, and passes into the left ventricle, through the mitral valve, is expelled through the aortic valve into the aorta and is distributed throughout the arterial system (Figure 1). Pathology may occur with the chambers, the valves (stenosis or incompetence) or the aorta (Tortora and Derrickson, 2014).
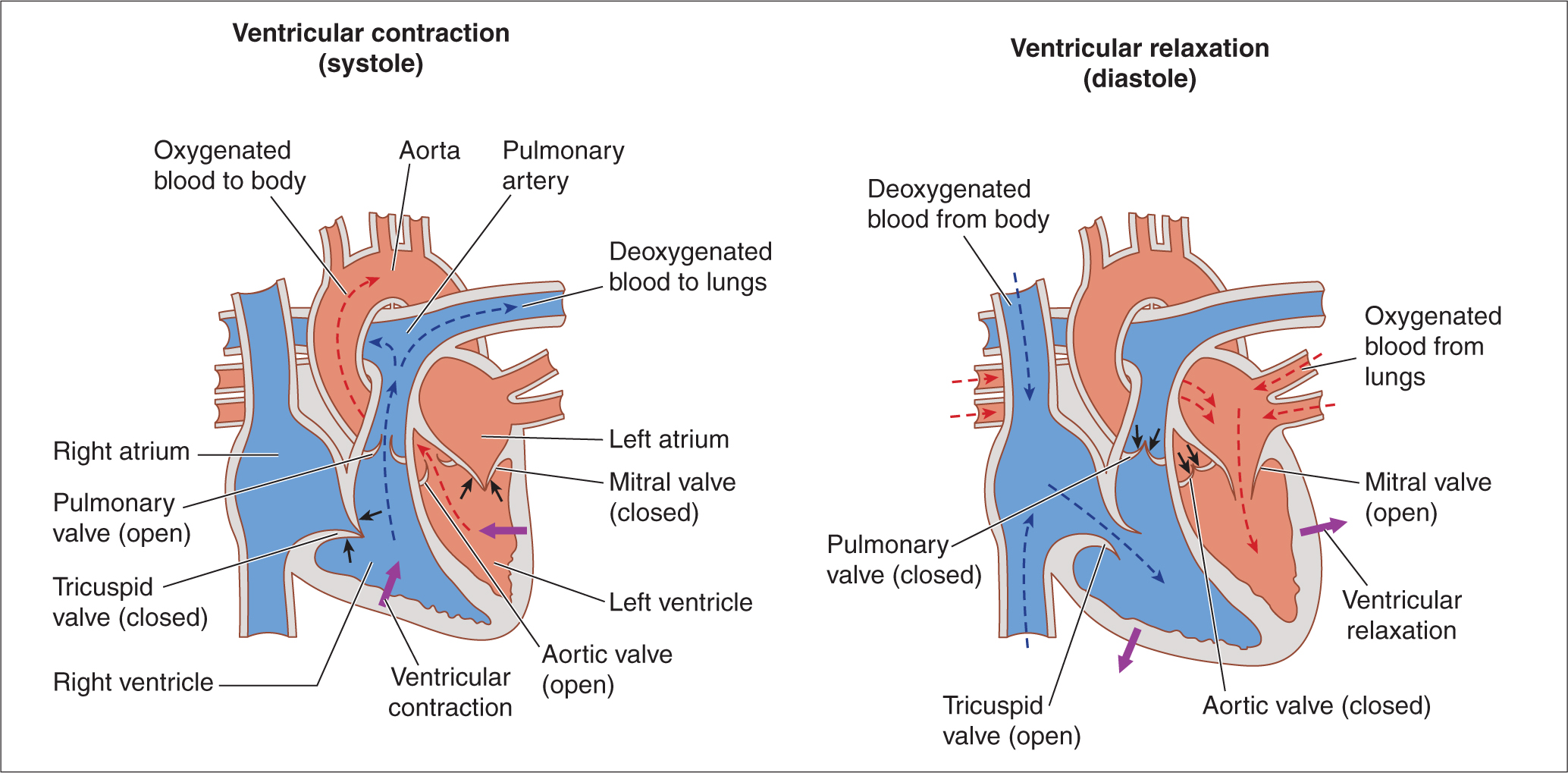 Figure 1. Blood flow through the heart
Figure 1. Blood flow through the heart
The heart is divided into three layers: the outer pericardium, a double layered semi-serous membrane, the myocardium, which contains the muscle of the heart and is responsible for pumping, and the inner endocardium. Pathology can affect any of the layers of the heart, for example endocarditis (which can cause valvular problems), myocarditis, and pericarditis (Bickley, 2017).
Blood supply to the heart
The heart is supplied with blood from the coronary arteries, arising from the aorta. Anatomy can vary, however, the right coronary artery generally supplies the inferior surface of the heart, while the left coronary artery branches from the left main stem into the left anterior descending and circumflex, supplying the anterior and lateral portions of the myocardium (Figure 2). The posterior descending artery, supplying the posterior surface of the heart, may arise from either the right or left coronary artery. Disruptions to blood flow in these arteries lead to acute coronary syndromes, including ST-segment elevation myocardial infarction (STEMI), non ST-segment elevation myocardial infarction (NSTEMI) and unstable angina (Ibanez et al 2015; Collet et al, 2021).
 Figure 2. The blood supply to the heart
Figure 2. The blood supply to the heart
Conduction system
The heart has its own intrinsic conduction system, with impulses being generated by the sino-atrial node, passing across the atria, conducted through the atrio-ventricular node, down the left and right bundle branches and into the Purkinje fibres, which infiltrate the ventricles (Figure 3). In addition, all myocardial cells can generate an electrical impulse, which in turn can initiate an arrhythmia (Bickley, 2017). Problems affecting the conduction system may manifest on the ECG or in physical signs. These include bradyarrhythmias or tachyarrhythmias, generally manifesting as palpitations, pre-syncope, or syncope (Ramrakha and Hill, 2012).
 Figure 3. The conduction system of the heart
Figure 3. The conduction system of the heart
The cardiac history
There is clearly a wide range of considerations in the history due to the variety of pathologies that can present. These will be explored in more depth in the next article, together with discussion of differential diagnosis and various tests to refute or confirm history and clinical examination. The most common presentations are outlined in this article.
There are four main symptoms that may be present due to cardiac dysfunction (Ramrakha and Hill, 2012).
- Chest pain
- Dyspnoea (shortness of breath)
- Syncope/pre-syncope (feeling faint/loss of consciousness)
- Palpitations.
Chest pain
Chest pain is an important symptom and can signify atherosclerosis of the coronary arteries, with possible acute plaque rupture leading to partial or complete occlusion of a vessel. This can lead to the spectrum known as acute coronary syndromes—unstable angina, NSTEMI or STEMI. The ECG and the use of high-sensitivity troponin blood tests will help confirm or refute this diagnosis (Collet et al, 2021).
In addition, conditions that affect the layers of the heart such as the pericardium and myocardium usually present with chest pain (pericarditis/myocarditis/myopericarditis). This is due to the presence of inflammation and possibly a degree of death of cardiac myocytes (Adler et al, 2015).
The third major cardiac cause of chest pain is aortic dissection when a tear can form in the intima of the aorta leading to blood gathering in a false lumen, which can lead to aortic rupture and sudden death. This is a differential not to be missed.
There are key questions to ask when taking a chest pain history and this is usually supported by an appropriate history-taking framework for pain, eg SOCRATES (site, onset, character, radiation, associated symptoms/signs, time, exacerbating factors, severity) or PQRST (provocation, quality, region/radiation, severity, time) (Mansbridge, 2018). In addition, the tools of ECG and blood tests to include cardiac troponins are useful in the emergency department.
Important questions to ask the patient
- What time did the pain start? (This is important for timing of subsequent testing for release of troponin, indicating myocyte damage; ask about every episode and how long each lasted).
- Where exactly is the pain? Can you point to it?
- What did/does it feel like? Heavy/ripping/tearing/sharp?
- On a scale of 0 to 10 how severe was the pain at its worst?
- Does the pain radiate anywhere? For example neck/jaw/one or both arms/back?
- Does anything make it worse? For example, exertion/change of position/taking a deep breath?
- Does anything make it better? For example, resting/leaning forward/analgesia other than glyceryl trinitrate (GTN) spray (prescribed for angina)?
- Did you feel short of breath/sweaty/nauseated, or did you vomit? Any palpitations or feelings that you were going to pass out?
The Canadian Cardiovascular Society Classification of Angina (MDCAlc.com, 2021a) may be useful in highlighting high-risk angina.
Shortness of breath
Stenosis or incompetence of valves or dysfunction of the left ventricular pumping mechanism often lead to the development of fluid overload, or heart failure, presenting with shortness of breath as the major feature (Ramrakha and Hill, 2012; Ponikowski et al, 2016). In addition, it can be a chest pain equivalent in people who may present atypically, including people with previous coronary artery bypass graft surgery or in people with diabetes (Collet et al, 2021).
Important questions to ask the patient
- How long has the shortness of breath been going on?
- Do you have the shortness of breath only when you do something or when you are sitting doing nothing?
- Are you able to wash and dress without having to stop because of shortness of breath?
- What distance could you have walked before the breathlessness started? And now?
- Did you walk in today from the car park? Did you have to stop to catch your breath? Is this normal for you? (These can be useful questions to establish if there is reduced exercise tolerance)
- How many pillows are you using in bed? Have you had to increase the number of pillows because of shortness of breath when lying flatter?
- Any waking up at night unable to breathe (paroxysmal nocturnal dyspnoea)?
- Have you noticed weight gain/swollen legs/difficulty with putting on shoes or socks?
- Have you noticed your trousers getting tight around your waist (ascites)?
The New York Heart Association Heart Failure scale (MDCalc.com, 2021b) may be useful in detecting deterioration in existing heart failure.
Syncope/pre-syncope
Cardiac arrhythmias and valvular stenosis or incompetence can both cause either near loss of consciousness (pre-syncope) or complete loss of consciousness (syncope). Cardiac syncope can signify critical valve disease, structural cardiac abnormalities (such as cardiomyopathies) or potentially life-threatening arrhythmias (Brignole et al, 2018).
Important questions to ask the patient
- Was there any warning prior to passing out?
- Were you aware of palpitations before passing out?
- Did you injure yourself?
- Did you have time to save yourself when falling?
- Any tongue biting/limb jerking/incontinence?
- Any confusion when you came round?
If there were any witnesses to the episode, they may be able to provide supporting histories.
Palpitations
Palpitations are defined as the sensation of being aware of the heartbeat. This is often benign and may be subjective and related to anxiety. However, there are some cardiac arrhythmias that present with palpitations, usually tachyarrhythmias, therefore it is important to ask the appropriate questions to elicit the relevant information (Priori et al, 2015; Bickley, 2017).
Important questions to ask the patient
- Do you feel it now? (If so, a normal ECG often reassures!)
- Were you aware of your heart racing?
- Did it feel regular or irregular?
- How long did it last?
- Can you tap it out on the table for me?
- Did it start and stop abruptly or gradually?
- Any other symptoms such as chest pain/presyncope/breathlessness or syncope?
Review of systems
In addition to the above targeted questions, it is good practice to conduct a systems review to avoid missing important information that may indicate different problems (Bickley, 2017). This involves brief inquiries about the different body systems in turn, to prompt the patient to mention symptoms.
Past medical history (including family history)
The personal past medical history (including surgical history and previous investigations) is important. Identification of common cardiac risk factors in the history is not the end. These are important and include diabetes, smoking, hypertension, previous ischaemic heart disease and family history of ischaemic heart disease. However, family history of heart disease and particularly sudden cardiac death in a first-degree relative is crucial. This is particularly useful in cases when suspecting conditions that may cause arrhythmias and sudden death, such as cardiomyopathies or long QT syndromes, as these tend to be genetically inherited (Brignole et al, 2018). Also important is any history of aortic problems or connective tissue disorders in family members, because aortic dissection may also run in families (Erbel et al, 2014).
Drug history
Check for allergies or previous adverse drug reactions. Ask about over-the-counter medication, anything bought off the internet, herbal remedies, and illicit drugs. For example, cocaine use is a risk factor for coronary artery dissection and spasm and the patient may not volunteer this information (Collet et al, 2021).
Social history
Ask who the patient lives with, and ascertain if they have any support at home/any package of care in place. It may be useful to know what kind of accommodation, for example are there stairs? The individual's occupation, smoking history and alcohol intake are all relevant to building up a clinical picture.
Examination of the cardiovascular system
Clinical examination follows the standard rules of inspect, palpate, percuss and auscultate, with the exception of percussion, which is not carried out in cardiac examination (Mansbridge, 2018). Ensure that you are in a private, warm environment. Wash your hands, introduce yourself, explain what you are going to do and gain consent to examine.
Examination starts at the end of the bed or when the patient walks in from the waiting room. Look at the patient for clues (Thomas and Monaghan, 2014).
- Look at the observation chart and medication already dispensed prior to seeing the patient
- Is the patient obviously in pain or short of breath/pale/sweaty?
- Is there any evidence of GTN spray/inhalers/sputum cartons/emesis bowls?
- Are there any walking aids/drip stands/catheters?
Expose the patient's chest. Observe for:
- Obvious deformity
- Surgical scars
- Equal and bilateral expansion
- Effort of breathing (tripoding, use of accessory muscles, intercostal recession)
- Pacemakers or other devices.
Moving to the hands and arms:
- Feel for perfusion (cold and clammy, or warm and well perfused)
- Look at the nails for finger clubbing/koilonychia/leukonychia/nicotine staining
- Capillary refill time (peripherally and centrally)
- Inspect the fingers and palms for Janeway lesions/Osler's nodes and splinter haemorrhages (endocarditis)
- Inspect for Dupuytren's contracture/palmar erythema (this can signify liver disease)
- Check for any evidence of intravenous drug use, recent venepuncture, or cannulation
- Palpate radial pulse, note regularity, character, and rate
- Check both radial pulses simultaneously to check for radio-radial delay (co-arctation of the aorta or aortic dissection)
- Check there are no shoulder problems and raise the arm, while checking the radial pulse to assess for collapsing pulse (aortic regurgitation)
- Check the patient's blood pressure (BP) if not already done. Bilateral BP can be useful in suspected aortic dissection: difference in systolic BP of 20 mmHg or more is significant. Lying and standing BP measurements can be useful to detect orthostatic hypotension.
Examine the neck and face:
- Palpate the carotid pulse
- Check for tracheal deviation
- Lie the patient at 45 degrees and observe for the pulsation of the internal jugular vein (the JVP)
- Look at the eyes for xanthelasma (periorbital yellow plaques indicating hypercholesterolaemia), jaundice or conjunctival pallor. Observe for corneal arcus (light-coloured circle around the iris signifying high cholesterol)
- Look at the face for signs of malar flush, which can indicate valvular disease
- Look at the mouth for evidence of angular stomatitis and chelitis indicating anaemia
- Look at mucous membranes in the mouth to assess hydration status and under the tongue for central cyanosis. Pallor of mucous membranes may indicate anaemia
- Look at the tongue for evidence of glossitis
- Observe the state of dentition and check for evidence of a high arched palate (one of the signs of Marfan's syndrome).
Moving to the precordium:
- The areas on the chest wall that correspond to sounds generated by opening and closure of valves and blood flowing through them are where thrills may be palpated. A thrill is a palpable murmur and signifies significant valvular disease. Figure 4 shows these areas on the surface anatomy of the chest. These areas should be palpated with a flat palm for the presence of thrills, which can be felt over the valve affected
- Feel the chest for the presence of right ventricular heave. The right ventricle sits in front of the left, and a sensation of it pushing the hand away can signify right ventricular hypertrophy
- Feel for the apex beat. This is the point of maximal impulse and should normally be felt in the fifth intercostal space, midclavicular line. If it is displaced, this may represent enlargement of the heart.
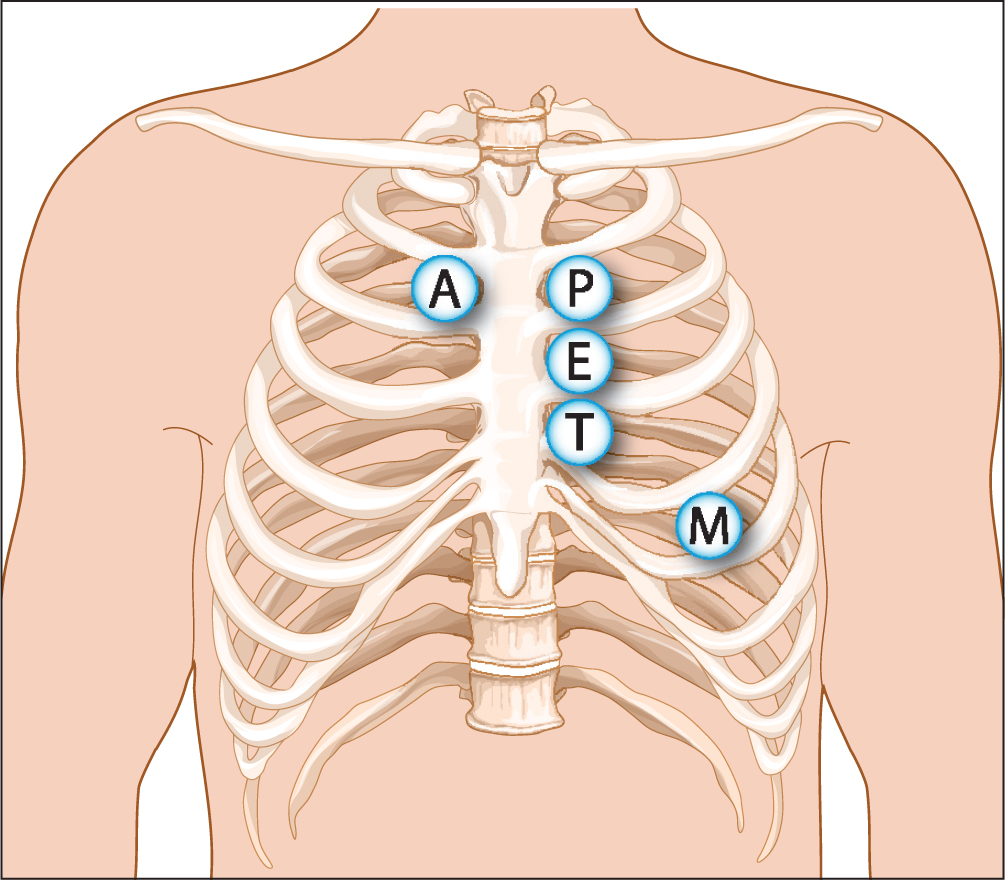 Figure 4. Areas for auscultation of heart valves: A=aortic; P=pulmonary; E=Erb's point; T=tricuspid; M=mitral
Figure 4. Areas for auscultation of heart valves: A=aortic; P=pulmonary; E=Erb's point; T=tricuspid; M=mitral
Next, auscultate the areas noted above to listen for murmurs. A murmur is turbulent blood flow across a valve and may be caused by stenosis of the valve, or incompetence of the valve causing backflow (Ramrakha and Hill, 2012).
- Check the aortic valve: second intercostal space, right sternal edge
- Check the pulmonary valve: second intercostal space, left sternal edge
- Check the tricuspid valve: fifth intercostal space left sternal edge
- Check the mitral valve: fifth intercostal space mid clavicular line (apex)
- Listen for carotid bruits
- Listen for pericardial friction rub (pericarditis)
- Listen over aorta for bruits and also over renal arteries.
Palpate all pulses:
- Radial
- Brachial
- Carotid
- Femorals (check for radio-femoral delay, aortic dissection)
- Popliteals
- Dorsalis pedis and posterior tibialis: check for pedal and pre-tibial oedema
- Check for sacral oedema.
Investigations
ECG
The major diagnostic tool in identifying cardiac conditions remains the ECG (Collet et al, 2021). It is beyond the scope of these articles to offer in-depth teaching on the ECG, however, some common ECG patterns that may be seen in clinical practice will be presented in the next article.
Bloods
Commonly the biomarker relied on to detect myocardial damage is troponin T or I. This cardiac enzyme will be detectable in blood around 3 hours from myocardial injury and can be detected with high-sensitivity assays. These are commonly called high-sensitivity troponin T (HSTnT) assays (Collet et al, 2021). Serial samples are required to demonstrate a rising pattern and confirm myocardial injury.
In addition to HSTnT, commonly requested blood tests include full blood count (FBC), urea and electrolytes (U&E), liver function tests and C-reactive protein (CRP). These are mostly useful to rule in or out other conditions that may present in a similar way, for example chest infection or cholecystitis. NT pro-BNP (N-terminal pro-brain natriuretic peptide) can be useful in diagnosing heart failure (Provan, 2018).
Chest radiogram/chest X-ray (CXR)
Most patients presenting with chest pain or shortness of breath will require a chest X-ray. This allows the clinician to consider neoplasms, infection and pneumothorax, and gives clues about potential aortic dissection and possible cardiomyopathies by revealing an enlarged heart (Provan, 2018).
Conclusion
This article has reviewed the structure and function of the heart with reference to many of the conditions that may affect this organ. In addition, the common presenting complaints of cardiac conditions have been highlighted, together with important aspects of the history for each symptom. The full cardiac examination was outlined.
The next article discusses some common cardiac conditions. These will be linked to common findings in a patient's history, examination, and investigations.
KEY POINTS
- Many different conditions can affect the heart, including coronary artery disease, arrhythmias, and disorders of the heart muscle/layers and of the aorta
- The four main presenting complaints in the emergency department are chest pain, dyspnoea, syncope, and palpitations
- Taking a thorough targeted clinical history is crucial, together with a comprehensive examination
- The main investigations to help come to a provisional diagnosis are blood tests (full blood count, urea and electrolytes, C-reactive protein and high-sensitivity troponin T), electrocardiogram and chest X-ray
CPD reflective questions
- What kinds of cardiac conditions might cause syncope and why?
- What other conditions might cause chest pain (not always cardiac). How would you differentiate?
- What are the red flag symptoms to escalate emergency treatment in bradyarrythmias or tachyarrhythmias presenting to the emergency department?