
Patients can require wound care at all ages, from infants to the elderly, and nursing practice can vary from primary or secondary care and long-term care institutions. Recent studies have recommended that wound care should be viewed as a specialism, which requires clinicians to have specialist training to diagnose and manage wounds appropriately (Guest et al, 2015). However, evidence suggests that this is not current practice. It has been recommended that effective treatment, diagnosis and prevention of wound complications could help reduce treatment costs and reduce the economic burden of wounds on the NHS (Guest et al, 2015). The estimated annual NHS cost in England for managing wounds after adjustment for comorbidities is £4.5-5.1 billion with two-thirds of this cost incurred in the community (Guest et al, 2015). The findings from this study indicated that approximately 30% of wounds lack a differential diagnosis. This could be indicative of a lack of experience by non-specialist health professionals in the community. The findings of Guest et al (2015) highlighted the need to change approaches to wound assessment and improve the quality of patient care. This has been actioned by the inclusion of wound assessment as a key indicator in the Commissioning for Quality and Innovation (CQUIN) framework for 2017-19 (Scott-Thomas et al, 2017). It is therefore essential for health professionals to improve their knowledge and skills in wound assessment.
The skin
Also known as the integumentary system, the skin is regarded as the largest organ in the body. There are two main divisions of the skin: the outer epidermis and the deeper dermis. The epidermis is made up of five layers of cells. The dermis is divided into two main layers (Figure 1). The functions of the skin are as follows (Blows, 2018):
A break in the skin caused by a wound means that these functions and barriers are temporarily lost, resulting in a disruption of homeostasis.
Acute and hard-to-heal wounds
A wound defined by Lazarus et al (1994) is a ‘disruption of normal anatomical structure and function, which results from pathological processes beginning internally or externally to the involved organ.’ Acute wounds are classified as wounds that proceed through an orderly and reparative process to establish sustained anatomical and functional integrity (Lazarus et al, 1994). The term ‘chronic wounds’ has been used for wounds that fail to proceed through an orderly, timely reparative process—these are now referred to as hard-to-heal wounds.
Stages of wound healing
Wound healing is usually described in four distinct phases, but descriptive models tend to refer to acute wounds (Figure 2). Hard-to-heal wounds do not follow a normal sequence of events and consequently delays in the healing process are experienced.
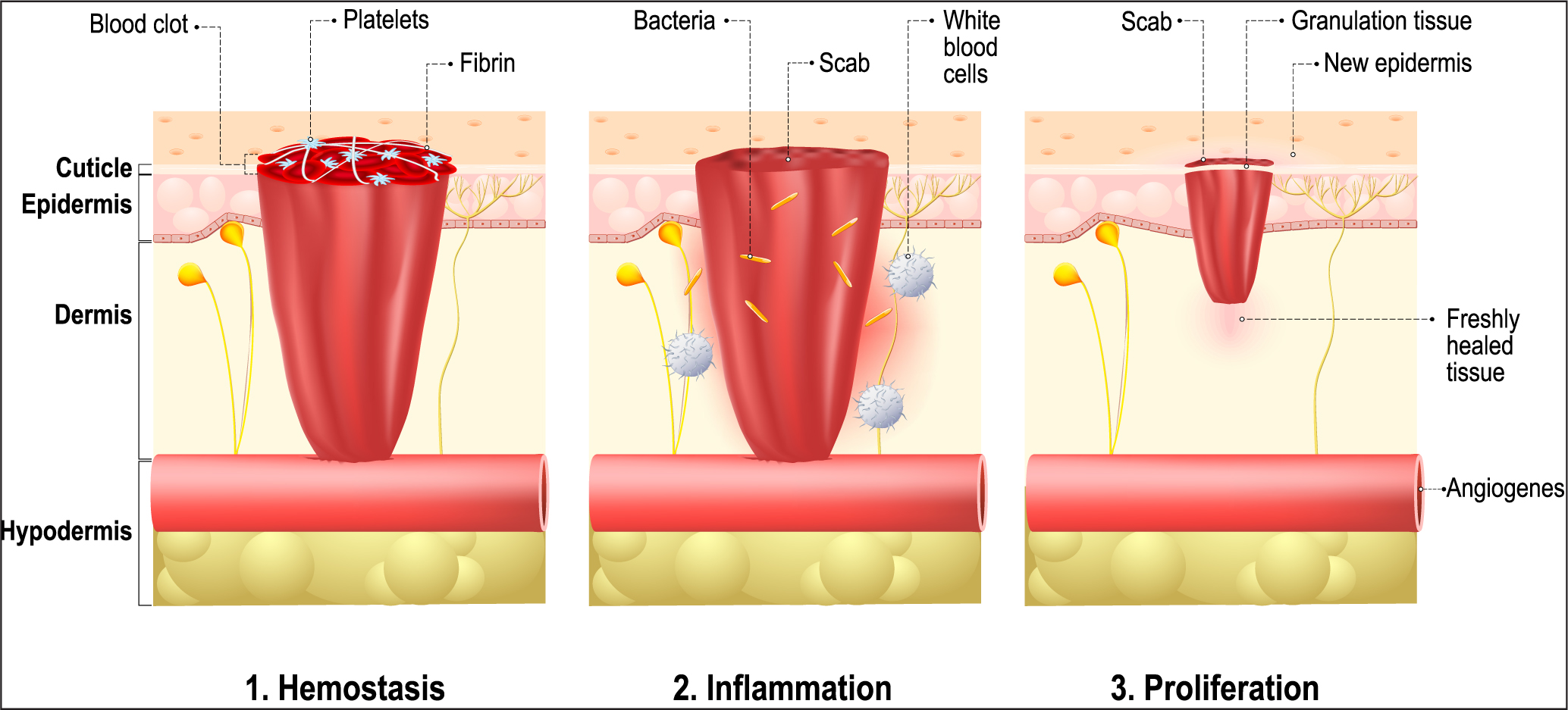
Haemostasis
Following initial wounding, blood loss is controlled by a complex series of events. The blood and lymphatic vessels undergo vasoconstriction for a short period of time to create a haemostatic plug (Nguyen et al, 2009). In addition to minimising injury, this process initiates the inflammatory phase.
Inflammatory phase
Once haemostasis has been achieved the blood vessels dilate to allow essential cells into the wound bed. The release of growth factors attracts the migration of phagocytic cells—neutrophils and macrophages. These cells' primary function is to host immune response and autolyse any bacteria or necrotic, sloughy or dead tissue within the tissue spaces (Nguyen et al, 2009). This process is known as phagocytosis. Because of increased blood flow, there is an increase in capillary hydrostatic pressure. The classic signs of this are redness and heat. The effectiveness of normal blood osmotic pressure increases capillary permeability, which leads to protein-rich fluid leaking into interstitial tissue spaces. As the fluid moves out of the capillaries the viscosity of the blood increases, slowing down the flow. As a result, red blood cells clump together forcing white cells to move towards the endothelium of the vessels and causing swelling and pain. There is an increased demand for nutrients and oxygen in the damaged area increasing the patient's metabolic rate, which raises core temperature.
Proliferative phase
The proliferation stage overlaps the inflammation stage as it starts to end. The focus of this stage is to rebuild tissue through three separate processes.
Granulation:
This leads to the formation of new blood vessels (angiogenesis), which deliver nutrients and oxygen to the healing tissues. Fibroblasts from the surrounding tissue are activated by growth factors released in the inflammatory phase. These replicate and produce a collagen-rich matrix, which builds strength and elasticity into the wound. Granulation tissue creates the appearance of a red, velvety carpet on the bed of the wound. Unhealthy granulation is characterised by a dark discolouration and bleed easily. This may be an indication of infection and poor vascular supply to the tissue (Peate and Stephens, 2019).
Contraction:
The myofibroblasts create a push/pull effect to contract the wound edges.
Epithelisation:
The wound is resurfaced by epithelial cells.
Maturation phase
The maturation phase involves remodelling of tissue to form scar tissue. This phase can take up to 2 years. Cellular activity reduces and the number of blood vessels in the wound decreases.
Assessment
A holistic wound assessment is essential to identify causative and contributory factors, support diagnosis and highlight factors that may contribute to delayed wound healing. Wound assessment is about assessing the wound bed, planning appropriate interventions, evaluating treatment and interventions and continual reassessment (Ousey and Cook, 2012). Accurate and timely wound assessment is the underpinning of effective clinical decision making, agreeing on appropriate patient-centred goals and reduced morbidity and costs associated with wound care (Posnett and Franks, 2009). Conditions such as obesity, cardiovascular disease, anaemia, respiratory disease, diabetes, renal failure, immune disorders and concurrent lifestyle factors such as smoking, mobility, nutrition and stress are important to determine how well the wound will heal (Benbow, 2016).
Assess the patient
Assessment involves gathering and interpreting information about the patient. Confirm the patient's specific requirements and reason for the assessment. A holistic assessment should include specific questions relating to the patient's health and wellbeing. This will provide clinicians with a strong foundation to manage the patient's skin and wound identifying intrinsic and extrinsic factors that may delay wound healing.
| Intrinsic |
|---|
| Oxygenation: oxygen is essential for cell metabolism and energy production. Hypoxic wounds are at increased risk of infection, reduced angiogenesis (the development of new blood vessels), reduced epithelialisation, fibroblast (connective tissue cell) proliferation, collagen synthesis and wound contraction (Guo and DiPietro, 2010) |
| Infection: once the skin is injured, micro-organisms that are normally on the skin surface access underlying tissue. Infected wounds become ‘stuck’ in the inflammatory phase. The pathogenic microbes compete with the fibroblasts for nutrients and other resources (Guo and DiPietro, 2010) |
| Venous insufficiency: increased venous pressure; over time leads to a chronic inflammatory response, which can cause the breakdown of tissue resulting in venous leg ulceration (Wounds UK, 2016) |
| Diabetes: prolonged wound hypoxia, dysfunction in fibroblasts and epidermal cells, impaired angiogenesis and neovascularisation (natural formation of new blood vessels), decrease host immune resistance and neuropathy (Guo and DiPietro, 2010) |
| Peripheral arterial disease: decreased blood flow to the lower extremities and wound, reducing the amount of oxygen and nutrients to the wound bed |
| Temperature: the cooler the wound the longer it will take to heal. Higher temperatures promote vascular dilation |
| Necrotic tissue or foreign bodies: both prolong the inflammatory response and increase the risk of infection |
| Oedema: affects the permeability of vascular membranes, inflammation or tissue trauma. Also, fluid can leak into the surrounding tissue |
| Dehydration: fluids are required for oxygen profusion, hydration of the wound bed, transportation of nutrients, as a solvent for vitamins, minerals, glucose, amino acids and to transport waste away from cells |
| Extrinsic |
| Age: skin loses its elasticity with ageing. Collagen is reduced and blood flow can be restricted due to other chronic conditions. Other factors that delay wound healing in older people are altered inflammatory response, delayed T-cell infiltration and alterations in chemokine production, reduced macrophage phagocytic capacity |
| Gender: oestrogen helps to regulate a variety of genes associated with regeneration. Older males and post-menopausal women are at a higher risk of chronic wounds (Oh and Phillips, 2006) |
| Comorbidities: conditions such as diabetes, chronic venous insufficiency, peripheral arterial disease and immune deficiency disorders are known to delay the wound healing process. Additional screening for these comorbidities in patients with wounds is recommended. In diabetes narrowed blood vessels lead to decreased blood flow and oxygen to a wound. Elevated blood sugars decrease red blood cells, which carry nutrients to the tissue, and lowers the efficacy of white blood cells (neutrophils and monocytes) to fight infection |
| Obesity: reduces the availability of oxygen to the wound. Skin folds can harbour bacteria and damage can be caused by skin-to-skin friction and increase the risk of pressure ulcer development (Mitchell, 2018). Obesity can also be connected to stress, anxiety and depression |
| Medications: steroids, non-steroidal anti-inflammatory drugs, chemotherapy—many medicines interfere with clot formation or platelet function, inflammatory responses and cell proliferation |
| Nutrition: Nutrition is required to provide adequate support for the increased energy demands during the healing process. Inadequate protein leads to skin fragility, decreased immune function and poor wound healing. The body requires 30–35 Kcal daily to heal a wound and 40 Kcal if the patient is underweight |
| Lifestyle factors: Alcoholism and smoking. Smoking causes vasoconstriction, which leads to hypoxia. Neutrophil and monocyte (cells that help prevent infection) activity are reduced and fibroblast proliferation and migration is reduced. Collagen is reduced in smokers, which means less tensile wound strength. Alcoholism diminishes host resistance making the body more at risk of infection. Decreases phagocytic function (phagocytosis is a three-stage process in which neutrophils, monocytes and macrophages engulf and destroy microorganisms, other foreign antigens and cell debris). Cytokine (small secreted proteins released by cells that have a specific effect on the interactions and communications between cells) release is suppressed and angiogenesis is reduced |
| Immunocompromised conditions: cancer, radiotherapy, AIDS. Chemotherapy and radiation can slow wound healing. Processes such as cellular replication, inflammatory reactions and tissue repair are compromised. Radiation therapy can cause permanent tissue damage |
| Stress and anxiety: stress delays wound healing by altering the multiple physiological pathways required in the repair processes (Gouin and Kiecolt-Glaser, 2011). Stressors can lead to negative emotional states, for example anxiety and depression, which have an impact on physiological processes and behavioural patterns that influence health outcomes (Guo and DiPietro, 2010) |
| Pain: ineffective wound pain management can delay wound healing and contribute to lack of concordance with treatment (Frescos, 2011) |
Assess the wound
| Type | Colour of tissue |
|---|---|
| Necrotic | Black |
| Sloughy | Yellow |
| Granulating | Red |
| Epithelialising | Pink |
| Infected | Green |
| Type | Consistency | Colour | Significance |
|---|---|---|---|
| Serous | Thin, watery | Clear, straw-coloured | Often considered normal but increased volume may indicate infection (eg Staphylococcus aureus). May also be due to fluid from urinary or lymphatic fistula |
| Fibrinous | Thin, watery | Cloudy | May indicate the presence of fibrin strands which would indicate a response to inflammation |
| Sero-sanguineous | Thin, slightly thicker than water | Clear, pink | Presence of red blood cells indicates capillary damage (eg after surgery or a traumatic dressing removal) |
| Sanguineous | Thin, watery | Reddish | Low protein content due to venous or congestive cardiac disease, malnutrition—or enteric or urinary fistula |
| Purulent | Viscous, sticky | Opaque, milky, yellow or brown, sometimes green | White blood cells, bacteria, slough or from enteric or urinary fistula. Bacterial infection (eg Pseudomonas aeruginosa) |
| Haemopurulent | Viscous | Reddish, milky | Established infection. May contain neutrophils, dying bacteria, inflammatory cells, blood leakage due to dermal capillaries, some bacteria |
| Haemorrhagic | Viscous | Dark red | Capillaries break down easily and bleed due to infection or trauma |
| Strong odour | Evident on entering the room with dressing intact |
| Moderate odour | Evident on entering the room with the dressing removed |
| Slight odour | Evident close to the patient with the dressing removed |
| No odour | No odour evident with dressing removed |
| Signs of venous disease | Signs of arterial disease |
|---|---|
|
|
|
Conclusion
Holistic wound assessment, which focuses on the patient's physical and mental wellbeing, is essential to precede effective wound treatment and management and ensuring quality patient care. Thorough, accurate and regular assessment can optimise wound healing and progression in enhance the patient's quality of life.