

Breast cancer is the most common cancer in the UK, affecting more than 55 000 people each year (Cancer Research UK, 2019). Sixty per cent of cancers are diagnosed following GP referral and 30% are diagnosed following surveillance in the NHS Breast Screening Programme (NHS England and Getting It Right First Time (GIRFT), 2021). Breast cancer incidence increases with age, with more than 25% of breast cancers diagnosed in people over 75 years of age, and fewer than 10% in those under 50 years of age (NHS England and GIRFT, 2021). In contrast, in the UK between 2018 and 2020, 2.5 breast cancers were identified per 100 000 women aged 29 years and under (National Cancer Registration and Analysis Service, 2022). This statistic generates a cancer conversion rate of 0.0025%, highlighting that those aged under 30 years are a low-risk population for developing breast cancer.
High demand for breast assessment and diagnostic resources significantly impacts delivery in primary and secondary care services, with more than 500 000 new outpatient referrals received by breast services annually in England (NHS England and GIRFT, 2021). In 2019-20, 124.9 million outpatient appointments were attended, representing a 66.9% increase from 84.2 million attendances in the previous decade (NHS Digital, 2010; 2020). One of the most attended outpatient groups includes diagnostic imaging (NHS Digital, 2020).
A patient group generating recent interest in diagnostic services are patients presenting with breast pain as their only symptom. A reason for this relates to increasing evidence that the incidence of breast cancer in women with ‘breast pain only’ symptoms reflects a low cancer incidence (0.4%) (Dave et al, 2022). Referrals for patients in this symptom group appear to disproportionately affect breast assessment services, representing over 20% of referrals (Dave et al, 2022). Management of patients referred for breast assessment with a low risk of cancer, such as those with breast pain only, has resulted in requests for new pathways to better manage these referrals (NHS England and GIRFT, 2021). The Association of Breast Surgery (ABS) has responded to this by commencing ASPIRE, a National Breast Pain Pathway Rapid Evaluation, to better understand the evidence and outcomes associated with novel breast pain pathways (ABS, 2023).
Breast referral triage pathways are acknowledged to be an effective way to identify patients at high risk of malignancy and optimise urgent appointments (Hung et al, 2006; Shetty et al, 2021). Established triage tools can provide a simple method of assessing breast referrals and can be supported by trained administrative staff (Cusack et al, 2012). Such assessment pathways can aid earlier diagnosis by identifying, assessing and diagnosing high-risk patients in clinics resourced to align with their presenting symptom and level of risk. This approach also supports the objective of the NHS Long Term Plan to improve the diagnosis of patients with breast cancer at earlier stages (NHS England/NHS Improvement, 2019).
Demand for almost all aspects of diagnostics has been rising year on year, and for some diagnostic resources demand has outstripped capacity (Richards, 2020). This increased demand has negatively impacted delivery of diagnostic waiting times standards, with subsequent effects on cancer and elective care services (NHS England, 2022).
Before this evaluation, breast symptom referrals received no established triage in the secondary care trust conducting this study. The service received annual mean symptomatic referrals of 6500 patients and mean cancer diagnosis rates of 442 patients (between 2018 and 2021). This iterative service improvement method (Shah et al, 2021) aimed to develop and adopt a combined clinical and non-clinical team collaborative breast symptom referral triage to:
This article describes the service review and quality improvement processes undertaken in the breast referral triage and assessment pathways, associated consultant nurse-led triage and assessment clinics, outcomes of the revised pathways and processes, and provides an overview of lessons learnt to support better quality care.
Method
An iterative service improvement method was used to undertake the triage service design. Distinct phases of the process were identified to facilitate testing of ideas at each stage (Table 1).
| Phase | Week(s) 1−13 | Service improvement action |
|---|---|---|
| 1 | 1 (and continuing throughout the evaluation process) |
|
| 2 | 2−3 | Standardised pathways generated with low-risk patients identified |
| 3 | 4−7 | Standardised pathway review and refinement |
| 4 | 8−12 | Standardised pathway review and refinement |
| 5 | 13 | Audit of new clinics October to December 2022 |
The first step in establishing the clinical and non-clinical collaborative breast symptom referral triage tool was to agree a process for systematic separation of ‘suspected cancer’ and ‘cancer not suspected’ referral groups, and identify patients at high risk and low risk of breast cancer. National Institute for Health and Care Excellence (NICE) guidelines recommend patients demonstrating symptoms that are indicative of breast cancer should be referred to breast assessment services in accordance with a ‘suspected cancer pathway’ (NICE, 2023). Such high-risk referrals relate to patients who are aged over 30 years with an unexplained breast lump, for example. Patients receiving suspected cancer referrals should be diagnosed, and those without cancer should be reassured, by 28 days from receipt of referral (NHS England, 2023). Patients who are referred with ‘cancer not suspected’ symptoms (also called breast symptomatic and non-urgent), should also receive a diagnosis or reassurance by 28 days from referral (NHS England, 2023). Between 1 October and 31 December 2022, 1435 ‘suspected cancer’ and ‘cancer not suspected’ referrals were received by the breast service.
Initially, the consultant nurse, breast service lead and cancer service manager discussed the proposed service improvement. Weekly collaborative meetings were then conducted with the consultant nurse, the breast referral navigator and the six administrators in the breast referral booking team for any queries to be raised, and any service improvement aims and outcomes agreed upon.
Agreeing a safe referral triage strategy and high and low risk criteria
Referrals were received under the categories of ‘suspected cancer’ and ‘cancer not suspected’. Emerging referral populations were identified and categories for safety netting established for those patients requiring urgent assessment, such as patients at risk of sepsis or who were very unwell, and those who may fall outside designated pathway groups such as children with breast symptoms, and adult patients requiring surgical or cosmetic opinion, rather than diagnostics expertise.
Identifying bespoke clinics to optimise imaging availability
A standardised pathway was developed for patients aged under 40 years, called the ‘under 40 clinic’. This clinic was aligned with ultrasound imaging only, as this is the first-line imaging modality for patients in this age group (Royal College of Radiologists (RCR), 2019).
Patients presenting with breast pain were offered clinical assessment plus imaging at a later date, as this was known to be a low breast cancer incidence symptom (Dave et al, 2022). Patients presenting with breast pain as their only symptom were also offered enrolment into the Association of Breast Surgery ASPIRE, Breast Pain Pathway Rapid Evaluation study (ABS, 2023). Exclusions to the ‘breast pain’ pathway were patients presenting with breast implants or a history of previous breast cancer, who were offered clinical assessments and the earliest possible imaging along with the ‘cancer suspected’ patients.
Eligible patients were invited to attend dedicated clinics within 2 weeks of referral and the ‘breast pain only’ group were offered imaging within a further 2 weeks, where required. In the event that a clinical breast examination identified a suspicious finding, urgent imaging was arranged in alignment with the high-risk pathway.
Both the ‘under 40’ and the ‘breast pain’ clinics were restricted by clinician availability and, when saturated, patients were offered clinic appointments consistent with standard practice prior to the evaluation study start date.
Adaptations made to triage process and clinics following iterative review
During weeks 4 to 7, the pathway continued to be reviewed weekly in regular meetings with the consultant nurse and the breast referral navigator. Any new patient groups appropriate for consideration were identified and discussed, with the rationale for service changes relating to each group discussed.
Referral triage moved to non-clinical ‘day to day’ oversight
The triage pathway was further refined in weeks 8 to 12 with day-to-day oversight moved from a clinical focus led by the consultant nurse, to a non-clinical focus, led by the breast referral navigator.
Data collection and review
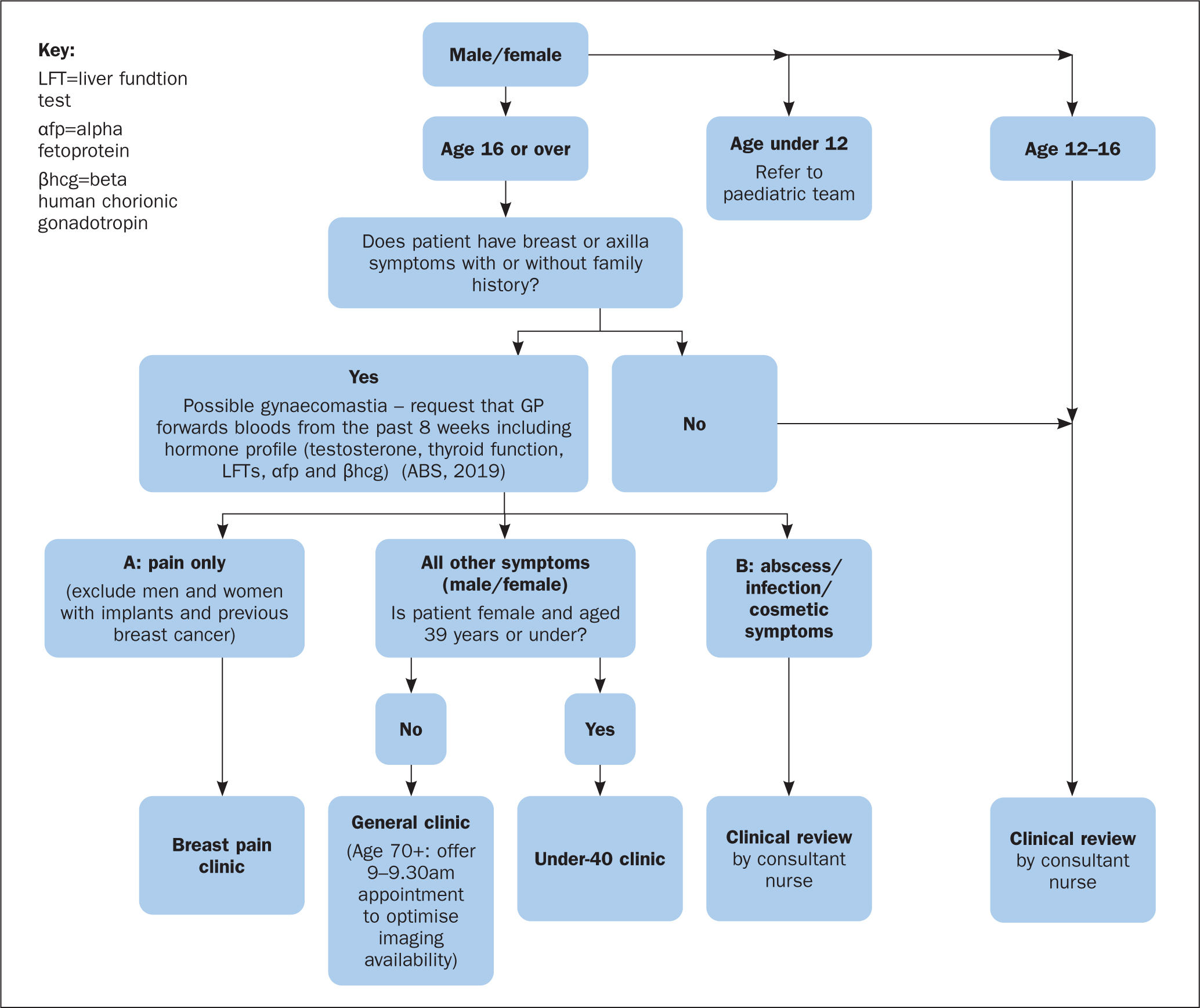
In week 13, related data were collected and reviewed, with key outcomes including for those patients whose care met the 28-day faster diagnosis standard (FDS) (NHS England/NHS Improvement 2019; NHS England, 2022) and cancers diagnosed in low-risk groups collated to evaluate the triage process, and the newly established ‘under 40’ and ‘breast pain’ clinics. Key referral categories and clinics were identified, and a flowchart developed to illustrate pathway management for each patient group (Figure 1).
Findings
The under-40 clinic
Three months of data were reviewed and a total of 126 patients were seen in dedicated under-40 clinics, with 40% referred for breast imaging (n=50/126). Same-day imaging was offered to 97.5% of those referred for breast imaging. Compliance with FDS for this group was 97.6% (n=123/126). One patient received a cancer diagnosis, consistent with a 0.79% cancer conversion rate (Table 2). Three patients were not seen within 28 days, with all three ultimately discharged and reassured. Of these three patients, one was seen on day 29 with delay due to patient illness between initial appointment and subsequent imaging. The other two patients were discharged on days 41 and 42 respectively, having both requested to reschedule two previously agreed imaging appointments.
| Number | Percentage | |
|---|---|---|
| Total number of patients | 126 | 100 |
| Faster diagnosis standard met | 123 | 97.6 |
| Imaging requested | 50 | 40 (97.5 same day) |
| Cancer diagnosed | 1 | 0.79 (cancer conversion rate) |
One 36-year-old female patient received a cancer diagnosis, following a clinical finding demonstrating an apparently symptomatic, palpable, clinically benign lump. She was offered same-day imaging and image-guided biopsy, which identified a sonographically suspicious mass. This was confirmed to be a grade 2 invasive ductal carcinoma.
This model of breast assessment was shown to facilitate higher levels of one-stop imaging provision while also allowing mammography resources to be allocated to other parts of the service, including supporting high-risk clinics, breast surveillance appointments, and to deal with any mammography backlog. High levels of 28-day alignment were achieved for this patient group. There was no evidence of cancer diagnosis delay and a low cancer conversion rate was seen, consistent with evidence relating to this younger population (NHS England and GIRFT, 2021).
The under-40 clinic was supported by an advanced practitioner who was experienced in clinical breast assessment and family history assessment.
Sixty per cent of patients were not referred for onward breast imaging assessment and this may reflect a high number of ‘cancer not suspected’ patients in this group. Imaging was arranged for clinically benign anomalies palpable on examination (graded P2), consistent with national guidance (RCR, 2019). The experience and clinical confidence of the assessing advanced practitioner may have contributed to this reduced number of onward imaging referrals, reducing pressure on imaging demand, and highlighting the value of this type of workforce.
The breast pain clinic
Three months of data were reviewed, showing 50 patients were seen in the dedicated breast pain clinic. Same-day imaging was not prioritised in this low-risk group, with 64% (n=35/50) of patients referred for subsequent breast imaging.
Compliance with FDS was 98% (n=49/50). Two patients received a cancer confirmed diagnosis, consistent with 4.0% cancer conversion rate (Table 3). Of the two patients diagnosed with breast cancer, one patient was aged 54 years and was found to have an impalpable, asymptomatic incidental 18 mm grade 2 invasive ductal carcinoma in the same region of the breast as the pain. The other patient was aged 71 years and also demonstrated normal findings on examination; however, radiologically suspicious, impalpable microcalcifications were identified on mammography in the symptomatic region. Unfortunately, this patient was the individual who breached 28-day FDS in this group. Initial imaging was received for this patient within 2 days of her initial assessment. However, her pathway was subsequently delayed due to complications after the initial mammography. She was ultimately diagnosed with breast cancer on day 37, representing a 9-day breach.
| Breast pain | Number | Percentage |
|---|---|---|
| Total patients | 50 | 100 |
| Faster diagnosis standard met | 49 | 98 |
| Imaging requested | 32 | 64 |
| Cancer diagnosed | 2 | 4.0 (cancer conversion rate) |
The breast pain clinic model of assessment delivered high levels of 28-day compliance (98%). Two patients received a cancer diagnosis, consistent with 4.0% cancer conversion rate. This is higher than would be anticipated from current evidence (Dave et al, 2022); however, the finding in this study may be misrepresentative in view of the small patient population and will be skewed by the late inclusion of patients over 50 years of age at week 8 of the evaluation. Overall, the evidence suggests that patients reviewed at breast pain clinics in this evaluation received care that was both safe and effective.
Diagnostic imaging was requested for 64% of patients, which included those assessed to have ‘focal breast pain’ with no other clinical findings (P1 on examination). This imaging referral rate reflects local guidance for P1 focal breast pain. However, it is acknowledged that local imaging recommendations can vary throughout the country for this symptom and clinical finding, and the authors await the findings of the ABS ASPIRE National Breast Pain Pathway Rapid Evaluation and other future studies, to shape practice and guidance moving forward. Currently, these findings highlight that same-day imaging may not be a suitable resource for the assessment of patients presenting with breast pain and is reinforced by findings from other related studies (Iddon and Dixon, 2013; Dave et al, 2022; Ellis et al, 2024).
Similar to the under-40 clinic model, the breast pain clinic was delivered by an advanced practitioner, experienced in clinical breast assessment, with additional expertise in breast pain and family history assessment.
During the 13 weeks of the study, the triage process was seen to change, with the needs and risks of each patient group iteratively reviewed and evaluated. Table 4 demonstrates how the triage pathway evolved with each phase of the study.
| Phase | Week(s) | Service improvement action |
|---|---|---|
| 1 | 1 |
|
| 2 | 2-3 |
Standardised pathways generated with low-risk patients identified
|
| 3 | 4-7 |
Standardised pathway review and refinement
|
| 4 | 8-12 |
Standardised pathway review and refinement
|
| 5 | 13 | Audit of new clinics October to December 2022 |
A further outcome of this service improvement was one of including daily clinical review for ‘routine’ breast referrals not seen in ‘suspected cancer’ and ‘cancer not suspected’ referral groups. Here, eligible patients, for example consultant-to-consultant referrals and patients with symptoms not aligned with ‘suspected cancer’ and ‘cancer not suspected’ criteria, were subject to daily clinical review and triaged accordingly by the consultant nurse, when indicated (Table 5).
| No breast symptoms | Breast symptoms |
|---|---|
| Breast cancer family history | *Low-risk symptoms (includes breast pain/likely cysts) |
| Breast reduction requests | *Tertiary referrals |
| Breast cancer follow-up requests | *Second opinion requests |
| NHS breast screening requests | |
| Cosmetic breast surgery |
Further improvements following breast referral triage
During the project, an additional low-risk group was identified in the under-30-years population presenting with breast ‘cancer not suspected’ symptoms. These patients were therefore prioritised into breast assessment clinics where imaging was less likely to be available. The rationale for delayed imaging was that patients would receive any required imaging within 2 weeks, through a similar pathway to the ‘breast pain only’ group and would not be disadvantaged diagnostically as their breast cancer risk was known to correlate with low incidence (National Cancer Registration and Analysis Service, 2022).
Phases 3 and 4 saw updated reviews of the breast pain clinics, and it was considered appropriate to extend the breast pain clinic group from age 50 and below to ‘all’ ages, as no disadvantage to these patients was seen in doing this.
A flowchart was developed (Figure 1) and used by the booking team for reference, to facilitate referral triage into appropriate clinics. Any patients not meeting flowchart triage alignment were flagged for daily review with the consultant nurse. This significantly reduced the consultant nurse's workload, releasing this individual for other clinical activity and further streamlining the appointment booking process.
Limitations
This study represents the experience of staff at a single specialist breast centre, with only initial findings evaluated. Further studies including larger patient numbers and of longer durations would add to the body of knowledge in this area, and current results may not be generalisable to other centres. Additionally, it is noted that the two breast cancers identified in the breast pain group were diagnosed in patients over 50 years of age, and this demographic were included in the clinic only at week 8 of the evaluation. In view of this, the cancer diagnosis rate may not be representative of the clinic under evaluation, and further study findings with more heterogenous age representation and larger patient numbers are required to better understand this group. Lastly, patient experience was not directly recorded, which would have been a valuable contribution to the findings of this evaluation.
Conclusion
The findings of this evaluation demonstrate that clinical and non-clinical service team collaboration improved service delivery in secondary care for this evaluation. This process facilitated the development of a safe referral triage strategy, including identification of high- and low-risk criteria. The value of referral triage is better understood with improvements seen in the patient pathway, and resources further optimised. These findings support NHS England's NHS Cancer Programme: Faster Diagnosis Framework, which outlines the benefit of urgent breast referral triage (NHS England, 2022).
Lessons learnt
Learning from this evaluation demonstrated that success of the triage process was interdependent with the identification and appropriate resourcing of clinics with which to align referrals. This indicates the need for wider collaboration, including radiology and non-clinical teams, in addition to booking teams, surgical and advanced practice colleagues. Since this evaluation, regular meetings with the wider service team are now in place in the authors' trust. This has enabled representatives from all areas of the FDS pathway to contribute to discussions and improvements in the pathway.
Additionally, this service change could have been improved further with more extensive co-production by including primary care and patient groups in discussion and service development, from an early stage to influence decision-making and service design.
It is recognised that the under-40 and breast pain clinics evaluated in this article were primarily supported by one individual advanced nurse practitioner, representing a single point of failure in the event of this individual's absence. Learning from this experience includes expanding provision of these clinics to the wider advanced practice and clinical team, which has since been done, to facilitate service rigour. Future planning would include business case development to secure funding, resources and training required to facilitate a sustainable and robust clinical provision of this service model.