
Wound care assessment, treatment and management are intrinsic and dynamic processes (Seckam, 2016; Wounds UK, 2018). Additionally, living with acute or chronic wounds has psychosocial consequences (Wounds International, 2012; Wounds UK, 2018). Guest et al (2015) suggested that the annual NHS cost of managing 2.2 million patients with wounds in 2012/2013 after adjusting for comorbidities was around £4.5–5.1 billion. Gray et al (2018) also proposed that expenditure might increase by more than 50% over the next 5 years. Guest et al (2017) also suggested that wound healing must increase by 1% per annum across all wound types to slow down the prevalence. If wound healing does not increase it has been estimated that an average clinical commissioning group/health board would spend £50 million on managing approximately 23 200 wounds and associated comorbidities (Guest et al, 2017). Subsequently, there are also financial implications for patients, wound care specialists and healthcare providers (Seckam, 2016). Treatment for surgical site infection in the UK has previously been estimated to cost between £814 and £6626 per patient (National Collaborating Centre for Women's and Children's Health, 2008). Hurd (2013) and Queen and Harding (2013) also highlighted the various global wound care dressing costs (Table 1).
| Traditional (gauze and absorbents) | $ 2.1 billion |
| Advanced dressings (moist wound dressings, negative pressure wound therapy) | $ 3.2 billion |
| Actives (active dressings and biological) | $0.7 billion |
| Total spend (dressings, adjuncts, beds, care time and pharmacology) | $70 + billion |
Chronic wounds pose significant financial implications for the NHS and patients themselves. In a discussion by Mudge (2015), it was suggested that the typical drivers for increased costs included the necessity of changing dressings regularly. Other factors suggested that add to the cost implications include management, duration of treatment, complications such as the presence of ischaemia, infections, neuropathy and comorbidities (Dowsett et al, 2012), therefore, it is vital to have a thorough understanding of how these costs arise if improvements are to be successfully implemented. Other costs comprise managing infections, maceration, pain and anxiety, delayed healing, and the additional nursing and hospital resources these complications consume (Guest et al, 2015). It was also reported that clinical and economic benefits were linked to an increased awareness of the impact that wounds impose on patients and the NHS and improved systems of care, which can include cost-effective and appropriate dressing selection (Guest et al, 2015; 2017).
Wound assessment and management
The skin or integumentary system is the largest organ in the body and comprises intricate and complex tissue that acts as a protective barrier between internal organs and the external environment. With ageing, skin loses its elasticity and integrity, and together with physiological changes the risk of skin-related injuries increases (Vuolo, 2009). Any tear or break in the skin is a wound; it may be attributed to physiological, mechanical and/or chemical damage and varies from superficial breaks or tears in the epithelium to deep trauma that involves muscle and bone (Vuolo, 2009). Wound healing rates vary according to the type and extent of tissue damage and patient comorbidities as well as nutrition, circulation and hydration status. Therefore, a detailed holistic assessment is essential for the management of wounds.
Exudate is the fluid leaking from a wound and plays an integral role in healing. It is predominately water and contains various blood cells (neutrophils, platelets and macrophages) nutrients, proteins, electrolytes, and inflammatory markers, protein-digesting enzymes (matrix metalloproteinases (MMPs)), growth factors, waste products and microorganisms (Cutting, 2004). Exudate is normally odourless, of a watery consistency, clear and pale amber (Vowden and Vowden, 2003). Exudate should be examined in the context of tissue type in order to administrate the correct management regime (Romanelli et al, 2010; Wounds UK, 2018).
Holistic wound assessment includes a comprehensive patient history, aetiology of the wound, condition and tissue of the wound bed and periwound area, colour, odour, type and amount of exudate. It also involves assessment of the current dressing regimen and its effectiveness at managing exudate. It should consider signs of infection, nutritional status of the patient, and psychosocial factors (Vuolo, 2009; Wounds International, 2012; Ousey and Atkin, 2013; Wounds UK, 2018). Examination of exudate is important and may indicate the components, contaminants and underlying causes, which can direct the appropriate dressing selection.
Management regimens differ depending on the cause of exudate and aim of treatment. As commented on by the World Union of Wound Healing Societies (WUWHS) (2007) if the aim is to reduce the wound moisture, one strategy would be to use an absorbent dressing capable of retaining fluid. Foam dressings in particular have been useful due to their high fluid-handling capacity, even with highly viscous exudate (BSN Medical, 2018). Conversely, if the aim of treatment is to reduce discomfort or pain, a silicone non-adherent dressing may be applicable (WUWHS, 2007). Wound care specialists are expected to choose the correct dressing in exudate management; identifying the exudate status, wound bed, dressing and surrounding skin in order to use effective strategies for achieving the desired moist wound environment in line with the patient's individual needs. There are several criteria for wound care specialists to consider when selecting an appropriate foam dressing in the management of exudate (Box 1).
The production of exudate is a normal feature of wound healing and if too much, too little or the wrong composition is produced a variety of outcomes may follow, including delayed healing, or psychosocial problems. It is therefore important to carry out a holistic assessment of the wound for effective clinical decision-making, resulting in better patient outcomes and reduction of costs, improving the overall quality of care. Posnett et al (2009) also recommended that precise and timely assessment is important in wound management, reducing costs and morbidity in addition to patient, family and wound care specialists (Wounds International, 2012).
Foam dressings
There are various foam dressings currently available on the market. Two particular dressings used to manage exudate in this study were Cutimed Siltec and Cutimed Siltec B. Both are sterile and have extra absorbency due to the addition of superabsorbent adhesive strips on the top of the foam layer, which absorb and retain exudate. The silicone wound contact layer is perforated and the outer film permeable to vapour and oxygen. In particular Cutimed Siltec B differs from Cutimed Siltec as it has an adhesive border. The dressing can be removed easily and with minimised trauma due to the silicone adhesive. The exudate is managed by the polyurethane foam core in combination with the perforations in the silicone layer. This combination allows the exudate fluid to flow vertically away from the wound thus protecting the periwound skin by reducing maceration/denudation. The top film (polyurethane) is water repellent, flexible and permeable to vapour and oxygen. Another important feature of this dressing is that clinicians and patients are able to visualise the exudate, an important indicator for dressing changes (King and Barrett, 2018). Indications for these dressings include exuding wounds, such as:
There are several different pad sizes (absorbent area) available ranging from 3.9 cm x 3.9 cm to 16.5 cm x 16.5 cm). Although the pad size is the same for Cutimed Siltec B foam dressings, the addition of the border means sizes range from 7.5 cm x 7.5 cm to 22.5 cm x 22.5 cm.
Aim of the studies
The purpose of the two studies was to observe and to evaluate the clinical performance of Cutimed Siltec and Cutimed Siltec B. Foam dressing criteria (Box 1) were considered in this evaluation including the following parameters:
Method
Two comparable studies using Cutimed Siltec and Cutimed Siltec B were carried out in Germany between November 2016 and March 2017 as well as in Germany and Poland between June 2017 and September 2017. It is important to mention that the Polish and German studies were conducted separately; however, the same protocol was used and the results pooled. One hundred and twenty nine patients agreed to participate in the study. Ethical approval was not required in Germany as this was a post-market clinical follow-up study with CE-marked products within the intended use. However, ethical approval was sought and granted in Poland (Decision Nr 24/2017). The studies were conducted under routine clinical conditions in three clinics in Poland and five in Germany. King and Barrett (2018) previously described the treatment method administered in this study. Patients meeting the criteria (Table 2) were informed in detail orally and by help of a written patient information and were enrolled onto the study after giving informed consent. The first dressing was then applied.
| Inclusion criteria | Exclusion criteria |
|---|---|
|
|
|
All clinicians involved in this study were informed regarding the dressing attributes, changes and evaluation process. During first dressing application and dressing changes evaluation forms containing non-identifiable patient information were completed. Important information gathered and recorded included:
A Likert scale (0–10 point) was used to measure pain, where 0 was ‘no pain’ and 10 was ‘worst possible pain’. Pain scores for this cohort were recorded generally and on dressing removal. Other considerations included ease of dressing removal, described as either traumatic or atraumatic removal. Skin reactions after dressing removal were documented focusing on redness, itchiness, rash and blisters.
Statistical analysis
The data generated were analysed using a mixture of descriptive and inferential statistics using SPSS software. As the same protocol was used for both the German and Polish studies, the data were combined together (pooled) for analysis. All data were summarised using frequency and percentages for the various clinical performance of Cutimed Siltec and Cutimed Siltec B and parameters collectively. A chi-square statistic was used to test whether there were changes in the distribution of exudate levels at each time period. In addition, chi-square statistics were used to assess differences in perceived amount of pain and wound margins between the initial time point and final time point.
Results
The results presented here were pooled from both the German and Polish cohorts. One hundred and twenty-nine patients—78 male (60%) and 51 female (40%)—took part in this study. Fifty-two (40%) of the cohort were aged between 18 and 65 years and 77 (60%) were over 65 years of age. In all, 150 wounds from 129 patients participating in these studies were treated with the Cutimed Siltec and Cutimed Siltec B dressings. The dressings were used to treat various wound types (Table 3) with the majority of wounds (141/94%) located on the lower body, foot or ankle.
| Wound type | Number of wounds |
|---|---|
| Diabetic ulcer | 46 (31%) |
| Venous ulcer | 51 (34%) |
| Surgical wound | 18 (12%) |
| Vascular ulcer (head, neck or torso) | 9 (6%) |
| Pressure ulcer | 6 (4%) |
| Cut/abrasion | 3 (2%) |
| Other | 17 (11%) |
Two patients died during the evaluation period for reasons unrelated to the dressing product. Taking into account the wounds on these patients, and some missing data, four wounds were excluded from the analysis so the final figures consider a total of 146 wounds.
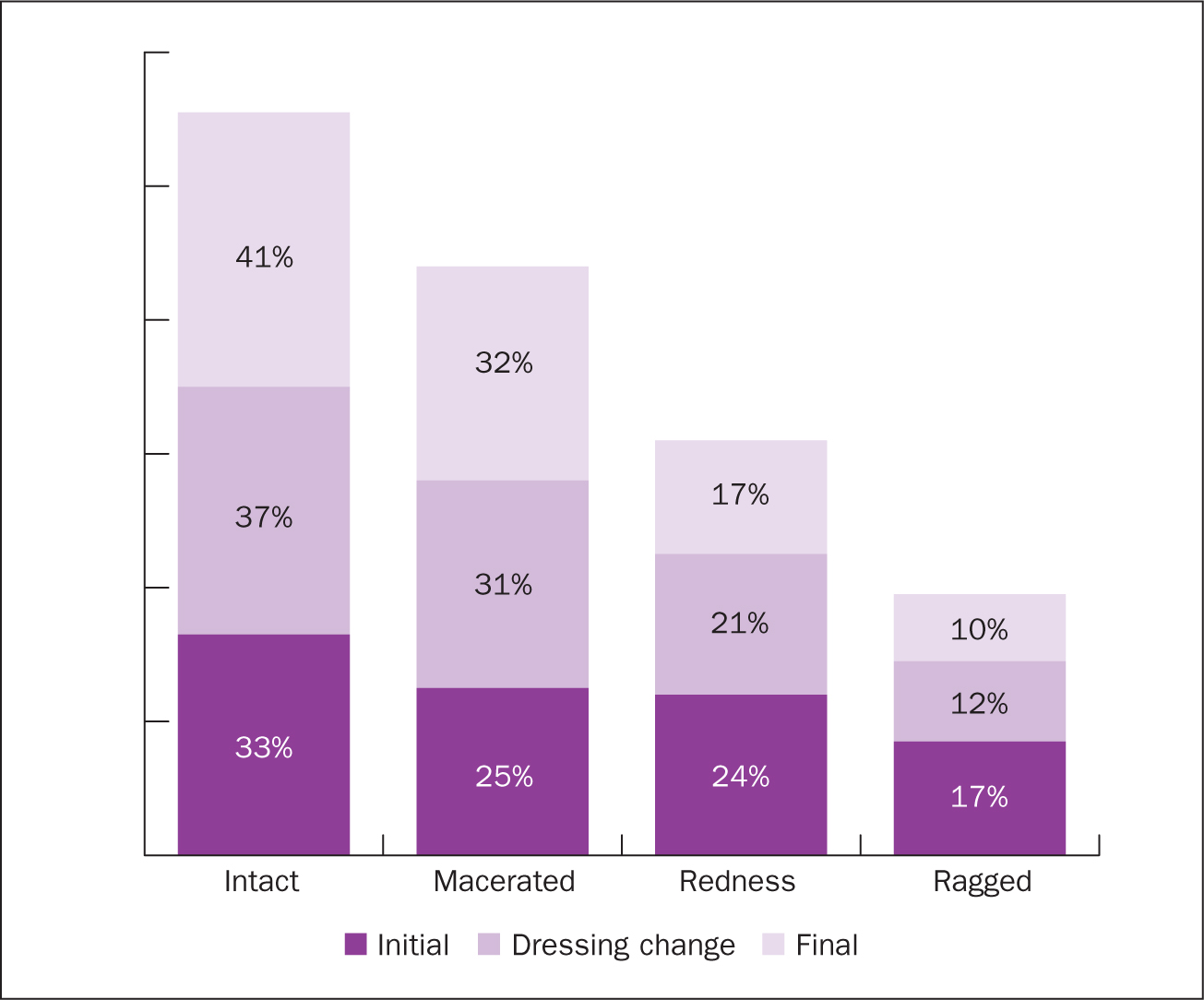
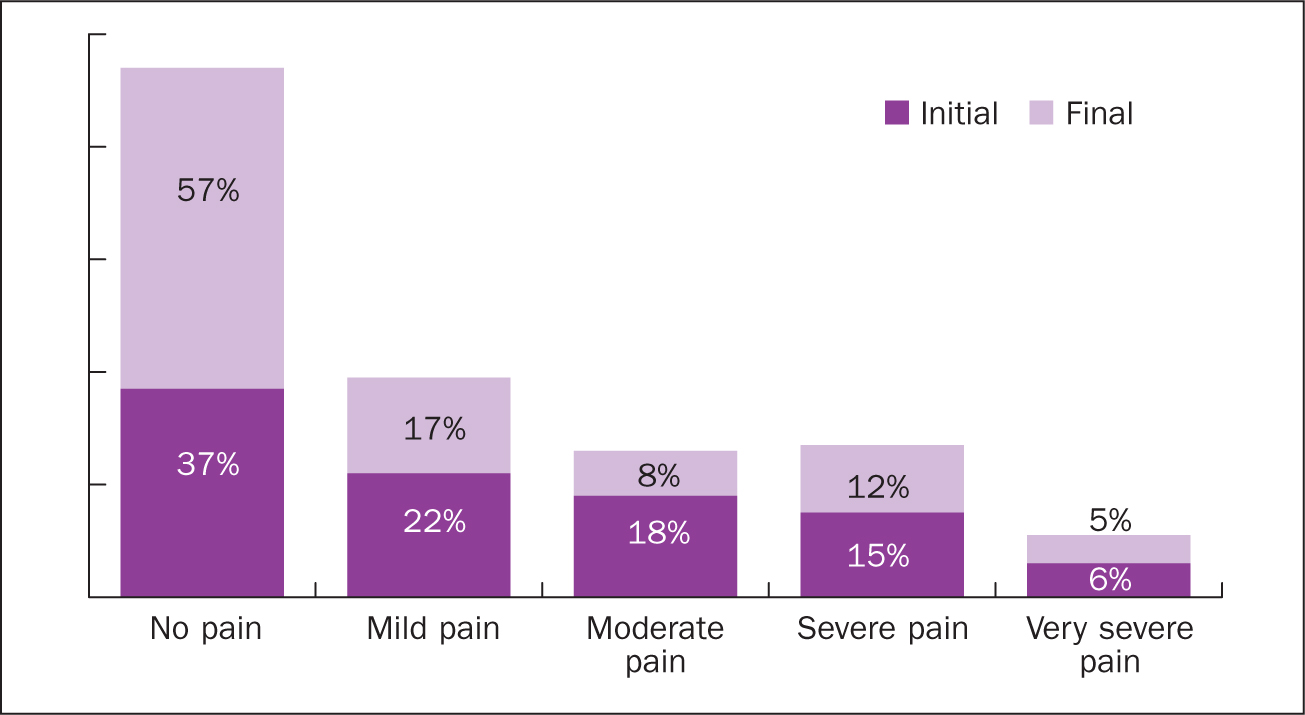
Low to moderate exudate was reported amongst these patients at each time point (Figure 1), with a decrease in moderate exudate during the dressing change visit and final visit. During the period of this study wound margins became more intact, less ragged and there was a decrease in redness (Figure 2). There was a statistically significant improvement (chi=15.28, p=0.009) in patients' general pain levels and during the initial and final dressing changes (Figure 3). There were no other statistically significant differences for exudate or margins.
In the evaluation of the product parameters, the majority of clinicians rated these as ‘good’ to ‘very good’ (Table 4). The majority of clinicians (>51%) rated the product as very good in terms of wearing comfort, ease of application, ease of removal, and adaptation to affected body. Over 90% of clinicians rated the product as ‘very good’ to ‘good’ on each parameter with the exception of absorption capacity (79%) absorption capacity under compression (87%) and retention capacity under compression (86%).
| Parameter | Very good | Good | Satisfactory | Sufficient | Insufficient |
|---|---|---|---|---|---|
| Wearing comfort | 89 (61%) | 48 (33%) | 3 (2%) | 4 (3%) | 2 (1%) |
| Ease of application | 88 (60%) | 53 (36%) | 3 (2%) | 1 (1%) | 1 (1%) |
| Ease of removal | 92 (63%) | 52 (36%) | 1 (1%) | 1 (1%) | 0 (0%) |
| Absorption capacity | 71 (49%) | 44 (30%) | 19 (13%) | 7 (5%) | 5 (3%) |
| Retention capacity | 49 (39%) | 47 (38%) | 17 (14%) | 6 (5%) | 6 (5%) |
| Adaptation to affected body part | 77 (52%) | 56 (38%) | 11 (7%) | 1 (1%) | 2 (1%) |
| Absorption capacity under compression | 38 (66%) | 12 (21%) | 4 (7%) | 2 (3%) | 2 (3%) |
| Retention capacity under compression | 36 (62%) | 14 (24%) | 4 (7%) | 2 (3%) | 2 (3%) |
The majority of clinicians' overall satisfaction (96%) and fulfilment of expectation (93%) were rated as satisfactory or above (Table 5). Clinicians also rated the product above satisfactory for overall satisfaction: 85% rated the product as good to very good. Similarly, with respect to fulfilment of expectations, 79% of the clinicians who rated the product at satisfactory level or above rated it as good to very good.
| Very good | Good | Satisfactory | Sufficient | Insufficient | |
|---|---|---|---|---|---|
| Overall satisfaction | 65 (45%) | 59 (40%) | 16 (11%) | 4 (3%) | 2 (1%) |
| Fulfilment of expectations | 63 (43%) | 53 (36%) | 2 (14%) | 4 (3%) | 5 (3%) |
Discussion
One hundred and twenty-nine patients took part in this study with 150 wounds being treated over three dressing changes. From the results observed the use of these dressings proved beneficial exudate management (Figure 1) with a decrease in medium exudate among this cohort of patients. These findings suggest that these foam dressings were useful in the management of medium exudate in line with the criteria outlined in Box 1, when selecting an appropriate foam dressing (WUWHS, 2007; Romanelli et al, 2010). There was also an increase in intact wounds with a decrease in redness (Figure 2). There was a significant decrease in reported pain from the initial visit to the final visit (Figure 3). Patients often suffer psychosocial implications (Wounds International, 2012) because of the various wound elements mentioned previously, thus the results presented here highlight the importance of pain management during dressing changes. A decrease in wound pain during dressing changes may be linked to atraumatic removal. Further investigation into the decrease in general pain is required. The findings support the use of Cutimed Siltec and Cutimed Siltec B in wound exudate management and wound care management in general.
As outlined by the WUWHS (2007), if the aim is to reduce the wound moisture, one strategy would be to use an absorbent dressing capable of retaining fluid, or the addition of a higher absorbency secondary dressing. Alternatively, if the aim of treatment is to reduce discomfort or pain a silicone non-adherent dressing may be applicable (WUWHS, 2007). The results demonstrated here address both of these aims without the use of a secondary dressing. The parameters and criteria when using Cutimed Siltec and Cutimed Siltec B foam dressings both meet those criteria outlined by WUWHS (2007) and studies presented by Romanelli et al (2010) and King and Barrett (2018).
The majority of clinicians' and patients' perspectives on the evaluation of the foam dressing parameters (Table 4) wearing comfort, ease of application and removal, absorption and retention capacity, adaptation to affected body part, absorption and retention capacity under compression were rated good to very good. Again, these findings parallel those criteria highlighted by WUWHS (2007)Romanelli et al (2010) and King and Barrett (2018) and are in line with the Best Practice Statement published in 2018 (Wounds UK, 2018). Qualitative data also revealed that clinicians found these dressings useful in practice:
‘Atraumatic … good due to high absorption capacity and fluid retention … did not irritate the skin or cause maceration’.
These comments align with and support those suggested by King and Barrett (2018).
Conclusion
This article builds on the evidence presented by King and Barrett (2018) in the evaluation of the absorbent silicone adhesive foam dressing on 20 wounds over three dressing changes. In this study 150 wounds were treated across multiple sites in Germany and Poland. Together these findings parallel, complement and add to the growing body of evidence in support of using the Cutimed Siltec and Cutimed Siltec B absorbent dressings. Positive attributes of using these dressings included ease of use, ease of dressing removal, exudate handling, conformability of the dressing and the ability to reduce pain on application and removal and during wear. Cutimed Siltec and Cutimed Siltec B are most suitable for up to moderately exuding wounds, however, for heavily exuding wounds these dressings may require regular changes or the use of dressings more suitable for managing heavy exudate.
These findings, together with the growing body of evidence, support the use of foam dressings as an alternative to those currently being used. Future wound care studies should also include in vitro testing of the Cutimed Siltec and Cutimed Siltec B foam dressings in terms of absorption and retention capacity under simulated compression conditions, longer follow-up periods and time to complete healing.