

In healthcare, practice change focuses on replacing low-quality, ineffective interventions with evidence-based practice (EBP) to improve efficiency and support improved patient outcomes. Healthcare organisations encourage employees to attend conferences and become educated about innovative technologies. However, new technology adoption can be overwhelming without the knowledge and tools necessary to support EBP implementation. Moreover, the realities of organisational challenges in healthcare can quickly stifle the EBP implementation process. This article proposes a clinical technology implementation model that can help nurse managers implement technology that aligns with EBP, drawing on experience from the adoption of a near-infrared vein visualisation tool (AccuVein AV500) to support EBP and enhance peripheral intravenous catheter (PIVC) placement, in a large US hospital system, which covers three separate hospitals: Swedish First Hill, Swedish Cherry Hill and Swedish Issaquah in Washington state.
EBP for PIVC placement
PIVC placement is the most common invasive procedure performed in acute care, with up to 90% of patients requiring intravenous therapy (Alexandrou et al, 2018; Jones, 2018; Marsh et al, 2021). PIVC annual sales exceed the estimated number of people in the US, 350 million, with approximately 37 million hospitalised patients, equating to 10 PIVCs per patient admission (Steere et al, 2019). Evidence shows that patients who require three attempts or more to insert a PIVC consume 43% of total IV placement costs, and premature PIVC removal is estimated to cost between US$9.8 and US$17.5 billion annually (£7.7 and £13.7 billion) (Goff et al, 2013; Glover et al, 2017; Hallam et al, 2020).
The Infusion Nurses Society (INS) has published Infusion Therapy Standards of Practice and update them regularly (Gorski et al, 2021; Nickel et al, 2024). The deviation from INS practice standards for PIVC placement can result in multiple PIVC attempts, catheter failure, and/or premature removal or dislodgement, contributing to treatment delays and an extended length of hospital stay (Berger et al, 2022; Santos-Costa et al, 2022). The frequency of the PIVC procedure may contribute to a level of acceptance for insertion failure as just a routine part of IV access (Helm et al, 2019). First attempt success can be as low as 50% (Parker et al, 2017). Additionally, PIVC premature failure rates range from 35% to 50% (Alexandrou et al, 2018; Rickard et al, 2018; Nickel, 2019). Common complications associated with outdated PIVC placement techniques include infection, pain and phlebitis (Keleekai et al, 2016; Nickel, 2019; Marsh et al, 2021). Multiple PIVC placement attempts can lead to vessel depletion and require clinically excessive use of advanced vascular access devices (such as midlines and central venous catheters), which have an increased risk of infection, morbidities, and mortality (van Loon et al, 2016; Morrell, 2020).
Limited compliance with EBP guidelines
INS recommendations for PIVC placement include vessel and site selection assessment, standard precautions with aseptic non-touch technique (ANTT) for site preparation, a disease and patient history review, and infusate therapy confirmation. New to INS standards in 2021 and continued in the 2024 edition is the need for vessel visualisation, using supportive technology to end the historical practice of blind insertions and palpation of the site during insertion, which negates ANTT practice (Gorski et al, 2021; Nickel et al, 2024).
For PIVC placement, the lack of implementation of EBP is complex, with several contributing factors. One factor is the limited education and opportunities to practise for nursing students and newly graduated nurses and a lack of consistent education for staff working in healthcare institutions (Hunter et al, 2018; Nickel, 2019; Vandenhouten et al, 2020). Up to 60% of nurses do not receive adequate PIVC education or the opportunity to practise in nursing schools (Lyons and Kasker, 2012; Vizcarra et al, 2014), which has created a knowledge deficit in clinical practice (Simonetti et al, 2019; Etafa et al, 2020). One concerning consequence of this knowledge deficit is a lack of adherence to ANTT by nursing staff, which contributes to site contamination, increasing the risk of PIVC infection (Helm, 2019; Nickel, 2019). New nurse graduates often rely on employer-based training to gain proficiency (Nickel, 2019). In US employer-based training, the responsibility to teach PIVC placement usually falls on the staff nurse preceptor, who likely has a concurrent clinical patient workload. Hospital policy and procedures likely adhere to current EBP standards; however, evidence suggests that these standards are often not universally implemented.
Nurse staffing shortages, attributed to an ageing workforce and the impact of the COVID-19 pandemic, have significantly impacted EBP implementation (Buchan et al, 2022). In the US, shortages have increased the use of agency nurses, who may have limited organisational orientation, which can lead to inadvertent PIVC practice variance (American Hospital Association, 2022). In summary, the combination of a lack of standardised education, a severe global staffing shortage in healthcare, and a deeply embedded culture of care whereby it is considered acceptable to fail half of the time with PIVC placement, highlights the challenges of widespread implementation of PIVC EBP guidelines.
A near-infrared technology solution
AccuVein AV500, a near-infrared (NIR) vein visualisation technology, is devised to assist and improve PIVC placement. AccuVein AV500 NIR technology illuminates the superficial venous system, easing assessment and efficient site selection, thereby promoting optimal PIVC placement (Sánchez-Morago et al, 2010; Zhang et al, 2022). The INS standards (Nickel et al, 2024) recommend the use of AccuVein AV500 vein visualisation technology to assess peripheral venous sites and facilitate more informed decisions about vein selection (for example, bifurcating veins, veins with tortuosity, palpable but non-visible veins, location of venous valves), primarily in paediatric and adult populations with difficult intravenous access. Additionally, the Emergency Nurses Association and the Association for Vascular Access recommend using vein visualisation technology (Parker et al, 2017; Pitts and Ostroff, 2019). NIR technology, such as the AccuVein AV500, offers benefits that extend beyond vein visualisation, allowing for assessment of vein quality, blood flow, refill speed, and identification and avoidance of valves; all critical criteria for successful PIVC placement (Kaur et al, 2019). Avoidance of valves can result in improved PIVC patency, a reduced need to replace the PIVC prematurely, and increased patient satisfaction (Çağlar et al, 2019; Eren and Caliskan, 2022).
Incorporating AccuVein NIR technology into routine pre-insertion assessment for PIVC placement has been shown to increase nurses' confidence with PIVC placement, increase first attempt success rates, decrease total procedure time, and decrease escalation calls for ultrasound-guided PIVC insertion by certified professionals (Delvo Favre et al, 2014; Guillon et al, 2015; Demir and Inal, 2019; Eren and Caliskan, 2022; Yılmaz et al, 2022). Using technology that allows for vein visualisation and assessment before PIVC placement brings clinicians closer to adhering to EBP standards. Furthermore, using AccuVein NIR technology during the PIVC placement procedure can enhance adherence to ANTT and avoid site contamination by removing the need to palpate the site during insertion.
AccuVein AV500 NIR technology does not negate the need for structured education on PIVC placement or opportunities to practise the skill. Instead, AccuVein NIR vein visualisation technology can support adherence to EBP guidelines and advance PIVC placement practices. Nurse managers are uniquely positioned to drive the adoption of EBP technology such as the AccuVein AV500. However, it can be challenging to make a compelling business case to hospital leadership that would harness the necessary support to facilitate a much-needed change in practice. A technology implementation model that incorporates wisdom from change theory and implementation science is presented in the next section. This model can be used by nurse managers to disrupt clinical practice and implement technology-based EBP changes.
Clinical Technology Implementation Model
The Clinical Technology Implementation Model (CTIM©) was developed based on the following:
- An evaluation of implementation science and change theory and
- Experience from the implementation of EBP in a large US hospital system to improve PIVC placement with AccuVein NIR technology.
The CTIM is founded on the nursing process (Ballantyne, 2016) with four key stages as follows:
- Assess
- Plan
- Implement
- Evaluate/expand.
Each stage aligns with a phase. Phases 1, 2, and 4 are based on Lewin's change management theory (Lewin, 1951) and Phase 3 is based on Betty Neuman's nursing theory and systems model (Ahmadi and Sadeghi, 2017; Verberk and Fawcett, 2017; Gonzalo, 2023). Within each phase, practical steps for implementation are also outlined (see Figure 1).
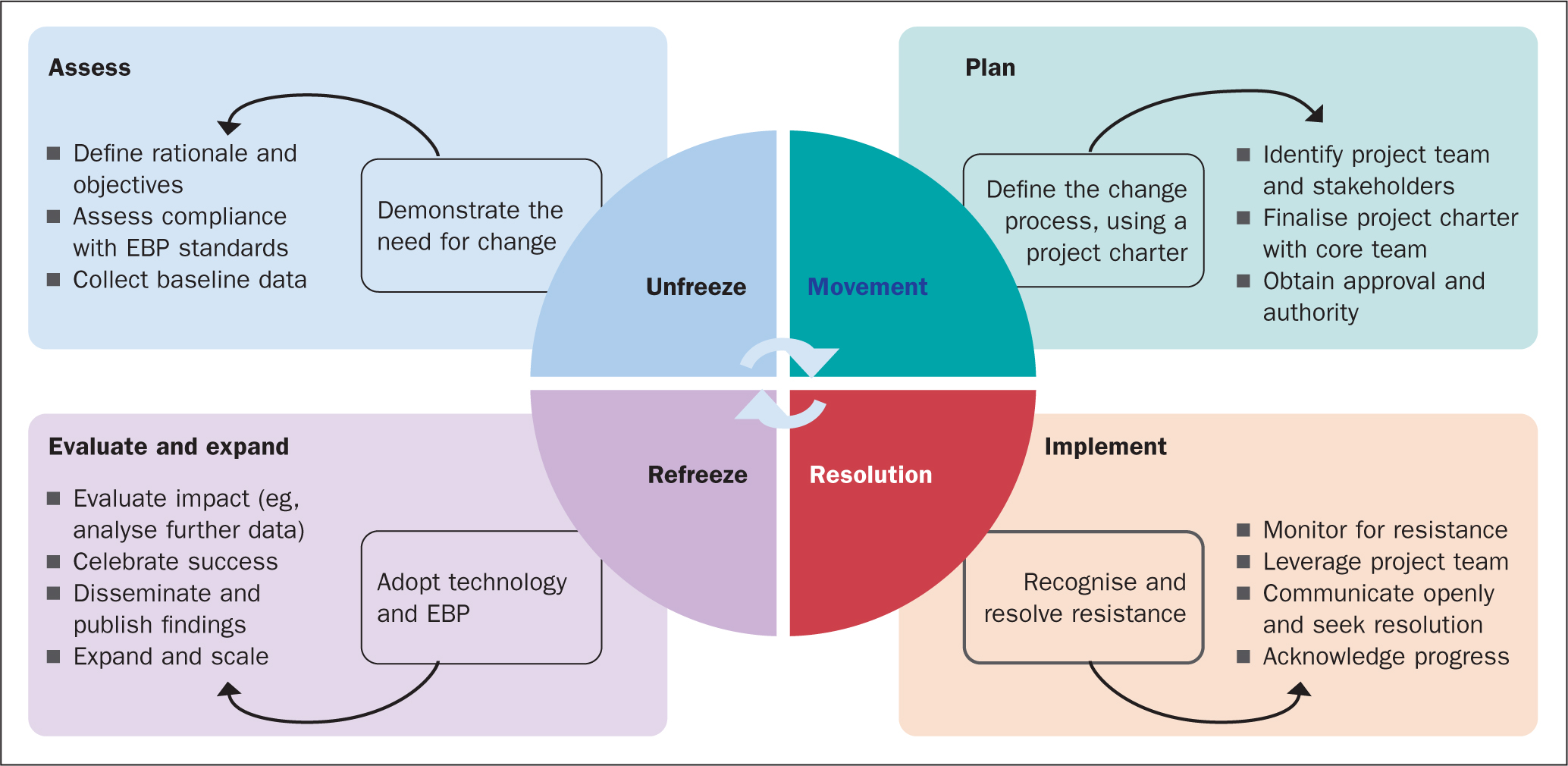
Four phases of the CTIM
Lewin defined three phases of change as unfreezing, movement, and refreezing (Petiprin, 2020). In the unfreezing phase, team stability must be disrupted to allow for old behaviour to be discovered and discarded, allowing for new information to be adopted into practice by the team. This process requires group-level involvement, which is often overlooked when attempting to change group performance (Schriner et al, 2010). In the case of PIVC placement, INS guidelines support the identification of practices to discard. Practice standardisation and implementing the evidence to improve patient outcomes is the goal.
The movement phase involves the identification of the plan for change and necessary implementation strategies. It is crucial to address the positive force pushing for change and the opposing force resisting change (Schriner et al, 2010). Nurses are regulated by administrative and facility policy, which can increase resistance to change. The change proposal must meet the standards of EBP, leading to better patient safety and outcomes. These standards help rationalise the proposed change and balance the resistance to promote the change. Maintaining a focus on patient outcomes and employee satisfaction underlines desirable innovation components and will support successful integration (Kotter et al, 2021).
The resolution phase is based on Neuman's nursing theory and systems model (Gonzalo, 2023), offering a new perspective in understanding personal response to change. The resolution phase addresses change resistance on an organisational and personal level. Organisational change can be implemented by administration via policies and penalties. Change implementation on a personal level must address a person's relationship to stress – a concept important to understand and account for when implementing a change in practice. Change, even for personal or professional improvement, causes stress. Stress is subjective and can be interpreted as a threat, resulting in the individual, or a team, feeling out of control. In Neuman's theory, each person is considered an open system that responds to environmental stressors. Neuman explains that the individual includes a resistant core; this resistance is a protective mechanism. As stressors break through this core, resistance is activated, moving an individual from wellness to illness on a continuum. It takes energy to break the core and additional energy to regain equilibrium. Resolution of change resistance focuses on identifying and recognising stressor defence as a protective mechanism in reaction to stress. This defence mechanism is a pivotal contributor to resistance to change, which is a significant factor in the failure of EBP implementation (Tucker and Mazurek Melnyk, 2019).
The final phase is Lewin's refreezing phase, which occurs when the change is implemented, developed into policy, and adopted by the team as a standard practice (Schriner et al, 2010). In this phase, equilibrium is established, and the new practice is internalised. Recognition and rewards play a significant role in this final phase to offer perspective related to the changes made and the benefits achieved. Utilisation of data to demonstrate improved patient outcomes helps to solidify the new EBP change. No effective process change occurs immediately, nor does it happen in a vacuum. Therefore, effective change will require continuous inquiry and communication to refreeze the new desired behaviour, with the team agreeing to commit to change and standardise the practice.
The CTIM phases provide a theory-based, practical model for implementing a technology-based change in clinical practice. The integration of concepts and understanding from Lewin's change theory provides a clear pathway to remove old and ineffective behaviours and practices by unfreezing, creating movement to introduce the new EBP behaviour, and refreezing. The addition of Neuman's theory ensures that the change leader recognises that resistance to change is a natural defence mechanism within the organisation's members, rather than an act of obstinance or personal affront. This will enable the change leader to recognise and support staff as they struggle through the complexity of emotions such as fear of role change, job loss, or inability to perform.
Four steps of the CTIM
The CTIM incorporates practical steps to achieve unfreezing, movement, resolution, and refreezing. The steps can be categorised as follows:
- Demonstrate the need for change
- Define the change process, using a project charter
- Recognise and resolve resistance and
- Adopt technology and EBP.
The implementation step remains the most challenging due to the involvement of numerous stakeholders, constantly changing hospital practices that increase resistance to change, and the lack of commitment to institutional sustained change in the systems and culture (Tucker and Gallagher-Ford, 2019). EBP system-wide implementation models include the Advancing Research and Clinical Practice through Closer Collaboration (ARCC) Model and the Integrated Promoting Action on Research Implementation in Health Services Model (Mazurek Melnyk et al, 2021; Tucker et al, 2021).
Step one: demonstrate the need for change
Unfreezing the ineffective processes requires recognition of ineffective and inefficient practices. A clear definition of the problem and clear objectives will help to demonstrate the need for change (Centers for Disease Control (CDC), 2006). Taking PIVC placement as an example, it is likely that a strong sense of urgency is already present in the organisation – central line-associated bloodstream infections (CLABSI) are rising (Fakih et al, 2022), and patient satisfaction is lacking (Morrell, 2020). Healthcare providers are concerned about treatment delays related to a lack of timely PIVC placement (Witting, 2012), and nurses are frustrated with repeated PIVC failure (Platt and Osenkarski, 2018). Hospital administration is concerned with economic impact along with patient and provider satisfaction, which is affected by delays in care (Morrell, 2020). This ‘perfect storm’ creates an opportunity for change to improve care for patients, clinicians, and the system.
In the case of PIVC placement, this backdrop provides a compelling rationale and allows the change leader to set clear objectives that are culturally aligned with the vision of the healthcare organisation. Furthermore, there is ample evidence indicating that the practice change in PIVC placement will positively affect patient outcomes (for example, first attempt success, reduced procedural time and dwell time) and improve employee satisfaction through reduced nursing time (McNeely et al, 2018; Zhang et al, 2022).
Assessing compliance with EBP guidelines and collecting baseline data: This will further serve to unfreeze and support the need for change. For PIVC placement, comparing your organisational findings to the INS standards will further demonstrate the need for a change in practice. Collecting organisational data for PIVC placement may be challenging. For example, historically, the number of PIVC placement attempts are not documented and understanding the average number of PIVCs or attempts to place PIVCs per patient per hospital stay will likely rely on manual prospective data collection and analysis. Collecting baseline institutional data, and supplementing that with analysis of current evidence from the literature, may be a good workaround. For analysis of institutional data, it is recommended that a sample of the hospital population be used for generalised projections (Banerjee and Chaudhury, 2010). Using a random sample will provide the most statistically sound baseline. For PIVC placement, this can be achieved by securing the daily admissions report, randomly selecting individuals from a similar population, and reviewing the number of PIVCs they have had during their hospitalisation. Cost estimates can then be determined when these numbers are multiplied by the cost of supplies, nursing time, and care delay, to support the financial objectives of the EBP change.
Another sampling method is to select several specific clinical units. Using a purposeful sample such as this can introduce bias and is not considered as statistically sound as a random sample. However, a purposeful sampling method is beneficial as it allows for cultural and social understanding regarding the practices within a specific unit. Furthermore, it can allow for better comparative data pre- and post-implementation of the change initiative. Of course, the availability of data, time and resources for each project will need to be considered when determining the data collection approach.
Step two: define the change process, using a project charter
A project charter provides an excellent framework to achieve movement in leading an EBP change. It will allow the change leader to organise and focus the change implementation and is a crucial tool for the successful implementation of new clinical technologies in a healthcare organisation. The project charter will set out the five main steps of the project (see Figure 2) (Davis, 2024).
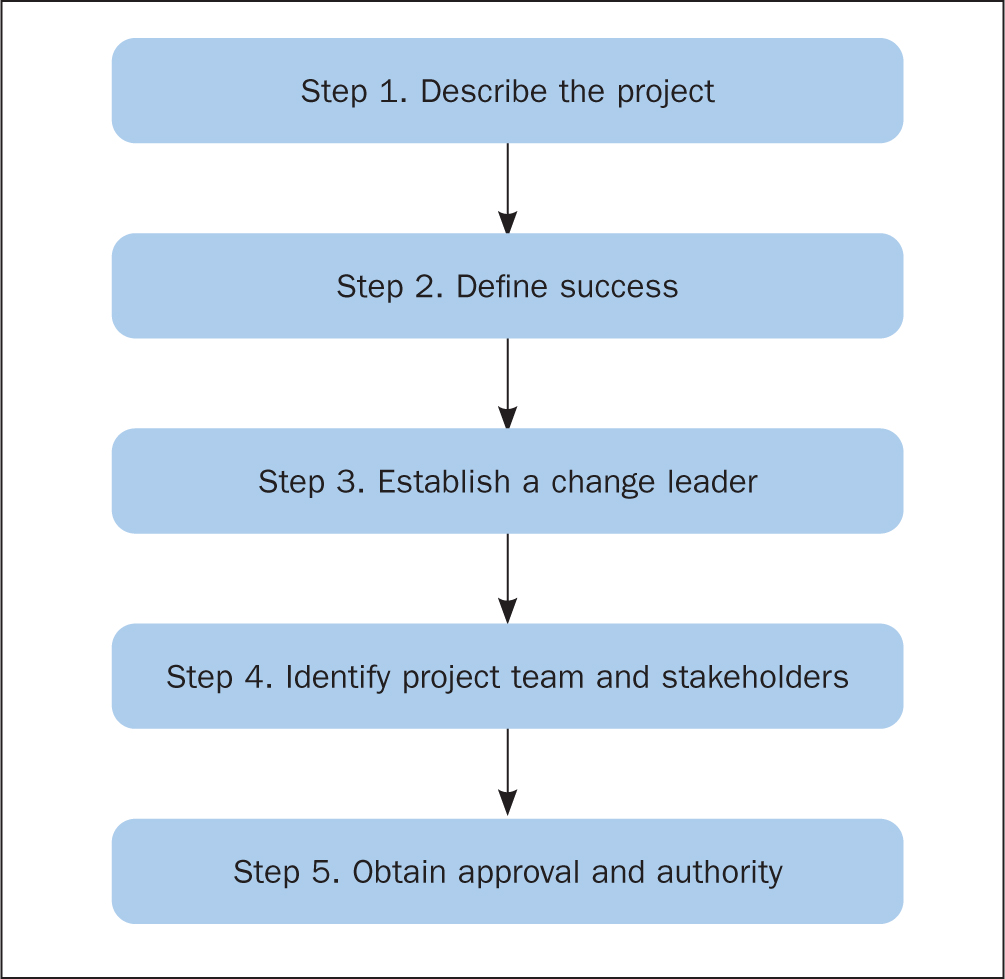
A project charter provides the structure necessary to support the proposed change process, identify the change team and stakeholders. A key factor to consider in determining the stakeholders and the core project team is where the initiative will take place, that is, will it be system-wide or focused on a few clinical units initially. Depending on the size of the healthcare organisation, focusing on a few select clinical units before scaling up across a larger system may be a good approach. Stakeholders should include clinicians but also supply management, medical providers, pharmacists, and patients (CDC, 2006; Kotter et al, 2021). If your organisation has an EBP council, these nurses can be a major asset in supporting your project and even participating in the core project team. Once a list of all stakeholders has been created, it will be easier to identify which ones should be a part of the core project team and what type of communication is required to each stakeholder group throughout the project. Nursing leadership, namely the chief nursing officer (CNO) in the US or chief nurse in UK hospitals, is likely the ultimate decision maker for this project. Nurse managers are often uniquely positioned to become change leaders – they can support staff in compliance with the adopted change, and some nurse managers will have budgets that may be used to purchase technology devices. Investigation into how capital equipment is purchased is essential to project charter development. Supply management can provide information on the cost of materials (such as PIV materials) and can supply an annual volume to support the project financially. The project charter must have structure while also allowing flexibility to make necessary alterations during the implementation stage. Therefore, it should be finalised and agreed with the core project team, to reduce fear and support ownership of the change process, thereby ensuring commitment to the goals and mission.
Step three: recognise and resolve resistance
The third step involves monitoring for resistance and leveraging the project team to recognise and resolve the stressor response and manage change resistance. Some team members can help to address institutional-based resistance while others will be instrumental in addressing personnel change resistance. Nursing administration/leadership support will have a significant influence on institutional change resistance. Nurse managers are instrumental in gaining personnel change support and it is critical that they understand Neuman's nursing theory related to change resistance. Nurse managers are the primary support for staff nurse compliance with the adopted change. This is a key factor. EBP standards do not implement change, people do. Therefore, understanding the foundations of personal resistance and seeking to resolve concerns through open and transparent communication is essential in EBP adoption. Change leaders should address the positive force pushing for change and the opposing force resisting change (Schriner et al, 2010). Nurses are regulated by administrative and facility policy, which can increase resistance to change. Remaining focused on meeting EBP standards, leading to better patient safety and outcomes, can help rationalise the proposed change and balance resistance. A focus on patient outcomes and also on employee satisfaction underlines desirable innovation components and will support successful integration (Kotter et al, 2021).
Effective leadership includes communication, influence, and interaction between individual team members on a day-to-day basis to maintain momentum while balancing multiple meetings with other change team members. The organisation and preparation of meetings is essential to avoid progress delays and build credibility. Each successful meeting builds on the urgency and excitement to help keep the process moving forward. Celebrating short-term wins with recognition of improvement is required to move forward in an environment with continually changing priorities (Kotter et al, 2021). Using communication strategies such as educational materials, reminders, computerised decision support, performance feedback, and organisational social media are avenues that help sustain the project momentum and progress. The complexity of the hospital system means there are many initiatives, all of which have a level of urgency. Therefore, the effective leader always pushes to keep the agenda moving forward (Porter-O'Grady and Malloch, 2018).
Step four: adopt technology and refreeze new EBP
In the final step, the goal is to refreeze the new EBP and technology adoption. This may include collecting further data to compare with baseline data and evaluate the impact. The evaluation and expansion phase is a time to also celebrate achievements and success. However, it is also crucial to disseminate and publish the findings of the change initiative. A first step in this regard is to disseminate within the healthcare organisation first and then seek other avenues for sharing the message and success (such as a journal publication or conference presentation). The internal organisational dissemination is most important to ensure adoption of the technology and EBP. Communication is vital here to ensure that the right findings are presented to the right stakeholders at the right time and in the right context. This can then support the need for expansion of the initiative to other units or departments within the healthcare organisation. Making sure the change aligns with the organisation's vision will help to sustain the EBP change and technology innovation.
Conclusion
Barriers to implementing EBP in healthcare are numerous, resulting in lower quality of care delivery, risks to patient safety, and increased costs (Mazurek Melnyk et al, 2021). Inadequate resources, lack of leadership support, and lack of clinician education related to implementation science create a barrier to EBP (Mathieson et al, 2019). The CTIM offers an effective instrument that is founded in change theory and implementation science and gives considerable attention to addressing change resistance. Simple removal of resistant individuals is not a realistic approach to dealing with change resistance. The CTIM offers a realistic approach to addressing resistance to EBP changes and technology adoption. For PIVC placement, it is critical to use technologies, such as the AccuVein AV500, to enhance compliance with EBP and support better outcomes for patients. Vessel preservation is the goal for the 2024 INS standards of practice (Nickel et al, 2024) and adoption of AccuVein AV500 vein visualisation technology to enhance PIV assessment offers an innovative and practical intervention to achieve this goal.
Implications for nursing management
Nurse managers are uniquely positioned to lead the way in embracing technology to improve care and reduce the EBP gap. In this article, a CTIM is presented, and real-life application examples are provided, based on an EBP initiative to adopt AccuVein AV500 technology in a large US hospital system. This information and EBP tool can help nurse managers to understand how to successfully implement a change initiative in their own unit or department, and apply the learning to improve PIVC placement in their own setting.
KEY POINTS
- The Clinical Technology Implementation Model (CTIM©) offers a practical, realistic, and evidence-based approach to address resistance to change and accelerate adoption of beneficial technologies
- The CTIM advocates that change leaders expect and embrace resistance to change rather than view it as something negative ie, change leaders should seek to understand the foundation of resistance and resolve concerns through open and transparent communication
- The CTIM has been used to successfully implement AccuVein near-infrared technology in a large hospital system in the US to improve peripheral intravenous (PIV) catheter access
- Vascular access specialists/clinicians are uniquely positioned to lead the way in embracing technology to improve PIV access and reduce the evidence-practice gap
CPD reflective questions
- Does your organisation experience any difficulty with implementing evidence-based practice?
- Is your organisation open to receiving change proposals from staff? Is there a process in place to review such proposals?
- How does your organisation support staff-initiated evidence-based practice changes?
- How does your organisation keep aware of new technologies and innovations that could improve practice?