
Epilepsy is a condition that affects the brain and is defined as a tendency to have unprovoked seizures (Kwan and Brody, 2010; Epilepsy Action, 2019). It is possible for an individual to have an isolated seizure without having epilepsy. A diagnosis of the condition will usually be made only if someone has had more than one seizure and the medical team considers that the person will have more (National Institute for Health and Care Excellence (NICE), 2018). Epilepsy can start at any age and varies from a condition that lasts a set period to one that can be lifelong (Kwan and Brody, 2010).
It is one of the most common neurological conditions (Meeraus et al, 2013) (Box 1), commonly diagnosed in childhood (Kwan and Brody, 2010), which affects around 50 million people worldwide. In some cases, the cause for the condition will remain unknown; however, there are some known reasons: stroke, head injury, infection such as encephalitis, or problems during birth (Shorvon, 2011; NICE, 2018). There remains discussion regarding the possibility of epilepsy being hereditary (Shorvon, 2011).
Some common seizures experienced by children are not classed as epilepsy, despite the feature of recurrence. For example, febrile seizures are those that are triggered by a high temperature (Patel et al, 2015). They happen to around 5 out of 100 children under the age of 6 years (Epilepsy Action, 2019) and are usually linked to a childhood illness. Febrile seizures are not epilepsy because they are provoked by the body's need to manage a temperature (Patel et al, 2015). However, it is considered that children who have had febrile seizures have a higher chance of developing epilepsy when they are older (NICE, 2013).
Seizures
A seizure is a sudden burst of unnecessary electrical activity in the brain (International League Against Epilepsy (ILAE), 2017), which disrupts the way the brain usually functions (D'Ambrosio and Miller, 2010). There are different types and presentation of seizure.
The classification of seizures, their signs and symptoms, will vary depending on where in the brain they begin and how they then progress (ILAE, 2017). Generally, seizures can be placed into two main categories: focal (partial) and generalised (ILAE, 2017). In focal seizures the electrical activity is focused in one area of the brain. Its presentation will depend on its location in the brain and that area's role. Understanding the structure and function of the brain will enable a nurse to better assess a child or young person presenting with a seizure (Figure 1). For example, the most common type of epilepsy to cause focal seizures is temporal lobe epilepsy (Epilepsy Action, 2019). The temporal lobe is responsible for many things, including language, feelings and memory. Symptoms may therefore include: sudden and unusual emotions or thoughts, being in a confused state, or unusual speech (Abhang et al, 2016).
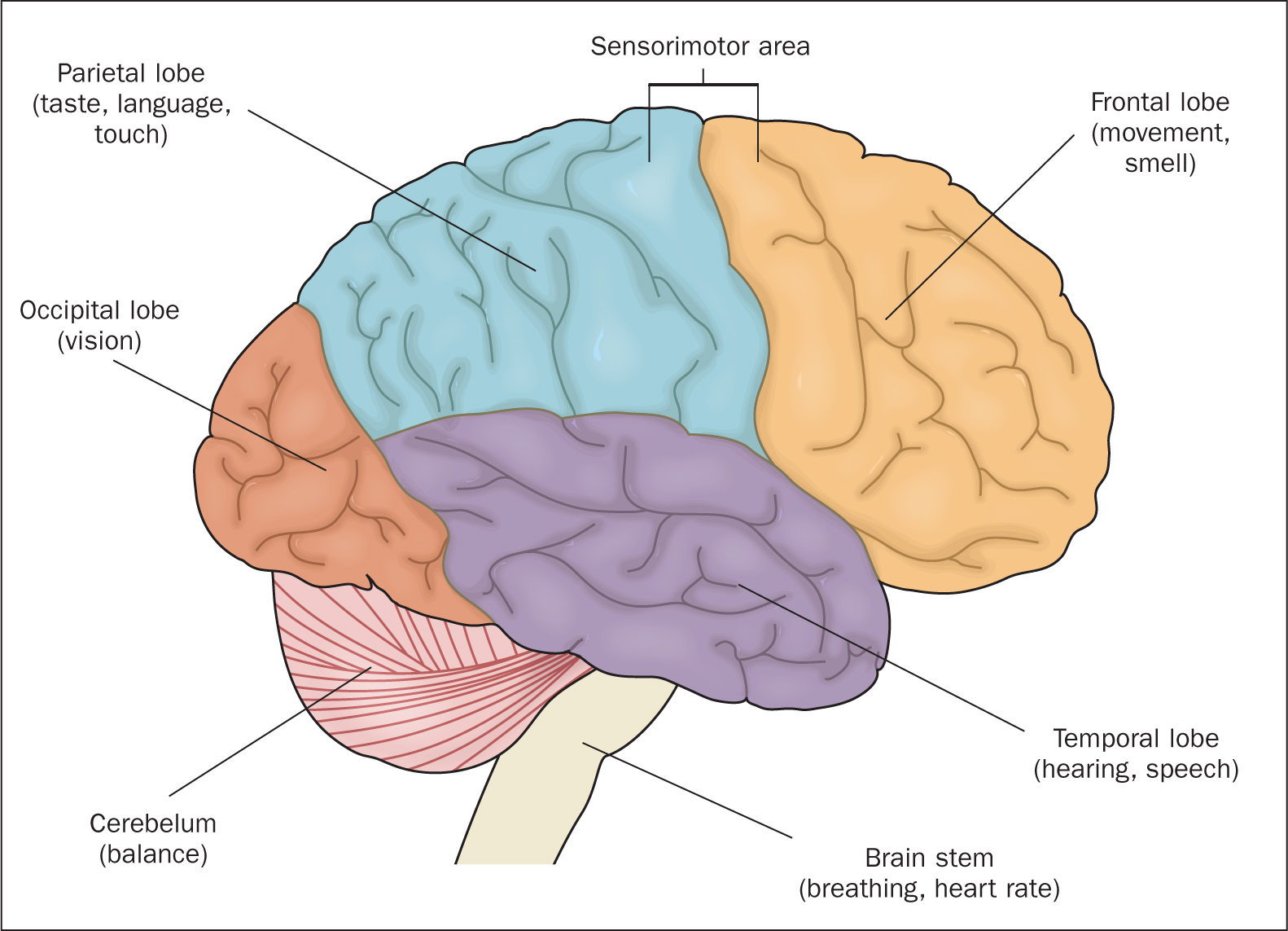
Generalised seizures are when the whole brain is affected by the sudden burst of electrical activity and the person becomes unconscious (NICE, 2018). The loss of consciousness can be very brief or lengthy. It may be that the child or young person gets symptoms suggesting that a seizure might be about to occur (Schulze-Bonhage et al, 2006). For example, if the electrical activity starts in the occipital lobe responsible for vision they may get visual disturbances before the electrical activity spreads to the rest of the brain, causing them to become unconscious.
In 2017, a new approach to classifying seizures was launched by the ILAE (2017). Naming a seizure type will be influenced by where in the brain it starts, the level of awareness during the seizure and whether the seizure involves movement or not.
As an example, a generalised tonic-clonic seizure affects both sides of the brain from the start. With this type of seizure awareness is fully impaired because the individual loses consciousness in the tonic phase. During this phrase they might also go stiff and drop to the floor, possibly biting down on their tongue; the limbs will often jerk rhythmically, the person may lose control of bodily functions, and breathing may be affected. This form is the most commonly recognised type, and was previously described as grand mal seizures (Epilepsy Action, 2019).
Diagnosis
A detailed and clear history, including description of the seizure presentation and length, is necessary to facilitate a diagnosis (NICE, 2018). This may be supported by a range of investigations to clarify the type or cause of the epilepsy (Shorvon et al, 2019). Investigations may involve blood tests, a brain scan or an electroencephalogram (EEG), which records the electrical waves in the brain.
However there is not a specific test to identify a diagnosis of epilepsy (NICE, 2018). This can make the process challenging for the family and the child while differential diagnoses are discussed (Shore et al, 2009; Lambert et al, 2014). A differential diagnosis may include: simple fainting, night terrors, breath-holding attacks, and pseudoseizures (Uldall et al, 2006).
Nursing care
If a child or a young person presents with a seizure it is vital for the nurse to follow a number of steps to maintain safety (Clore, 2010; NICE, 2013; Epilepsy Action, 2019). Box 2 describes how health professionals should manage a young patient having a focal seizure. In the case of a generalised seizure, the nurse should:
Children and young people with a diagnosis of epilepsy may be prescribed buccal midazolam if a seizure lasts longer than 5 minutes. Midazolam belongs to a group of medicines called benzodiazepines (Great Ormond Street Hospital for Children (GOSH), 2017). These work in the central nervous system by acting on specific receptors in the brain, making the nerves less sensitive to stimulation (GOSH, 2017). Side-effects may include tiredness, amnesia, sedation and breathing difficulties. This medication is administered to attempt to prevent status epilepticus: this is a medical emergency defined as 5 or more minutes of either continuous seizure activity or repetitive seizures with no period of recovery (NICE, 2013).
Communication and support
Family-centred care is a core concept in the nursing of children and young people, and remains vital when considering a child or young person diagnosed with epilepsy (Shields et al, 2012). Caregivers of children with epilepsy are at increased risk of post-traumatic stress disorder (Carmassi et al, 2017), so it is important for nurses to plan, implement and evaluate care with the whole family in mind, which may be supported by a specialist nurse (Royal College of Nursing, 2015). Epilepsy can place additional pressure on a child and their family, leading to decreased quality of life (Bilgiç et al, 2017). For example, young people with epilepsy are more likely to suffer social avoidance, depression and low self-esteem (Baker et al, 2005). It is thought that this may be in part due their understanding of their condition, which leads to a perception of lacking control (Jacoby and Austin, 2007). Education and support of the child or young person and their family are therefore vital.
Nurses should remain calm and reassuring throughout the episode of care, ensuring that they communicate clearly and consistently (Bilgiç et al, 2017). This should incorporate the opportunity to explore, discuss and support understanding, where appropriate. Part of this might include supporting the family in identifying any possible triggers that make the child or young person more likely to have a seizure (Jacoby and Austin, 2007). Examples of these include: not taking epilepsy medicine as prescribed, feeling tired, stress, being exposed to flashing lights or missing meals (Royal College of Paediatrics and Child Health (RCPCH), 2015). This information may inform documentation within the epilepsy passport, which is carried by the child at all times. It contains up-to-date information about the child's epilepsy and is accessible by health professionals in case of an emergency. It supports carers in all settings to understand the management of a child or young person's condition (RCPCH, 2015).
Treatment and management
The main treatment for epilepsy is medication. These drugs are sometimes called anti-epileptic drugs or AEDs (NICE, 2013). The medication does not cure epilepsy, but it helps to stop or reduce the number of seizures. If epilepsy medicine does not work well for someone, their specialist team might suggest other types of treatment. Other types of treatment include brain surgery, vagus nerve stimulation, or a special nutritional plan called the ketogenic diet, which is sometimes recommended for children (Epilepsy Action, 2019).
Conclusion
To safely care for a child or young person with epilepsy a nurse must have a good understanding of the condition and its varying presentations. By reviewing the classification of seizures, nurses will be able to interpret and explain to families' complex medical terms. This article has provided a brief introduction to recognising epileptic seizures in children and young people and the initial management of young patients. Nurses should explore the topic further through reading and apply their new knowledge in their practice area.