
Diabetes mellitus is a condition that results in elevated blood glucose levels (hyperglycaemia). Continued elevation can contribute to progressive micro- and macrovascular complications leading to renal, nerve and ocular damage, representing a significant contributor to morbidity and mortality (Bilous and Donnelly, 2010). Currently there are more than 3 million adults (aged 18–99) diagnosed with the condition in the UK, representing a population prevalence of 5.9%; 1 in 17 adults has diabetes mellitus (International Diabetes Federation (IDF), 2017).
Type 1 diabetes mellitus represents approximately 10% of cases. The origin of the condition is autoimmune in nature, arising from the complete destruction of insulin-secreting beta cells within the pancreas. Type 1 diabetes results in an absolute absence of insulin and therefore blood glucose levels continue to rise because glucose cannot enter the body's cells to be metabolised and produce energy; excess glucose cannot be stored as glycogen. These individuals require insulin injections every day.
Type 2 diabetes mellitus accounts for the remaining 90% of cases. It causes cells to be less responsive to insulin and/or reduces insulin production by the pancreas; therefore, glucose entry into the cell is reduced resulting in increased blood glucose levels. Type 2 diabetes is caused by a combination of genetic and ethnic predispositions, but predominantly lifestyle factors such as obesity and lack of physical exercise. Incidence is further correlated with increasing age (Holt and Kumar, 2015). Individuals may take medications to increase insulin production, to make cells more receptive to insulin or, ultimately, may require injectable insulin.
Gestational diabetes mellitus manifests with a degree of glucose intolerance with onset or first recognition in pregnancy. Individuals affected have an increased risk of developing diabetes after pregnancy (Buchanan et al, 2007).
There are several subtypes of diabetes outside these three, including but not limited to genetic defects leading to diabetes, idiopathic diabetes (presenting with no underlying autoimmune cause), endocrinopathies, or drug- and chemical-induced diabetes. For these reasons, and the potentially mixed picture of diagnosis, it is less important to label the type of diabetes than it is to understand the mechanisms and importance of hyper- and hypoglycaemia and treat accordingly (American Diabetes Association, 2013).
Rationale for blood glucose monitoring
The measurement of blood glucose provides information on the effectiveness of blood glucose metabolism and guides interventions to achieve optimal glucose control within the body.
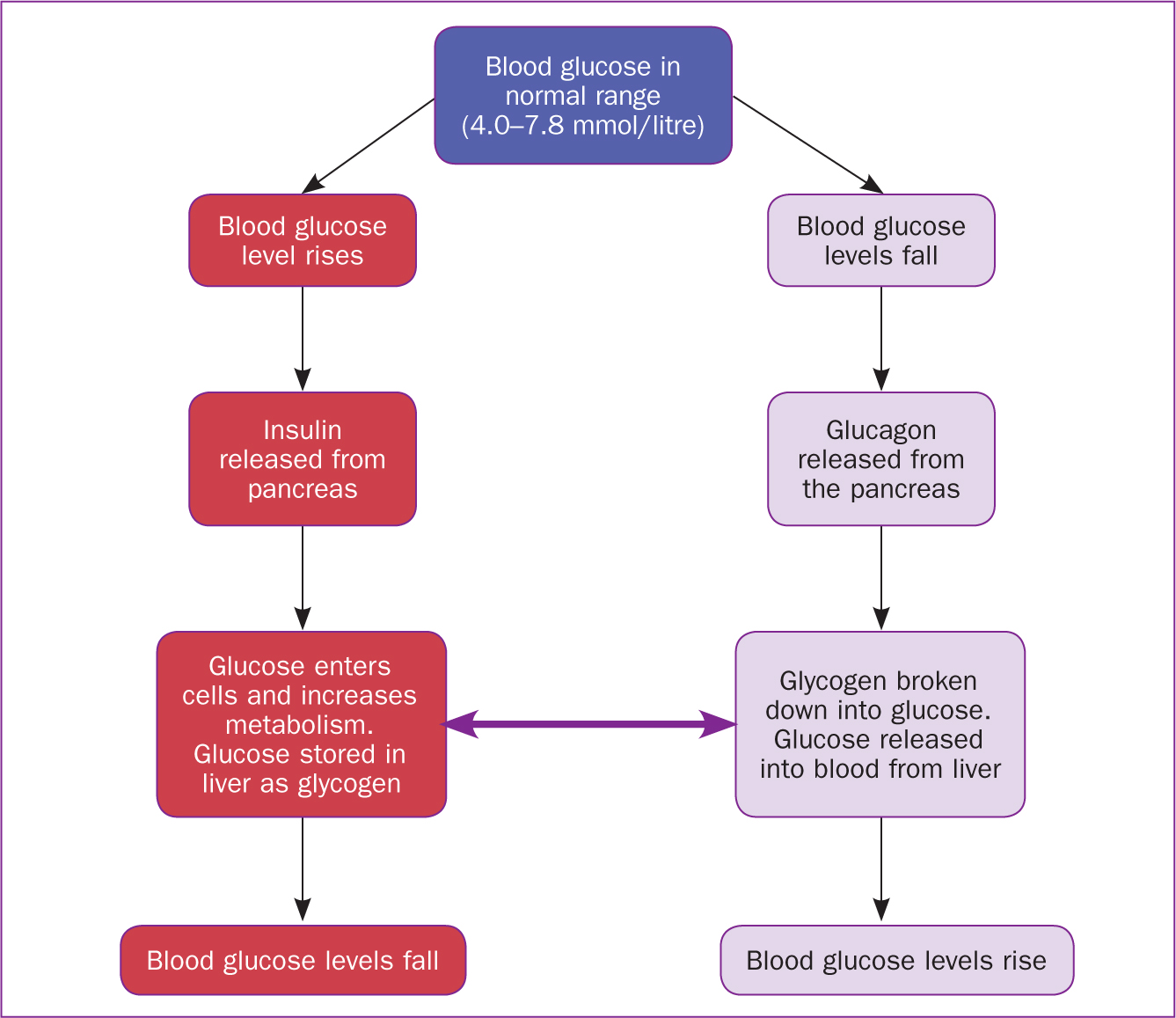
Glucose is a monosaccharide and is an essential fuel for the brain and other body cells formed as an end product of carbohydrate digestion (Maughan, 2009). Glucose is either metabolised to produce energy or is stored in the muscles and liver as glycogen. Changes in the glucose level after absorption of carbohydrate is termed the ‘glycaemic response’ (Maughan, 2009; Sanders, 2016). Regulation of normal glucose metabolism is shown in Figure 1.
The measurement of blood glucose is a key self-care activity for people with diabetes and has been shown to positively correlate with improved long-term glycaemic control (Shaji et al, 2013; Shrivastava et al, 2013) and can function as a cue to action in diabetes self-management (Brackney, 2018).
The measurement of blood glucose is also a key nursing assessment in (Delves-Yates, 2018a):
Nurses should observe patients whose blood glucose levels fall below 4 mmol/litre closely.
Point-of-care testing for blood glucose levels is managed with the use of bedside finger-prick testing. Using this approach, capillary blood glucose monitoring provides immediate results of hypo- and hyperglycaemia (Dougherty and Lister, 2015). In the past, urine test strips were used; however, accurate measurements relied on stable renal function, making the test potentially unreliable (Holt, 2014).
Blood glucose ranges
Normal target ranges
The National Institute for Health and Care Excellence (NICE), 2016a) states that normal target ranges should be as follows:
Hyperglycaemia
Hyperglycaemia occurs when there is a random plasma glucose of more than 11 mmol/litre (NICE, 2016b).
Hyperglycaemia describes any blood glucose concentration that is higher than the recognised target ranges (Patton and Thibodeau, 2015). Prolonged hyperglycaemia can result in damage to many organs of the body, leading to renal failure, blindness or gangrene resulting in amputation (Boore et al, 2018).
Acute hyperglycaemia occurs when the body cannot utilise glucose because of insufficient or a complete lack of insulin production. This causes the body to generate glucose via glycogenolysis (glycogen breakdown), lipolysis (fat breakdown) and gluconeogenesis (glucose derived from substrates such as lactate, glycerol and glucogenic amino acids). Blood glucose rises further, and the person is effectively ‘starving in a sea of plenty’ (Dean et al, 2004). Fatty acid metabolites known as ketone bodies, accumulate from this process, resulting in diabetic ketoacidosis (DKA). Ketones are observed in the blood and urine (Marieb and Hoehn, 2015; Patton and Thibodeau 2015). Symptoms of hyperglycaemia are summarised in Table 1. Points to note about DKA are listed in Box 1. Hyperglycaemia can also lead to hyperosmolar hyperglycaemic syndrome (see Box 2).
| Gastrointestinal |
|
| Adrenergic |
|
| Respiratory |
|
| Renal |
|
| Electrolyte imbalance |
|
| Liver and adipose tissue |
|
| Cardiovascular |
|
| Central nervous system |
|
Causes
The causes of hyperglycaemia are (Marieb and Hoehn, 2015):
Hypoglycaemia
Hypoglycaemia is defined as a random plasma glucose of less than 4 mmol/litre. It occurs when blood glucose levels fall resulting in inadequate energy available to the brain, leading to abnormal behaviour—sometimes mistaken for drunkenness (Patton and Thibodeau, 2015). If prolonged, the individual may lose consciousness and, if not treated, may die (Boore et al, 2018).
The symptoms of hypoglycaemia are outlined in Table 2.
| Central nervous system |
|
| Cardiovascular |
|
| Gastrointestinal |
|
| Adrenergic |
|
Causes
Hypoglycaemia treatment
NICE and the British National Formulary (Joint Formulary Committee, 2019) recommend the following. In mild to moderate hypoglycaemia:
In severe hypoglycaemia (causing unconsciousness):
It is important to note that people with type 1 diabetes may become increasingly unaware that they are experiencing a hypoglycaemic episode as the number of episodes they experience increases. This is termed ‘hypo unawareness’. People with type 1 diabetes should be assessed for their awareness of hypoglycaemia at each annual review with their doctor (NICE, 2016a).
Careful consideration must be given to the management of people with diabetes undergoing surgery, as outlined in Table 3.
| Target group | Plan |
|---|---|
| Well-controlled type 2 diabetes |
|
| People on insulin, with type 1 diabetes or undergoing major elective surgery |
|
Blood glucose measurement
There are many devices available for point-of-care testing. Several factors should be considered in the selection of meters, testing strips and lancets, including:
Staff must be appropriately trained in the use of blood glucose meters, have an awareness of potential sources of error, be able to give advice and interpret results and have their competence recorded appropriately with access to regular updates. There must be a standard operating procedure/local policy in place to ensure testing is carried out in line with best available evidence and with access to the manufacturer's guidance on the use of all blood glucose monitoring equipment (Medicines and Healthcare products Regulatory Agency (MHRA), 2013).
Equipment
The following should be assembled (Delves-Yates, 2018b):
Table 4 outlines the blood glucose monitoring procedure.
| Step | Procedure | Rationale |
|---|---|---|
| 1 | Decontaminate the machine as per local policy and switch on. Ensure correct date and time are displayed and that there is adequate battery. Scan operator ID if required according to local policy |
|
| 2 | Ensure the unit of measurement is mmol/litre |
|
| 3 | Ensure equipment is correctly set up, this may vary according to the device or if automated systems are used. Always follow manufacturer guidelines and local policy. Checks may include: |
|
| 4 | Identify the individual verbally and check against the wrist band |
|
| 5 | Select an appropriate site, consider: |
|
| 6 | Ask person to sit/lie down |
|
| 7 | Ask the person to wash hands with soap and water and dry with low-linting gauze |
|
| 8 | Practitioner to wash hands and don gloves and observe universal precautions according to local policy |
|
| 9 | Take a single-use lancet and ensure correct setting is used if depth setting can be adjusted |
|
| 10 | Remove the device cap if present; activate the lancet according to the manufacturer's guidance at the selected site. Use the side of the finger. Rotate sites |
|
| 11 | Dispose of the lancet according to local policy |
|
| 12 | Insert the test strip into the blood glucose meter. Ensure meter is ready for droplet. Apply and ensure the window is entirely covered with blood |
|
| 13 | Apply gauze and pressure to puncture site, monitor for excessive bleeding |
|
| 14 | Remove gloves and apron, dispose of as per local policy, carry out hand hygiene according to local policy |
|
| 15 | Document result and sign according to local policy |
|
| 16 | Decontaminate the meter |
|
| 17 | Report any results outside of normal ranges |
|
| 18 | Ensure the person is comfortable and receiving appropriate care |
|
Errors in results
Potential sources of error include (Hortensius et al, 2011; Dougherty and Lister, 2015; Training Research and Education for Nurses in Diabetes UK, 2017):
Conditions that may interfere with point-of-care testing and contraindications to point-of-care testing are given in Table 5.
| Contraindication | Example |
|---|---|
| Dialysis treatment | Some fluids may contain maltose, a disaccharide, which can interfere with test strip methodology |
| Peripheral circulatory failure | Severe dehydration, diabetic ketoacidosis, hypotension, shock, peripheral vascular disease |
| Severe dehydration | Vomiting or diarrhoea, diuretics, uncontrolled diabetes |
| Variations in blood oxygen tension | People receiving intensive oxygen therapy |
| High concentrations of non-glucose-reducing substances in the blood | Intravenous infusion of ascorbic acid |
| High bilirubin values | Jaundice |
| Extremes of haematocrit | Neonatal blood samples, pregnancy |
| Hyperlipdaemia | Total parenteral nutrition, hyperlipidaemia |
Note: All glucose meters/strips' instructions give a number of situations/conditions where the test result may be affected and when the meter/strips should not be used. A laboratory measurement of glucose using a venous sample should be performed where contraindications are observed or suspected and when abnormal or unexpected results are obtained. The operator must be aware of the contraindications particular to the type/brand of equipment they are using
Monitoring and reporting
Accurate recording of blood glucose monitoring is essential to ensure safety. Records should include results, test strip lot number, meter maintenance records, calibration and quality control testing, patient and operator identity and battery change (MHRA, 2013). Technology is now available to utilise wireless devices for point-of-care testing that allows electronic data capture and documentation of results, device testing and operator identification, directly linked to the patient's medical records (Roche, 2018).
Self-monitoring
In the community, routine self-monitoring of blood glucose levels is advised for all people with type 1 diabetes, ideally at least 4 times a day: before each meal and before bed (NICE, 2016a). People with type 2 diabetes should also self-monitor blood glucose if they require insulin, have evidence of hypoglycaemia, or if pregnant or planning pregnancy (NICE, 2017a).
Technologies are available that enable people with diabetes to continuously monitor and manage their blood glucose and review results via mobile devices. In November 2017, the Abbott FreeStyle Libre flash glucose monitor device was made available through the NHS formulary for people with type 1 diabetes who meet specific criteria. The device continuously measures glucose levels within interstitial fluid, using a sensor applied to the skin (NICE, 2017b). Such devices will become increasingly prevalent in the future.
Consideration should be given when people who routinely monitor their own blood glucose are admitted to hospital. There is conflicting evidence about the continuation of self-monitoring in the inpatient setting. Some authors highlight the complexity of hospital treatment and its effect on normal glucose control as a factor that makes self-monitoring beyond the ability of the individual to manage their own blood glucose (Shah and Rushakoff, 2015); others counter this argument highlighting that removing self-monitoring may place the person at increased risk of hypo- or hyperglycaemia (Mabrey and Setji, 2015). However, there is consensus that co-operative management and partnership with people with diabetes should be encouraged to maximise satisfaction and clinical outcome.
Recommendations
Timely internal quality control, including unit calibration, must be carried out according to local policy and the manufacturer's guidance to ensure the device is working correctly and results are reliable. External quality assessment should also be implemented using the analysis of standardised test samples with an undisclosed value from an external source. Participation in an external quality assessment scheme allows comparability across sites and can often be co-ordinated through laboratory departments (MHRA, 2013). Holt and Kumar (2015) suggested the use of technologies that use existing wireless point-of-care testing to integrate with a diabetes data management system to proactively institute timely changes in diabetic management. Electronic prescribing further enhances this safety focus.
Conclusion
All nurses should be familiar with the importance of blood glucose monitoring and the procedure to carry out testing safely and effectively. Appropriate and timely monitoring of blood glucose will allow for the successful management of blood glucose levels that fall outside target ranges. This will ensure ongoing safety during episodes of acute illness or effective management of diabetes in the longer term, minimising future diabetes-related health complications.