

The role of advanced clinical practitioners (ACPs) has emerged in the NHS as a response to increasing healthcare demands, workforce shortages, and the need for more flexible, skilled practitioners who can deliver high-quality care across various settings (Evans et al, 2020; Timmons et al, 2023). ACPs are essential in managing a wide range of health conditions, including dermatological presentations, where they play a crucial role in skin assessment, examination, management, and referrals to dermatology teams (Alsararatee, 2024). Despite their pivotal role, many ACPs report a lack of confidence in conducting comprehensive dermatological assessments. To address this gap, this article aims to guide novice ACPs in performing systematic dermatological assessments and examinations. It covers essential aspects such as accurately documenting the presenting complaint and the history of the presenting complaint, understanding the past medical and surgical history, and gathering detailed information on medications and allergies, and on family history to identify potential hereditary conditions.
An essential component of dermatological assessment is understanding the psychosocial impact of skin conditions on patients. Skin diseases can significantly affect mental health, contributing to anxiety, depression and reduced quality of life (Cortés et al, 2022). A thorough evaluation of how skin conditions affect quality of life should be conducted, including assessments of social functioning, sleep disturbances, and the psychological toll. Recognising these elements is crucial for a holistic approach to dermatological care. In addition, it is vital to distinguish between rashes (eruptions) and lesions, as they may present differently and require tailored approaches to diagnosis and management.
Rashes and lesions differ in both presentation and underlying causes (Badia et al, 2020). Rashes, or eruptions, typically refer to widespread areas of inflammation or irritation on the skin, affecting large regions and often indicating a systemic or diffuse process (Feig and Cohen, 2022). They can appear as maculopapular, vesicular or erythematous, and are commonly associated with infections, allergic reactions or inflammatory skin conditions such as eczema. On the other hand, lesions are more localised abnormalities on the skin that can be solitary or grouped, presenting as macules, papules, nodules or plaques (Johal et al, 2021). Lesions often indicate a specific pathological process, such as a tumour, localised infection or trauma. Understanding this distinction helps clinicians tailor diagnostic approaches, as rashes often suggest broader systemic involvement, whereas lesions point to localised issues requiring focused examination.
This article emphasises the importance of taking a social history, including factors such as sleeping patterns, smoking, alcohol consumption, menstrual history, recreational drug use, diet, sun exposure and occupation, because these elements can significantly impact dermatological health. Furthermore, it highlights the need to consider contact and travel history to identify potential environmental or infectious contributors to skin conditions. In addition, this article also provides detailed guidance on physical examinations, including assessing the morphology, colour, distribution and palpation of skin lesions. It highlights the importance of examining the scalp and hair, nails and mucous membranes, ensuring a thorough and holistic approach to dermatological care. By integrating these elements, ACPs can enhance their confidence and proficiency in dermatological assessments.
History of the presenting complaint
Allowing the patient to tell their story without interruption is crucial (Cappella and Street, 2024). This approach helps them share their concerns and feel heard. Begin the consultation with open questions, then transition to semi-open and focused questions as needed (Mohd Salim et al, 2023). Furthermore, provide the patient with enough time to answer and avoid interrupting them (Milton et al, 2023). When gathering the history of a skin condition, it is important to systematically assess both rashes and lesions to gain a comprehensive understanding of the patient's concerns (Yon et al, 2023). Clinicians should begin by allowing the patient to describe the onset, duration and progression of the skin issue. Asking whether the condition is acute or chronic and whether there have been previous episodes helps in establishing patterns and possible triggers (Snyder et al, 2023).
For eruptions, specific attention should be given to the distribution, whether localised or generalised, and whether there is symmetry or asymmetry in its presentation. Associated factors such as itching, pain, or other symptoms should also be explored. For lesions, it is crucial to assess their size, shape, and colour, following structured guidelines such as the ABCDEFGH criteria to rule out malignancy (Brown et al, 2023). In addition, the Primary Care Dermatology Society (PCDS) website offers practical tools and structured guidance to enhance the assessment of skin conditions, including lesion morphology and common dermatological patterns (PCDS, 2024). This resource can help clinicians apply a systematic approach to both rashes and lesions, aiding diagnosis and management.
Location of the symptom
Asking about the site of the rash is important because it can provide clues about the cause and type of rash (Albright and Morrison-Beedy, 2024). Different conditions affect specific areas of the body. For example, contact dermatitis might appear where the skin touches an allergen, whereas fungal infections often occur in warm, moist areas (Oliveira et al, 2023). Knowing the location helps make an accurate diagnosis and determine the best treatment.
Onset
Clarifying how and when the symptom developed is important because it helps in diagnosing the condition accurately (Ayo et al, 2020). The onset can indicate whether the rash is acute or chronic, and can help identify possible triggers or causes (Macy, 2021). For example, a sudden onset might suggest an allergic reaction that can be stopped by discounting the causative medications, whereas a gradual development might indicate a chronic condition. A rapidly growing non-pigmented nodule raises suspicions of squamous cell carcinoma or amelanotic melanoma (Smith and Wernham, 2020).
Character
The character of a skin condition is crucial for ACPs to evaluate, as it guides diagnosis and treatment. Primary symptoms such as dryness, itching and pain reflect the patient's experience and provide essential diagnostic insights. It is important to observe whether lesions are monomorphic (uniform, as seen in drug reactions) or polymorphic (variable, as in chickenpox) (Oakley, 2022). This distinction helps ACPs understand the condition's underlying cause and adapt treatment strategies accordingly. Recognising these characteristics enables more accurate, patient-focused therapeutic approaches, ultimately improving clinical outcomes.
Radiation
Asking the patient if the symptom moves or spreads to other areas can provide insight into the nature and severity of the condition (Roche et al, 2021). For instance, a rash that spreads might indicate a systemic issue or a more widespread infection. This is especially important because some acute conditions require urgent treatment, such as necrotising fasciitis, toxic epidermal necrolysis and erythroderma. These serious conditions need immediate medical attention to prevent severe complications (Alsararatee, 2024). Patients sometimes present with one lesion, and the ACP should ask if similar lesions are distributed elsewhere. Some dermatological skin lesions are diagnosed based on their distribution – for instance, psoriasis is mostly distributed in the extensors and atopic dermatitis is distributed in the flexures. Therefore, distribution is important in the clinical diagnosis.
Associated symptoms
Associated symptoms refer to additional signs that accompany the primary skin condition but are not directly part of the lesion itself (Callen et al, 2016). These might include systemic symptoms such as fever, fatigue or malaise, suggesting broader implications of the underlying disease. For ACPs, identifying these symptoms is essential, because they provide important clues to systemic involvement and guide comprehensive patient care. For instance, when a skin condition is accompanied by fever or malaise, it may indicate an infectious or autoimmune component, prompting further investigation and adjustments to the treatment plan.
Exacerbating or relieving factors
Identifying factors that worsen the condition, such as specific allergens or environmental triggers in the case of a rash, can aid in avoidance strategies or targeted treatment (Faraz et al, 2024). Conversely, recognising factors that alleviate the rash, such as certain medications or skincare practices, can inform management plans and improve patient outcomes by optimising symptom relief. Additionally, recognising patterns such as relapsing hand dermatitis improving over weekends suggests occupational allergic or irritant contact dermatitis (Russo et al, 2023). Furthermore, melasma worsens with UV light exposure, making it more noticeable in summer, while psoriasis tends to improve in sunny weather (Passeron et al, 2020).
Severity
Assessing the severity of symptoms on a scale of 0 to 10 is crucial in skin assessment, particularly in identifying potentially life-threatening conditions such as necrotising fasciitis or severe drug reactions such as Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and drug reaction with eosinophilia and systemic symptoms (DRESS) (Alsararatee, 2024). For example, a patient presenting with a rapidly spreading rash accompanied by severe pain and a high severity rating on the scale may indicate necrotising fasciitis, a serious bacterial infection requiring immediate surgical intervention to prevent tissue necrosis and systemic complications (Alsararatee, 2024). Similarly, in cases of SJS, TEN, or DRESS, a high severity rating for skin involvement, along with systemic symptoms such as fever, malaise and organ involvement, signifies the need for urgent medical attention and discontinuation of culprit medications to prevent further progression and improve outcomes (Perwitasari et al, 2021). This grading system aids dermatologists in promptly recognising and managing potentially life-threatening skin conditions based on the perceived severity of symptoms, thereby optimising patient care and outcomes.
Previous episodes and treatments
When enquiring about previous episodes of the skin condition, it is important to ask whether the patient has experienced similar issues in the past and how these were managed (Singh et al, 2022). Clinicians should also assess the patient's understanding of previous treatment advice, including how much and when to use medications, as well as when to start or stop treatment. This ensures that the patient adheres to the prescribed treatment regimen and understands critical aspects of medication use, such as timing, dosage, and potential side-effects. Additionally, it is essential to evaluate whether the treatments were effective and if there were any adverse reactions or misunderstandings regarding the treatment plan. Clarifying these aspects can help prevent misuse or overuse of medications, leading to better management in future episodes.
Contact history
It is important to ask about recent contacts with infectious diseases or individuals with similar skin problems (Cortés et al, 2022). Asking the patient directly, ‘Have you been in contact with anyone recently who had an infectious disease or skin problems like yours?’, helps identify potential sources of infection or transmission, aiding in the diagnosis and management of the patient's condition. This information enables healthcare providers to take appropriate precautions, conduct further evaluations if necessary, and implement targeted treatment strategies to prevent the spread of contagious diseases and ensure optimal patient care.
Ideas, concerns and expectations
Incorporating the Ideas, Concerns, Expectations (ICE) framework into dermatological assessments enables ACPs to provide patient-centred care by exploring the patient's perspectives (Simon et al, 2020). ACPs can ask, ‘What do you think is causing this?’, to understand the patient's ideas and any underlying misbeliefs. Addressing concerns by asking, ‘Is there anything about this condition that worries you?’, encourages patients to share fears, allowing ACPs to provide reassurance. Additionally, exploring expectations with,‘What do you hope we can achieve?’, ensures treatment plans are aligned with patient goals, fostering collaborative care.
Understanding expectations through questions such as,‘What are you hoping we can achieve today?’, ensures that treatment aligns with the patient's goals, whether focused on symptom relief, cosmetic outcomes or reassurance. This approach allows for shared decision-making, where the patient's expectations are integrated into the management plan. For example, if a patient is particularly concerned about scarring, incorporating discussions around reducing scars in the treatment plan enhances patient satisfaction and helps the ACP create a more personalised and collaborative care approach.
Additionally, integrating the ICE framework into follow-up care strengthens continuity by allowing ACPs to reassess patient ideas and concerns as treatment progresses, ensuring any evolving expectations align with clinical outcomes. Embedding the ICE framework in the assessment and treatment process fosters a collaborative, patient-centred approach, which enhances care quality and patient engagement. This holistic strategy empowers patients, making them active participants in their care, and improves satisfaction and trust. By maintaining open communication at every stage, the treatment plan becomes more adaptive and responsive to patient needs.
Summary of the patient history
Summarising the history taken is crucial for clinicians to ensure all relevant information is captured accurately. This process allows clinicians to identify any gaps or errors in the information provided, thereby enhancing the accuracy of the diagnosis and treatment plan, while also giving patients an opportunity to correct any inaccuracies.
Systemic enquiry
A systemic enquiry in dermatology involves screening for symptoms in other body systems, which may not initially seem relevant to the primary presenting complaint. This approach helps identify potential systemic conditions that may manifest with skin symptoms or impact overall health. For example, fevers may indicate underlying cellulitis, while peripheral oedema could suggest cardiovascular issues (Tienpratarn et al, 2024). Moreover, screening for respiratory symptoms such as wheezing and dyspnoea might indicate anaphylaxis. By assessing various body systems, clinicians can detect relevant comorbidities or complications, ensuring comprehensive patient care and management.
Past medical and surgical history
Inquiring about the patient's medical history provides insights into existing skin lesions or rashes, and ongoing treatments and management. For instance, in a patient with diabetes, there can be cancerous nigricans or intertrigo and recurrent candidiasis (Yesudian, 2024); patients with hypothyroidism may develop dry or thickened skin or vitiligo.
By asking questions such as ‘Do you have any medical conditions?’, and ‘Are you currently seeing a doctor or specialist regularly?’, ACPs can gather information about the patient's overall health status and potential systemic factors that affect their skin condition. Considering inflammatory skin diseases' non-dermatological symptoms underscores the importance of systemic implications. For instance, arthralgia may accompany cutaneous lupus or psoriasis, or the ‘atopic march’ links atopic eczema with food allergies, asthma, and hay fever. Generalised pruritus with night sweats and weight loss may indicate underlying lymphoma; specific rashes such as the photosensitive malar rash in systemic lupus erythematosus provide diagnostic clues (McCormick et al, 2024). ACPs should enquire about previous surgeries for cancer, as cutaneous metastases may develop at surgical sites (Johnston et al, 2023).
Medication history
Inquiring about the patient's medication history helps to understand potential exacerbating factors for skin conditions (Albright and Morrison-Beedy, 2024). Asking, ‘Are you currently taking any prescribed medications or over-the-counter treatments?’, allows clinicians to document medication details, including name, dose, frequency, form and route. It is crucial to inquire about any side-effects from medications, because certain drugs can worsen skin diseases. For example, β-adrenoceptor blockers (beta blockers) can worsen psoriasis (Ray et al, 2023) and gliptin family medications (dipeptidylpeptidase 4 inhibitors) can worsen bullous pemphigoid (Hadjkacem et al, 2023).
Allergies
Enquiring about allergies is essential to identify potential triggers for skin reactions (Sheikh and Jha, 2024). Asking if the patient has any allergies and clarifying the type of reaction they had, such as a mild rash or anaphylaxis, helps assess the severity and manage the risk of allergic reactions. Documenting drug allergies, including skin contact allergies caused by lanolin or rubber, is important for treatment decisions (Fonacier et al, 2024). ACPs should exercise caution regarding reported penicillin allergies, as studies indicate that a significant proportion of these reports are inaccurate. For instance, a study by Shenoy et al (2019) found that fewer than 5% of patients with a reported penicillin allergy have clinically significant reactions upon evaluation. Addressing these inaccuracies through detailed patient histories and appropriate testing allows clinicians to tailor treatment plans effectively, ensuring safe and optimal management of dermatological conditions.
Family history
Asking the patient if there is any family history of skin disease helps to identify familial patterns of dermatological conditions. Clarifying at what age the disease developed is crucial, because diseases developed at a younger age are more likely to be associated with genetic factors. For example, asking,‘At what age did your father develop melanoma?’, helps assess the genetic risk factors for melanoma. Certain dermatoses, such as atopic eczema, psoriasis, and ichthyosis, often run in families.
Individuals with a close family history of melanoma are at an increased risk of developing the disease themselves. Approximately 10% of melanoma patients have a family member with a history of the condition (Skin Cancer Foundation, 2024). This elevated risk may be due to shared genetic factors, similar skin types, or common environmental exposures within families. Notably, having one or more first-degree relatives (parents, siblings, or children) diagnosed with melanoma significantly heightens an individual's risk (American Cancer Society, 2024). Therefore, it is crucial for individuals with a family history of melanoma to engage in regular skin examinations and adopt preventive measures to mitigate their risk.
Additionally, suspicion of cancer-associated genetic syndromes, such as Gorlin and Muir–Torre syndromes, can be raised by a strong family history of malignancy (Lam et al, 2024). By understanding the patient's family history of dermatological diseases, ACPs can better assess genetic predispositions and tailor management strategies accordingly.
Social history
It is important to record the following aspects in a social history.
Sleeping patterns
Sleeping patterns can determine whether the skin condition impacts quality of life. For instance, psoriasis can be exacerbated by stress, thus causing patients to have insomnia (Cameron et al, 2024).
Smoking
Document the patient's smoking history, detailing the type and quantity of tobacco consumed. Smoking is a known risk factor for skin cancer and has notable effects on overall skin health (Jackson et al, 2024).
Alcohol intake
Record the frequency, type and volume of alcohol intake per week, as alcohol consumption can exacerbate various skin conditions such as psoriasis and hidradenitis suppurativa. Patients who drink alcohol excessively might have liver cirrhosis and if clinicians are planning to start them on methotrexate it is crucial to check liver functions before starting steroids to avoid further damage to the liver.
Menstrual history
This is important when it comes to conditions such as polycystic ovary syndrome if the patient presents with hirsutism (Siusiuka et al, 2023).
Recreational drug use
It is important to inquire about recreational drug use, specifying the types and frequency of consumption. Intravenous drug use elevates the risk of cellulitis and necrotising fasciitis at injection sites, along with heightened susceptibility to HIV and hepatitis B and C, which often manifest with dermatological symptoms.
History of sun exposure and burns
The ACP should assess the patient's history of sun exposure and sunburn, particularly in childhood, which correlate with increased melanoma risk (Wunderlich et al, 2024). Chronic UV exposure, common in outdoor sports and certain occupations, heightens the risk of non-melanoma skin cancers, especially in fair-skinned individuals.
Diet
The social history should also include questions about recent dietary changes or foods that trigger symptoms, this includes rashes associated with conditions such as coeliac disease (Butterworth and Los, 2024).
Occupation
Clarify the patient's current occupation to understand potential exposures. Occupations involving frequent hand washing (‘wet work’) pose an increased risk of irritant hand dermatitis (Vilela et al, 2024). Explore whether skin issues worsen during work hours and improve during breaks and identify any exposure to skin irritants or hazardous substances, such as hair dye chemicals among hairdressers or epoxy resins in metalworkers.
Pets
Address any pet ownership, recognising pets as sources of fungal infections and fleas, leading to flea bite allergies. Fish enthusiasts face a risk of chronic mycobacterial skin infections if they fail to wear proper protective gear during tank maintenance (Spiliopoulou et al, 2023).
Travel history
Inquiring about recent travel history may provide valuable clues to the patient's presenting complaint. For example, asking the patient if they have recently been travelling can help identify potential exposures that may be relevant to their skin condition, such as erythema migrans after visiting a location with potential tick exposure (Bonnet et al, 2023). Moreover, it is important to take any recent travel to tropical beaches into consideration, because cutaneous larva migrans is usually acquired from such locations. This information supports the diagnosis and management of dermatological conditions by considering environmental factors and potential infectious exposures related to travel.
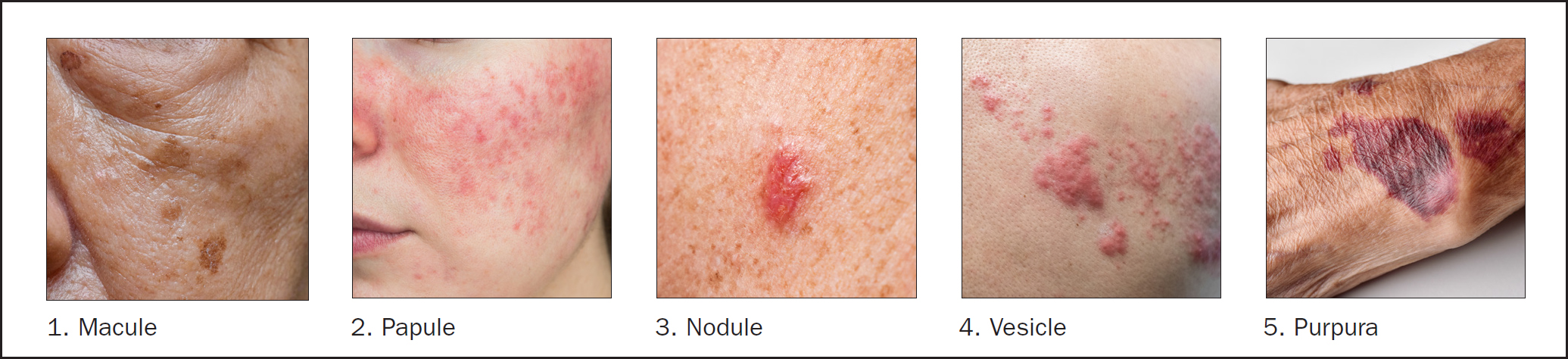
Primary and secondary lesions
Primary lesions (Table 1; Figure 1) are directly associated with a disease process. Secondary lesions (Table 2; Figure 2) are modifications of a primary lesion resulting from evolution of the primary lesion, traumatic injury or other factors (Linton, 2011).

| Lesion | Description |
|---|---|
| Macule | An area of skin that is a different colour or texture and that is flush with the adjacent skin and less than 1cm in diameter, such as in solar lentigo |
| Papule | A lesion that is dome-shaped and less than 1cm in diameter, such as in the case of rosacea |
| Nodule | A firm dome-shaped lesion that is more than 1cm in diameter, suc as a basal cell carcinoma |
| Plaque | A flat-topped raised lesion, with a clearly defined border; more than 1cm in diameter, such as appears in psoriasis |
| Vesicle | Fluid-filled lesion of less than 1cm in diameter. Usually occurs in groups but single lesions may occur, depending on the cause, for example in the case of herpes zoster |
| Bulla | A large, fluid-filled blister, for example a bullous pemphigoid |
| Purpura | A rash of purple spots due to small blood vessels leaking blood into the skin. ‘Petechiae’ refers to lesions of 1mm to 2mm, and ecchymoses are larger lesions. Examples include Henoch-Schönlein purpura and bruises |
| Telangiectasia | Dilated small blood vessels on the surface of the skin, such as appears with basal cell carcinoma and in sun-damaged skin |
| Wheal | A skin rash that appears as red, raised, itchy bumps or welts, an example is urticaria |
Adapted from Akingbola and Vyas, 2021. This is not an exhaustive list
| Lesion | Description |
|---|---|
| Excoriation | Abrasions caused by scratching itchy skin conditions, for example i cases of eczema |
| Scale | Skin conditions that result in scaling, flaking patches, such as in psoriasis |
| Crust | Crusts consisting of dried blood, pus or serum. An example is impetigo |
| Erosion | Breakdown of the epidermis, such as occurs in pemphigus vulgaris |
| Ulcer | The formation of a break in the skin that can lead to the disintegration of tissue. This may occur in venous ulcers and arterial ulcers |
| Fissure | A crack in the skin that can extend to the dermal layer, such as in the case of hand eczema |
| Scar | A mark on the skin after a wound or injury has healed, for example following a surgical incision |
| Keloid | A raised, thick scar, such as in cases of acne keloidalis nuchae |
| Atrophy | Thinning of the skin, for example as the result of corticosteroid overuse |
Adapted from Akingbola and Vyas, 2021. This is not an exhaustive list
Examinations
During a dermatological examination, observing signs such as scratching, agitation or discomfort can indicate underlying pain or irritation. Such behaviours may lead to complications such as skin damage or infection if not promptly addressed. A comprehensive skin examination requires inspecting the entire body under adequate lighting, focusing on areas such as nails, scalp, oral cavity, genital areas and mucous membranes to identify any abnormalities.
The ABCDEFGH system serves as a critical framework for identifying potentially malignant skin lesions, particularly melanoma (Jin, 2024). This method expands upon the well-known ABCDE system by including the characteristics firmness, growth and height, offering practical guidance for clinicians in assessing suspicious lesions. The systematic use of the ABCDEFGH framework ensures that both visual and tactile evaluations are comprehensive, facilitating early detection of malignancies and improved clinical outcomes.
A: asymmetry
Identifying asymmetry during dermatological examinations is essential, because it often indicates malignancy. For example, morphoeic basal cell carcinomas present with irregular borders and asymmetrical growth (Alsayyah, 2023). In cases of melanoma, asymmetry in pigment, size, or shape between two halves of a lesion is a key feature, where one side may be raised or darker, while the other remains flat or lighter. Asymmetry is critical for distinguishing malignant from benign lesions and facilitates early detection.
Additionally, the distribution of lesions offers valuable diagnostic information. Symmetrical patterns typically indicate systemic conditions, whereas asymmetry suggests external triggers such as infections or trauma (Sheikh and Jha, 2024). Different distribution patterns, such as grouped, linear or dermatomal, are indicative of specific conditions such as herpes simplex or herpes zoster. Unilateral lesions, as seen in fungal infections, contrast with symmetrical conditions such as palmoplantar pustulosis. The Koebner phenomenon (which refers to the appearance of new lesions on previously unaffected skin following trauma (Brambilla et al, 2023)) further highlights the diagnostic significance of scars, which may become reactivated in previously damaged skin.
B: border
The border of a lesion is a critical factor in diagnosing malignancy. Benign lesions typically exhibit smooth, well-defined edges, whereas melanoma often presents with irregular, ragged, or blurred borders (Singh, 2022). These irregularities, such as scalloped or notched borders, are indicative of abnormal growth into surrounding tissues. Evaluating the lesion's morphology, whether primary or secondary, aids in accurate diagnosis. Border irregularity, especially when combined with asymmetry, colour variation or rapid growth, necessitates further clinical investigation, because these are hallmark signs of melanoma progression.
C: colour
Assessing colour in skin lesions is important because it provides critical clues about underlying conditions. Different colours can indicate various pathologies or stages of disease (Mittal et al, 2024). For example, erythema (redness) often suggests inflammation or infection, whereas brown or black pigmentation might indicate chronic conditions or malignancies such as melanoma. Changes in colour, such as hyperpigmentation or hypopigmentation, can signal metabolic or systemic disorders (Wang et al, 2023).
Skin lesions and rashes can appear in various colours, depending on the patient's skin tone. For instance, lichen planus may look pink to violet on lighter skin but appear purple to black on darker skin (Madnani, 2023). Common colours seen in skin lesions include brown, black and red. Rashes may be hyperpigmented (darker), hypopigmented (lighter), or depigmented (complete loss of pigment), with hypopigmentation and depigmentation often being less noticeable in lighter skin tones. Erythema, which is redness due to blood vessel dilation, can be blanched with pressure, unlike extravasated blood, which does not blanch during diascopy. Erythema is harder to detect in very dark skin and can be easily missed. Moles can range in colour from flesh-toned to brown or black, with dermal melanin giving a blue-grey hue. A mole with more than two colours should raise suspicion of melanoma.
Colour variation is a hallmark of melanoma. Benign moles usually have a uniform colour, typically tan, brown or black; melanoma lesions may contain different shades of brown, black, pink, red, or even blue or white. A mole with multiple colours or an uneven distribution of pigment is a significant red flag. In particular, the presence of unusual colours such as blue or white may indicate a more advanced stage of melanoma. When assessing colour, it is essential to look for both changes in an existing mole and the presence of multiple colours in new growths.
D: diameter
Lesions larger than 6mm in diameter (about the size of an end-of-pencil eraser) are more likely to be melanoma than smaller lesions. Although melanomas can be smaller than this, diameter is still an important factor to consider. Any mole or lesion growing larger over time, especially beyond this 6mm threshold, should raise concerns. This criterion is particularly useful in combination with the other factors, because size alone does not always determine malignancy. However, growth beyond 6mm typically necessitates further evaluation, especially if accompanied by other suspicious features.
E: evolving
Perhaps the most important factor in the ABCDEFGH model is evolution. If a mole or skin lesion is changing in any way – whether in size, shape, colour, or elevation – it should be closely monitored. This can manifest as rapid growth, changes in the texture (for example becoming rougher or more scaly), bleeding, itching or the appearance of new symptoms such as pain. A stable lesion over time is less likely to be malignant, but a lesion that changes quickly is a strong indicator of potential melanoma and warrants immediate medical attention.
F: firmness
Firmness refers to the texture of the lesion. Melanomas often feel firm or hard to the touch, unlike benign moles, which tend to have a softer, more uniform texture. This criterion is particularly useful in identifying nodular melanomas, which tend to present as firm, elevated lesions. When palpating a lesion, clinicians should note any firm, non-movable qualities that feel different from surrounding skin tissue. The lesion's hardness can indicate deeper skin involvement, suggesting a more advanced or aggressive form of melanoma.
G: growth
Rapid or progressive growth is another critical factor in identifying melanoma. A mole or lesion that grows noticeably over a short period, especially if it is small at the beginning and quickly becomes larger, should raise alarms. Melanomas typically grow both horizontally (across the skin surface) and vertically (deep into the skin layers), making early detection essential. Observation that a lesion is growing not only in diameter but also in elevation or thickness is a strong indication of malignancy, particularly when growth is combined with changes in colour, asymmetry, or firmness.
H: height
Finally, height is an essential part of the ABCDEFGH assessment. A raised lesion, particularly one that has become thicker over time, is often a warning sign. Benign moles are usually flat or slightly raised but stable in their appearance. A melanoma, however, may start as a flat lesion and gradually become more elevated. A lesion that develops an uneven, raised surface, especially if it changes rapidly, should be evaluated. This change in elevation, or height, is a signal that the lesion may be invading deeper layers of the skin, which indicates a more advanced stage of cancer. When an ACP is assessing a patient with a rash or lesion, applying the ABCDEFGH approach helps to quickly identify potential malignancies, prompting further investigation or referral if necessary
Palpation
Palpation is a critical component of dermatological examinations, allowing ACPs to assess both the surface and deeper characteristics of lesions. When examining the surface, palpation can reveal important details about texture; for instance, a lesion might feel smooth such as ecchymoses or rough such as a psoriatic plaque. Simple palpation helps determine the morphology of lesions; running fingers over a rash's border can distinguish a macule from a papule, and gently pinching a lesion between the thumb and index finger can identify a dermatofibroma through characteristic indentation. Applying tangential pressure may elicit pain in a wart, whereas pain with perpendicular pressure is indicative of a corn. The elevation of a lesion is also important, with palpation identifying whether it is flat, raised, or depressed. Crusts, if present, should be examined to see if they can be removed to inspect the underlying tissue, as in psoriasis. Temperature differences, such as the warmth of an abscess, can also be detected through palpation.
In assessing the deeper characteristics of a lesion, consistency is key; lesions may feel hard, firm or soft. Fluctuance can be evaluated by holding the lesion's sides and applying pressure to its centre to check for fluid-filled masses such as cysts. Mobility should be assessed to determine if the lesion is freely movable or tethered to surrounding structures. Lastly, tenderness, often indicating an infective or inflammatory cause, is an important factor to note during palpation. Through these techniques, palpation provides a comprehensive understanding of the lesion, aiding in accurate diagnosis and management.
Scalp and hair, nails and mucus membranes
After completing the skin lesion assessment the ACP should ask the patient if they have noticed any changes in the scalp, hair, nails, and mucus membrane.
Scalp and hair examination
Scalp conditions can be isolated or part of broader dermatoses. For example, seborrhoeic eczema on the face or body is often accompanied by diffuse scaling on the scalp, whereas psoriasis is characterised by adherent, thicker scaling (Trüeb and Gavazzoni, 2023). Various forms of alopecia (hair loss) may present differently; alopecia areata features a non-inflamed scalp with ‘exclamationmark’ hairs at the edges, whereas conditions such as scalp ringworm (kerion) exhibit inflammation and pustulation. Traction alopecia, trichotillomania, lichen planus, systemic lupus erythematosus, and aplasia cutis are other notable causes of localised or scarring alopecia. Generalised alopecia might be due to androgenic alopecia, telogen effluvium (a condition in which hair falls out after stress or illness (Aksoy et al, 2021)), endocrine disorders, iron deficiency, or medication effects such as after taking anticonvulsants or chemotherapy agents (Pitton et al, 2023). Hirsutism, excessive hair growth in women, may be caused by conditions such as polycystic ovary syndrome or Cushing's syndrome (Vyas and Stewart, 2023).
Nail examination
Nails provide essential clues to various medical and dermatological conditions. Psoriasis can present with pitting, ridging, onycholysis and nail loss. Atopic eczema might show pitting and transverse ridging; alopecia areata could cause fine pitting in severe cases (Hamad et al, 2023). Lichen planus often results in longitudinal ridging and thinning of the nail plate, and Darier's disease is characterised by notching of the free edge of the nail. Each of these changes can offer insights into the underlying health issues and guide further diagnostic evaluation.
Mucous membrane examination
The examination of mucous membranes, particularly in the oral and genital areas, is crucial for diagnosing various conditions. For instance, lichen planus can affect these areas, presenting with characteristic lesions. Pemphigus, a group of autoimmune blistering disorders, may also manifest in mucous membranes (Ramírez et al, 2023). A thorough inspection for colour changes, lesions, ulcerations and signs of inflammation in the gingiva, tongue, and buccal mucosa is essential for identifying infections, nutritional deficiencies, or systemic diseases such as anaemia or diabetes mellitus. This detailed examination helps uncover conditions that may not be visible on the skin alone.
Conclusion
A systematic and thorough dermatological assessment is essential for ACPs to provide effective, patient-centred care. Integrating psychosocial evaluations, distinguishing between rashes and lesions, and employing structured approaches such as the ABCDEFGH model allows for precise diagnosis and treatment. Understanding patients' concerns and expectations through the ICE framework enhances communication and patient satisfaction. By combining clinical examination skills with holistic care, ACPs can improve outcomes in dermatological practice and ensure comprehensive patient management.