

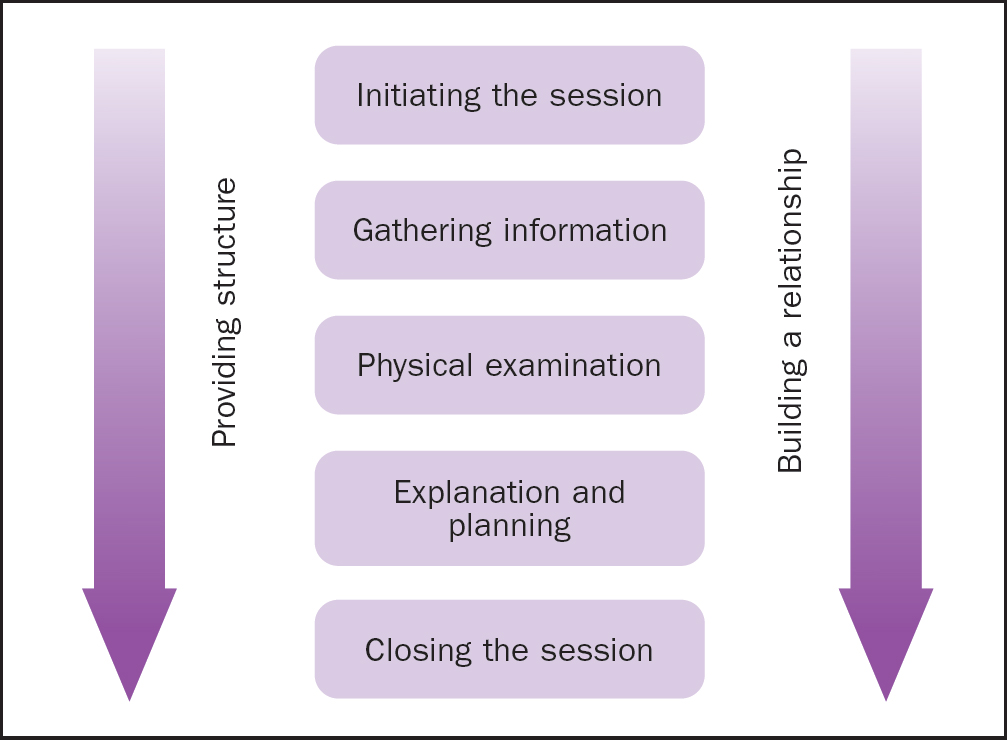
Consultation models provide a structure for the two-way interaction between patient and clinician, usually initiated when the patient is ill. Seminal work has been used in this case study as there is limited evidence for nurses' consultation styles. There is a variety of consultation models, from medically focused ones (Byrne and Long, 1976) to more shared approaches (Silverman et al, 2013; Neighbour, 2017). The Calgary-Cambridge Model, developed by Silverman et al (2013), is used widely to teach consultation skills. It comprises five steps (Figure 1):
For the purpose of this case study, this model is used to critically analyse a consultation with a patient referred by his GP to a surgical assessment unit, following a history of abdominal pain. This model was chosen because it is structured, patient-centred and facilitates shared decision-making.
Applying the Calgary-Cambridge Model
Initiation of the session
The first stage of the model is initiation where patient and clinician identify themselves, rapport is quickly established and the confidence of the patient is gained (Silverman et al, 2013). The second author introduced himself as a trainee ACP working under the supervision of his supervisor, and consent was gained for the consultation to go ahead. To ensure confidentiality all identifiable patient information has been anonymised.
Gary Dean (not the patient's real name) explained that over the past 48 hours he had been experiencing abdominal pain. The use of open questions within the ‘golden minute’ at the start of a consultation can help elicit information about the problem by simply listening to the patient speaking about their concerns without interruption. Using closed questions could mean that much of the patient's history is not conveyed and therefore lost; this can have a detrimental impact on the outcome of a consultation because 80% of diagnoses can be made from history-taking alone (Keifenheim et al, 2015).
Information gathering
The second stage of the model is information gathering from both a biomedical and a patient perspective (Louw et al, 2020). Encouraging the patient to describe their symptoms and expectations is key to recognising differential diagnoses (Ashworth, 2022), the process whereby clinicians consider the possible causes of patients' presenting complaint before making a final diagnosis.
Mr Dean described how he had been awakened in the early hours of the morning by a sharp central abdominal pain, and that he had felt feverish and nauseated. He was immediately fearful of the recurrence of an umbilical hernia, despite previous mesh repair. Using the pain assessment mnemonic SOCRATES (Table 1) (Gregory, 2019), he described how the fever and nausea had settled, but he had persistent loss of appetite, and the pain had now gravitated towards his right groin.
| S | Site | Where exactly is the pain? |
| O | Onset | What was the patient doing when the pain started? |
| C | Character | What does the pain feel like? |
| R | Radiates | Does the pain go anywhere else? |
| A | Associated symptoms | For example, nausea and vomiting |
| T | Time/duration | How long have they had the pain? |
| E | Exacerbating/relieving factors | Does anything make the pain worse or better? |
| S | Severity | Obtain an initial pain score |
Source: Gregory, 2019
Appendicitis typically presents with a sharp central abdominal pain that gravitates to the right iliac fossa, where the appendix is located (Ford, 2019; Moris et al, 2021). Typical presentation also includes nausea, vomiting, loss of appetite and low-grade fever. Red flags are signs or symptoms of serious underlying pathology: those for appendicitis include abdominal pain, nausea, fever and vomiting. However, other differential diagnoses need to be considered, such as those of a surgical, medical or urological aetiology (Lotfollahzadeh et al, 2024).
Investigations
Mr Dean's vital signs were unremarkable (Table 2).
| Vital signs | Patient's observations | Normal range |
|---|---|---|
| Temperature | 36.1°C | 36.1–37.2°C |
| Blood pressure | 128/82mmHg | 90/60mmHg–120/80mmHg |
| Respiratory rate | 20 breaths per minute | 12–18 breaths per minute |
| Heart rate | 75 beats per minute | 60–100 beats per minute |
| SpO2 | 98% on room air | 95–100% |
| Blood sugar | 5.1 mmol/L | 4.0–7.8mmol/L |
There are no specific diagnostic blood markers for acute appendicitis. Mr Dean's blood results (Table 3) demonstrated elevated C-reactive protein (CRP) and white blood cell count (WBC). This indicates infective or inflammatory processes, which can cause acute abdominal pain; however, they have poor specificity (Gans et al, 2015). Mr Dean had normal alanine aminotransferase (ALT) and alkaline phosphatase (ALP) results, making post-hepatic disease unlikely as the cause of his pain, especially in the absence of jaundice (Blann, 2013). Pancreatitis could be excluded based on a normal amylase.
| Test | Result | Normal value |
|---|---|---|
| Sodium | 138 | 133–146mmol/L |
| Potassium | 4.7 | 3.5–5.3mmol/L |
| Urea | 5.9 | 2.5–7.8mmol/L |
| Creatinine | 106 | 59–104μmol/L |
| eGFR | 65 | 90 |
| CRP | 74.8 | 0–5mg/L |
| Albumin | 41 | 35–50g/L |
| ALP | 101 | 30–130U/L |
| ALT | 23 | 0–48U/L |
| Bilirubin | 16 | 0–21μmol/L |
| Amylase | 99 | 15–90U/dL |
| Hb | 166 | 130–180g/dL |
| WBC | 11.9 | 4–11 × 109/L |
| Platelets | 299 | 150–450 × 109/L |
| MCV | 83.8 | 80–100fl |
| INR | 1.1 | 0.8–1.2 |
| APTT | 1.17 | 0.8–1.17 seconds |
ALP=alkaline phosphatase, ALT=alanine aminotransferase, APTT=activated partial thromboplastin time, CRP=C-reactive protein, eGFR=estimated glomerular filtration rate, INR=international normalised ratio, MCV=mean cell volume, WBC=white blood cell count
Urinalysis (Table 4) revealed a trace of blood and 1+ of protein above baseline. Although the presence of leucocytes and nitrites are good indicators for the presence of infection, the absence of nitrites does not necessarily mean that an infection can be excluded. Apart from lower abdominal pain, Mr Dean did not describe any lower urinary tract symptoms such as dysuria, therefore, a urine sample was not sent for culture.
| Test | Normal value | Result |
|---|---|---|
| Colour | Yellow/amber/clear | Clear, light yellow |
| pH | 5.0 to 9.0 | 8.0 |
| Leucocytes | Negative | Negative |
| Nitrites | Negative | Negative |
| Protein | Negative/trace | +1 |
| Glucose | Negative | Negative |
| Ketones | Negative | Negative |
| Blood | Negative/trace | Trace |
| Specific gravity | 1.010 to 1.025 | 1.009 |
Although not usually included in an abdominal assessment, the inflammatory marker procalcitonin has been shown to have greater diagnostic efficacy in identifying appendicitis (Yu et al, 2013), which can be complicated by the probable presence of perforation or gangrene. Unlike uncomplicated appendicitis, complicated appendicitis cannot be managed non-operatively.
Physical examination
The third and fourth stages of the Calgary-Cambridge Model is physical examination, explanation and planning (Denness, 2013). Alongside this, building the relationship and providing structure run as threads throughout the consultation (Figure 1) (Silverman et al, 2013). As Mr Dean's symptoms were abdominal, the gastrointestinal system was the focus for his examination.
The usual sequence for examination is inspection, palpation, percussion and auscultation (Mealie et al, 2024). However, according to Jarvis (2019), in the case of abdominal examination, the sequence is reversed following inspection, arguing that percussion and palpation could stimulate peristalsis: this could cause falsely positive hyperactive bowel sounds, if auscultation is left until last. However, when auscultation is performed before palpation and before percussion, this has been shown not to alter the frequency of bowels sounds (Çalış et al, 2019).
Abbott et al (2014) stressed the importance of maintaining privacy and dignity to reduce anxiety and the effect that this may have on body function, in accordance with the Nursing and Midwifery Council (2018)Code, which states that nurses must respect people's right to privacy and confidentiality. The use of personal protective equipment in keeping with appropriate infection control measures were used. Each element of the examination was explained to Mr Dean to ensure that he understood what was happening without being overwhelmed, because receiving such information can lead to increased anxiety.
The Calgary-Cambridge Model has been criticised by Da Costa et al (2020) for paying little attention to the clinical environment. Caldwell (2019) advised that a consultation should occur in a quiet, private environment where the clinician and patient are both fully prepared for the encounter, where the patient should feel unhurried and in where they can be listened to attentively by the clinician. There should also be facility for the patient to lie flat, because a supine position is necessary for the abdominal examination. Much information can be gained simply by observing the patient enter the room, such as general appearance, gait, consciousness level, tone of voice, posture, facial expression and grooming.
Although the physical examination would focus on Mr Dean's abdomen, the clinician needed to be cognisant that there could be non-abdominal signs elsewhere on the body of gastrointestinal pathology (Abbott et al, 2014).
General inspection
Mr Dean appeared well groomed, was alert and oriented. He had a high body mass index at >30 and was obviously in pain when moving to sit on the treatment couch.
Abdominal examination
Inspection
There are a number of approaches to undertaking an inspection of a patient's abdomen. Mealie et al (2024) recommend that it should be done from the foot end of the bed. Local policy may be different, with the University College London Medical School (UCL) (2015), for example, suggesting dividing the abdomen into nine segments for examination. However, according to Jarvis (2019), the nine-segment approach is archaic and quadrants are much simpler to assess.
The observer must check for symmetry, scarring, distension, prominent veins, hernias, visible peristalsis (obstruction) or pulsation (abdominal aortic aneurysm). If distension is present, the clinician should ask the patient whether this is normal and, if not, screen for ascites.
In Mr Dean's case, his protuberance was normal for him and adipose rather than fluid filled, with no evidence of a fluid wave or bulging flanks when lying flat. Due to abdominal tension, Mr Dean found it difficult to lie completely flat and, on the advice of the ACP's supervisor, he was encouraged to flex his hips at 45° with knees bent at 90° (Oxford Medical Education, 2016). Apart from the rounded abdomen, the only notable abnormality was evidence of an old horizontal surgical scar laterally right of the umbilicus, and some laparoscopic site scarring around the umbilicus and in the right upper quadrant. Post-laparoscopic intra-abdominal adhesions are a common cause of small bowel obstruction (ten Broek et al, 2018) which, like appendicitis, is a key differential in the acute abdomen (a condition needing urgent attention) (Patterson et al, 2023). However, this was unlikely in Mr Dean's case because he had not reported any changes in bowel habit.
Auscultation
Auscultation of the abdomen with a stethoscope is performed to identify altered bowel sounds. Had bowel sounds been absent on auscultation for a full 5 minutes then, ominously, bowel obstruction, perforation, ischaemia and infarction could all be indicated. Felder et al (2014) concluded that auscultation of bowel sounds in clinical practice is not useful in determining what is normal or pathological because the listener frequently misinterprets the sounds. This is because there is no standardised method or empirical evidence base to support auscultation of the abdomen and further research is needed to provide clinicians with more definitive advice.
When using a stethoscope, it is unclear whether it is more effective practice to listen, albeit impractically, to all four quadrants of the abdomen for up to 5 minutes each or to auscultate just to the right of the umbilicus for 2 minutes, the preferred choice for the clinician as the rate of bowel sound is 2–5 min (Zuin et al, 2017; Mealie et al, 2024). Advice by Jarvis (2019) is to place the diaphragm of the stethoscope lightly in the right lower quadrant over the ileocecal valve because bowel sounds, if present, can normally be heard here. The author opted to auscultate just to the right of the umbilicus and found Mr Dean's bowel sounds to be diminished rather than hypoactive, which could indicate decreased gastrointestinal activity.
Auscultation for other abdominal pathology – including a friction rub over a potentially enlarged liver or spleen, or vascular bruit (atherosclerosis) – using the bell of the stethoscope – was not possible due to Mr Dean's body size.
Percussion
Mr Dean's abdomen was percussed by pressing the left middle finger firmly against the abdominal wall and striking the phalanx with the pad of the right middle finger. Light percussion in all four quadrants heralded tympanic sounds, usually heard in the air-filled structures of the supine abdomen, with some dullness over adipose tissue (Jarvis, 2019). The maximal point of percussion tenderness in the right lower quadrant, two thirds of the way from the umbilicus to the anterior superior iliac spine, represents McBurney's point (a location used as a guide to determine the position of the appendix) (National Institute for Health and Care Excellence (NICE), 2024). If this is identified as the point of maximum tenderness, as in Mr Dean's case, this is indicative of acute appendicitis.
Palpation
The key part of the physical examination in diagnosing appendicitis is palpation. Palpation helps to distinguish the difference between subjective pain and objective tenderness. If the clinician can pinpoint tenderness, then the differential diagnoses may be narrowed down. Palpation should be performed with the examiner seated or kneeling to the right of the supine patient, so that their hand and arm can be held horizontally to the patient's abdomen. It should be done superficially at first with the fingertips, and start at the furthest area from the point the patient has identified to be of maximal tenderness (Jarvis, 2019).
The aim of light palpation is not solely to elicit tenderness but also to detect abnormalities in the abdominal wall, such as masses, crepitation or spasm. The patient should be as relaxed as possible and the clinician may want to employ distraction techniques when determining whether the origin of the pain is functional or organic. Keeping the patient's knees and hips flexed helps to relax the abdominal muscles, while moving to deeper palpation with the palmar surface of the hand. In Mr Dean's case, the absence of any mass was confirmed by deep palpation performed using the flexor surface of the second author's fingers with the right hand tilted at an angle and the left hand placed on top.
As with percussion tenderness, signs of guarding and rebound tenderness are indicators of peritonis (NICE, 2024). Guarding is defined as an involuntary muscular protective mechanism by Jarvis (2019), and Lotfollahzadeh et al (2024) cited its occurrence on slight pressure to the right iliac fossa as an indication for peritonitic appendicitis. Although Mr Dean displayed some reactive muscular tension on light palpation of his right iliac fossa, there was an absence of a brief worsening, or rebound, of pain on its release, suggesting peritonism was equivocal (Bjørsum-Meyer and Schmidt, 2013). However, Mr Dean did experience pain in his right lower quadrant when deep pressure was applied to his left lower quadrant, which indicated a positive Rovsing's sign, which is another red flag for appendiceal inflammation (Rastogi et al, 2018). Rovsing's sign is a manoeuvre that involves deep palpation to attempt to distend the caecum and appendix. It is not merely a case of pressing on the left iliac fossa to cause irritation in the right. Manipulation of the right leg to irritate the psoas or obturator muscles are also positive signs for appendicitis; however, these were not formally undertaken because Mr Dean was observed to be in discomfort as he was lifting his legs onto the treatment couch.
Diagnosis
Diagnosis of acute appendicitis is based on a set of observations linked with theory. Its aetiology is largely unknown but it is thought to be caused by luminal obstruction (NICE, 2024). Although abdominal examination is an essential component of physical assessment, it has been increasingly replaced by imaging modalities (Mealie et al, 2024).
Computerised tomography (CT) is useful, as it was in Mr Dean's case, for identifying appendicitis; however, routine use of CT is not well established (Rud et al, 2019]). Should a diagnosis be apparent from the history taking, physical examination and blood results, surgery should not be delayed by a wait for imaging. Appendicectomy remains the ‘gold standard’ for uncomplicated appendicitis (Gorter et al, 2016; Krzyzak and Mulrooney, 2020). According to Di Saverio et al (2020), in cases of uncomplicated appendicitis, delays to surgery can progress to perforation, with associated higher rates of morbidity and mortality, and general surgeons are likely to choose to operate if diagnosis is probable rather than definite.
Implications for practice
The trainee ACP has learnt from this supervised process that the true value of the clinical consultation lies in the ability of the clinician to interpret, verbally and non-verbally, what the patient is communicating (Caldwell, 2019). It is important to note that many patients may well not be as eloquent or at ease in expressing themselves within the clinical context as Mr Dean. Furthermore, appendicitis may present more atypically than in Mr Dean's case and will be difficult to diagnose (Echevarria et al, 2023). For example, an older adult may require a more comprehensive physical examination due to concurrent comorbidities and their frailty may be present difficulties in communication (Omari et al, 2014).
Therefore, following history-taking, there may need to be an assessment of all systems without the focus being exclusively on the abdomen (Bakopoulos et al, 2022). Krom (2020) acknowledged health assessment skills are key to the increasing clinical autonomy of nurses' work. As such, nurses have a legal obligation to provide a level of care that is deemed acceptable (Dowie, 2020). A non-reductionist, holistic approach to health care is vital in transforming service delivery to better meet individual health needs, as illustrated by the case study (Health Education England, 2021), which is a key focus of the NHS Long Term Plan (NHS England, 2019).
Conclusion
The trainee ACP used the Calgary-Cambridge Model (Silverman et al, 2013) to structure a consultation with a 63-year-old-man referred by his GP to a surgical assessment unit following a 2-day history of abdominal pain. Mr Dean had presented with classic symptoms of uncomplicated appendicitis and was not acutely distressed. Pain began peri-umbilically before migrating to the right iliac fossa and, on examination, the patient was positive for McBurney's point and Rovsing's sign (Abbott et al, 2014). Initial fever, elevated CRP and WBC were contributors to diagnosis, with the differential of urinary tract infection excluded. Mr Dean's hands displayed no evidence of liver impairment, his sclera were non-icteric, conjunctiva not pale and oral mucosa was intact.
A CT supported the examination findings and Mr Dean underwent a timely laparoscopic appendicectomy. The application of a consultation model helped the trainee ACP to structure the consultation between the patient and the clinician and facilitated shared decision-making.