
Exploring and achieving peoples' preferences for place of care and death are acknowledged to influence the quality of end-of-life care (Department of Health (DH), 2008; 2010; Macleod, 2011, National Institute for Health and Care Excellence (NICE), 2015; 2019). Achieving preferred place of death has become a marker of the quality of end-of-life-care (DH, 2010; Macleod, 2011) with existing evidence claiming that most people wish to die at home (Gomes et al, 2012). However, some literature and anecdotal evidence challenges this orthodoxy and proposes that alternatives are needed as the concepts of preference and choice are complex (Hoare et al, 2015; Pollack, 2015). This article will provide a practical overview, explore the key considerations and the role of the nurse in effective discharge planning for patients who have expressed a wish to die at home. This will be done by using the ‘five priorities of care for the dying person' (Leadership Alliance for the Care of the Dying Person (LACDP), 2014) as a framework to promote safe discharge in end-of-life.
Priority 1: recognition
Recognising that a patient may be nearing the end of their life is a key consideration. Early recognition of dying is vital to allow for discussions to be started about the patient's wishes, for example their preferred place of death and for discharge planning to be initiated (NICE, 2019). If recognising dying is delayed, then there is a risk that the patient's wishes may not be identified soon enough and discharge home may not be achieved.
Rapid discharge home in the patient's last days of life is possible and involvement of local specialist palliative care teams can be helpful (NHS England, 2015). A senior doctor should assess the patient if there has been a sudden or unexpected deterioration in a patient's condition to ascertain whether the deterioration is potentially reversible, or confirm that the patient may be dying (LACDP, 2014).
Priority 2: communication
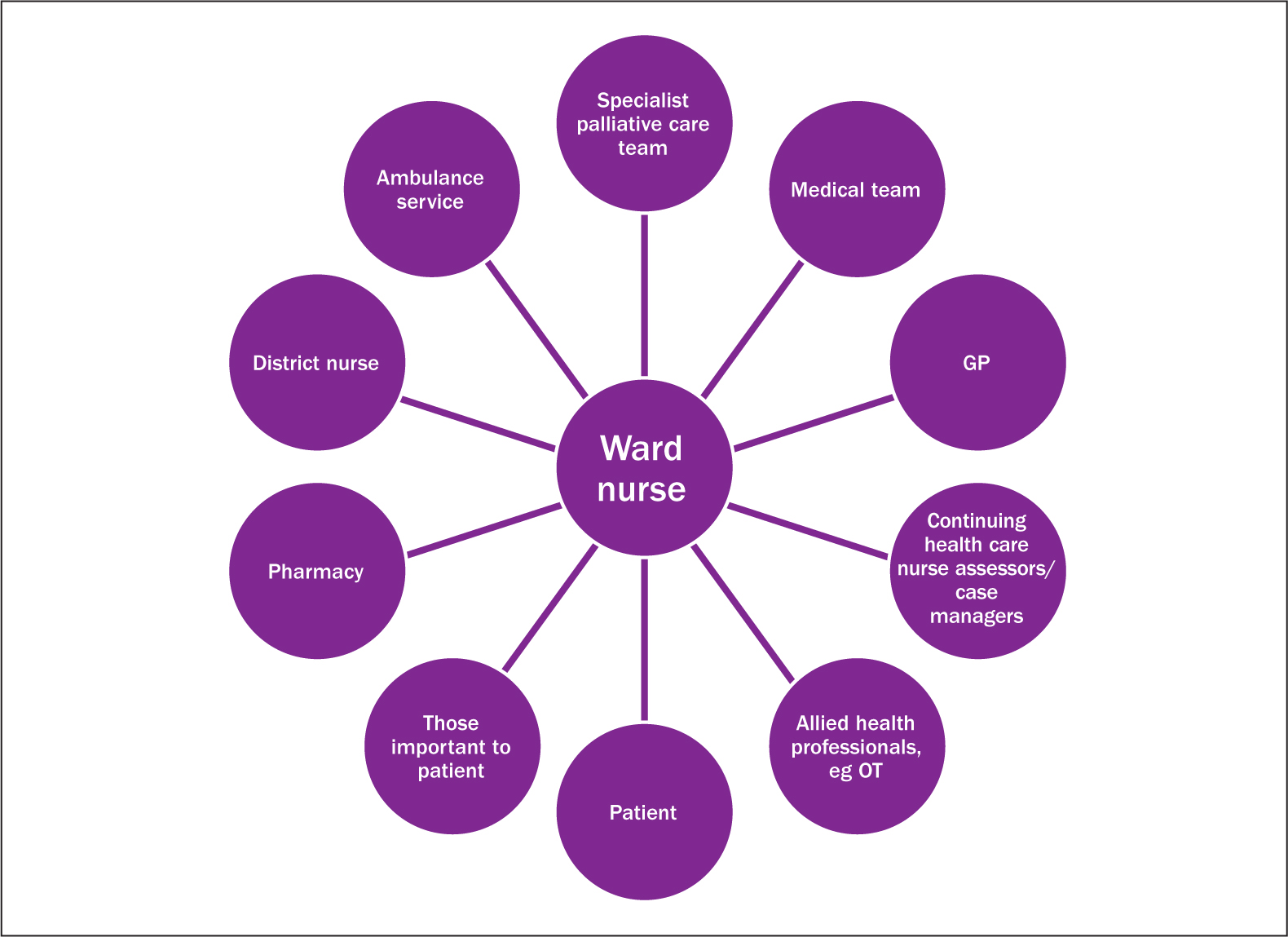
Sensitive communication needs to take place between the dying person, those identified as important to them and members of the health care team. Early, effective communication, both verbal and written, is essential to aid a seamless transition of care. It ensures that patients receive timely, coordinated care, with involvement from the appropriate services and members of the multidisciplinary team (Figure 1). If a patient is expected to die soon, there needs to be an explanation about how death might be expected to occur, while accepting the uncertainty of the prognosis, and discussing the plan of care and giving the dying person (and those identified as important to the dying person) the opportunity to ask questions (LACDP, 2014). It is also important to discuss with the patient and their family, the potential risk of dying in transfer to their preferred place of death.
Priority 3: involvement
Patients have a right to be involved in decisions about their care and consideration should be given to the extent of the patient's desired involvement. Appropriate information should be given to allow decisions to be made and should include those important to the patient and carers (DH, 2015). There are national initiatives such as ReSPECT (Recommended Summary Plan for Emergency Care and Treatment) (Resuscitation Council, 2019), which is aimed at encouraging patients and their families to be involved in decision-making in order to ensure that they receive the right care and treatment in a future emergency. Important conversations to have may include, do not attempt cardiopulmonary resuscitation (DNACPR), advance decision to refuse treatment (ADRT) and emergency health care plans (EHCP). There may be occasions where patients lack the capacity to make a decision regarding preferred place of death, and in this situation, decisions should follow a best interest process.
Priority 4: support
Caring for a dying relative or friend at home can place an enormous strain on people. What can appear routine, normal everyday practice to health professionals can be challenging to family members as they may not have experienced caring for someone before. Research has shown that the odds of a patient dying at home are reduced by two-thirds if carers prefer otherwise or are reluctant to support on discharge (Grande and Ewing, 2008; Alonso-Babarro et al, 2011). Therefore, nurses have a responsibility to emotionally support the family by preparing them for the possibility that the patient will die at home, and allowing them to voice any fears or concerns that they may have regarding discharge. From a practical perspective, the family should be provided with:
Priority 5: plan and do
Once the decision has been made for discharge home, and priorities 1–4 have been implemented, an individual plan of care must be devised in order to ensure that the patient's individual needs are addressed.
Case study
The following case study illustrates a safe, rapid discharge home for end-of-life care. In order to preserve confidentiality in line with the Nursing and Midwifery Council (NMC) (2018), the patient's name has been changed.
Sally was a 72-year-old woman with metastatic lung cancer. She had been admitted to hospital with increasing shortness of breath and chest pain. She was diagnosed with community acquired pneumonia and was started on intravenous antibiotics and oxygen. Despite these treatments, she continued to deteriorate, and the ward team recognised that Sally was dying. A DNACPR was implemented and this was clearly communicated to Sally and her family. During this discussion, Sally identified that her preferred place of death was home; this decision was supported by her family. Anticipated emergencies, such as increasing shortness of breath were discussed, and an EHCP was written. Box 1 shows the steps that facilitated Sally's safe discharge within 24 hours.
Sally died peacefully 3 days later at home surrounded by her family. While understandably sad at losing their loved one, they were grateful that her wish to die at home had been achieved.
Conclusion
This article has highlighted the key considerations for facilitating a safe and timely discharge home for end-of-life care. The nurse has a pivotal role in communicating, collaborating and coordinating the discharge, to ensure a seamless transition from hospital to community, ensuring that preferred place of death can be achieved.