
Intermediate life support (ILS) refers to a range of skills that are used to treat adult patients during cardiopulmonary arrest until experienced assistance arrives (Resuscitation Council UK, 2016). Although these skills are predominantly used in the acute hospital environment, they may also be used in other clinical settings, depending on the availability of equipment such as defibrillators. ILS includes effective basic life support (BLS), which was discussed in a previous article (Barker, 2019). This article will focus on the ILS skills of early recognition of deterioration, airway management and defibrillation.
Early recognition of deterioration
Up to 80% of patients suffering cardiac arrest display evidence of deterioration in the hours before arrest; once a cardiac arrest occurs, even in the hospital environment, fewer than 20% of patients will survive until discharge (Resuscitation Council UK, 2016). Early recognition of deterioration and a call for help therefore form the first link of the Chain of Survival (Nolan et al, 2006). The Resuscitation Council UK (2016) advocates the use of a scoring system to aid the responder in identifying the deteriorating patient. The currently used system in the UK is the National Early Warning Score 2 (NEWS2) instituted by the Royal College of Physicians (2017). This provides a score based on 5 numeric observations but, in addition to the previous version, includes the patient's level of consciousness using the ACVPU scale (alert, confused, voice, pain, unresponsive) (Table 1). NEWS2 and other early warning systems (EWS), also empower the patient's assessor to seek appropriate senior support when deterioration is identified. A study by Spearpoint et al (2009) found no significant change in the number of emergency alert calls made by hospital staff following inclusion of such a system of recognition in ILS training. However, this study recognised that the proportion of pre-arrest calls increased from 15% to 45%; a reduction in the numbers of in-hospital cardiac arrests was observed, as was a reduction in the number of unsuccessful resuscitation attempts.
| A | Alert | Patient is fully awake |
| C | New confusion | New-onset confusion, disorientation, delirium or any other acute alteration to mentation (in acutely ill patients, confusion should be assumed to be ‘new’ until confirmed otherwise) |
| V | Voice | Patient responds in some way (eye/voice/motor) when spoken to |
| P | Pain | Patient only shows response to pain stimulus |
| U | Unresponsive | Unresponsive to all stimuli (‘unconscious’) |
Airway management and ventilation
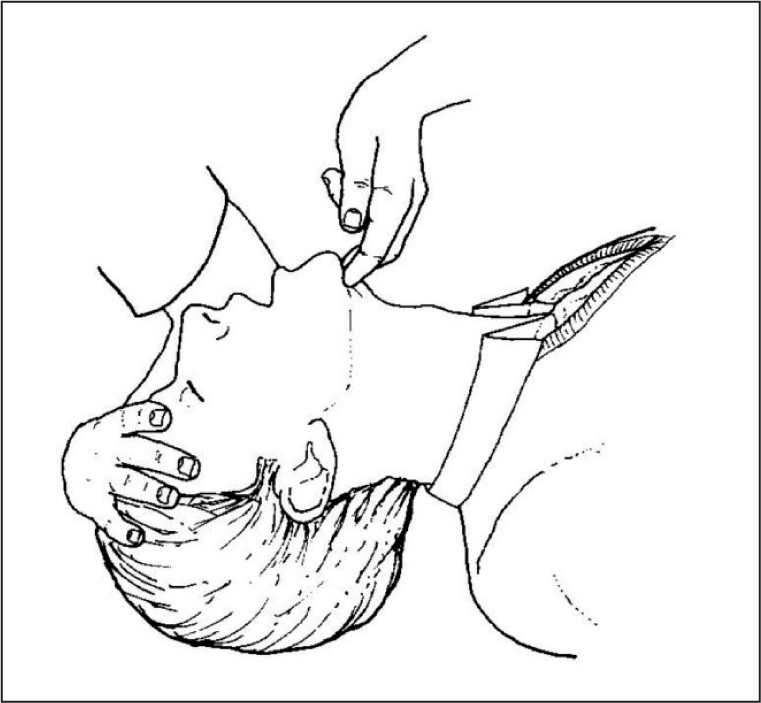
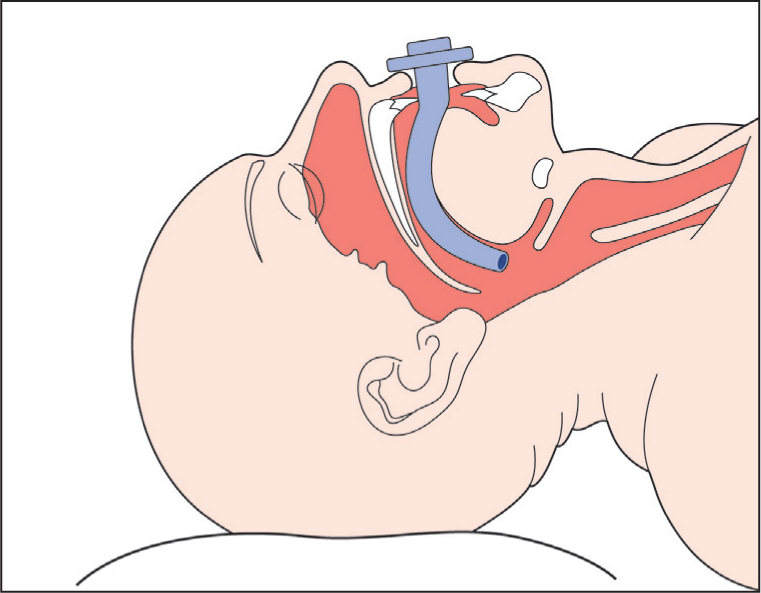
The airway of an unconscious patient may become occluded as a reduction in muscle tone can lead to a collapse of the soft tissue around the airway; the most common site for this is the pharynx. Basic manoeuvres such as the head tilt, chin lift (Figure 1) can open the airway. ILS takes this further by including the use of oropharyngeal (Figure 2) and nasopharyngeal airways, which are useful aids to preventing soft palate or tongue obstruction of the airway during resuscitation (Resuscitation Council UK, 2016).

Oropharyngeal airway sizes 2, 3 and 4 are commonly used for small, medium and large adults respectively; this decision can also be made by selecting an airway equal in length to the vertical distance between the patient's incisors and the angle of their jaw (Resuscitation Council UK, 2016). Before inserting the device, the patient's airway should be inspected to ensure there are no objects that could be pushed back into the patient's larynx. The device is then inserted ‘upside-down’, with its end pointing towards the roof of the patient's mouth. As the device is moved past the hard roof of the mouth, it should be rotated by 180° so that it follows the direction of the patient's airway. This technique is used to prevent the tongue being pushed back into the airway (Resuscitation Council UK, 2016). If the patient resists the insertion of the oropharyngeal airway, or later becomes intolerant of it, they do not need it. Once inserted, look, listen and feel to check the patency of the airway. Figure 3 shows an oropharyngeal airway in place.
Alternatively, a nasopharyngeal airway may be better tolerated, or more appropriate for patients with maxilla-facial injuries or clenched jaws. However, they are unsuitable for patients with basal skull injuries. Sizes 6-7 mm are normally appropriate for adults (Resuscitation Council UK, 2016). The airway should first be lubricated with water-soluble jelly. It should then be inserted in to the nostril bevel-end first, with a gentle twisting motion as it is advanced (Resuscitation Council UK, 2016). Should resistance in one nostril be encountered, the other one can be tried. The flanged end should not be advanced beyond the nostril opening. Once again look, listen and feel to check the patency of the airway (Resuscitation Council UK, 2016).
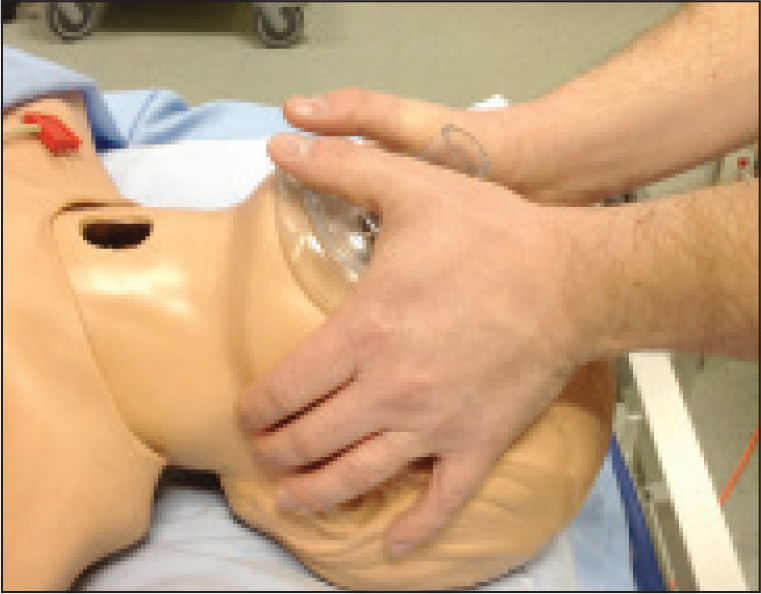
In addition to airways, a pocket mask, or a self-inflating bag, valve and mask may be used to aid ventilation. These make mouth-to-mouth resuscitation unnecessary and allow supplementary oxygen to be administered. With either device, it is important that a seal is maintained between the mask and the patient's face. First, open the patient's airway using the head-tilt, chin-lift manoeuvre. Position the mask over the patient's face; the pointed end of the mask goes over the patient's nose, the lower edge sits between their chin and bottom lip. Then press down on mask with your thumbs, while pulling the patient's jaw upwards in to the mask to create the seal while maintaining the patient's head position (Figure 4). Then, when using the pocket mask, breathe into the mask's valve for 1 second so that the patient's chest rises. When using the self-inflating bag, it is difficult to maintain the seal and squeeze the bag; it is therefore advised that this is used as a two-person device: the second rescuer squeezes the bag while the first maintains the seal. With either device, or BLS, the aim is to see the chest rise by around 2 cm (Barker, 2019). The full volume of the self-inflating bag will be excessive in most patients.
Defibrillation
Defibrillators are used to terminate cardiac arrhythmias that prevent the heart from pumping blood. They do this by stopping the unwanted electrical activity of these arrhythmias, thus allowing the heart's normal rhythm to resume control (Resuscitation Council UK, 2016; Resuscitation Council UK and British Heart Foundation, 2017). Specifically, arrhythmias requiring defibrillation are ventricular fibrillation (VF) and pulseless ventricular tachycardia (VT). Defibrillation cannot be used for asystolic arrests or pulseless electrical activity.
VF is characterised by irregular, rapid, bizarre waves due to random electrical activity in the myocardium. VT is characterised by broad, regular complexes at a rate above 100 per minute. At lower rates, patients may have sufficient consciousness and a pulse; these patients require immediate attention and close monitoring but should not be defibrillated unless the pulse is lost (Resuscitation Council UK, 2016).
Once help has been summoned, performing effective BLS should take priority over finding a defibrillator (Resuscitation Council UK, 2016). However, the sooner the patient receives defibrillation, the better their chances of survival (Chan et al, 2008), so any available helpers can be directed to seek a defibrillator while BLS is performed.
Some specialist units continue to use manual defibrillators. However, many trusts now use automated external defibrillators (AEDs); these are also often available in public places. Research has shown AEDs demonstrate a high level of accuracy in distinguishing between shockable and non-shockable rhythms (Jekova et al, 2009). These devices will not recommend a shock (or charge) unless they detect a shockable rhythm.
To use an AED, the unconscious patient's chest must first be exposed. Once switched on, many AEDs will provide audible instructions for the rescuer. The pads should then be applied to the patient's chest. Pads may have pictures on them identifying the sites to which they should be applied; one is applied below the patient's right clavicle, the other to the left, lower portion of the patient's rib cage. Once these have been applied the pads should be plugged into the AED itself. If more than one rescuer is present, chest compressions should not be interrupted while the AED is attached (Resuscitation Council UK, 2016). However, once attached, compressions must be interrupted to allow the AED to analyse the heart rhythm. Once it has done this, it will either instruct rescuers to resume chest compressions, or recommend a shock and proceed to charge itself in preparation for this.
The AED will not deliver an inappropriate shock to an unconscious patient. However, there are some safety considerations for others of which the rescuer must be aware. The rescuer must clearly communicate to anyone nearby that they are about to defibrillate. They must quickly check that no one (including the person using the AED) is touching the patient, the patient's bed frame, trolley, or any equipment attached to the patient such as infusions. They must also make sure that any devices with oxygen flowing through them (such as the self-inflating bag, or an oxygen mask), is at least 1 metre away. Finally, they should also make sure that there is no risk of conduction of electricity through liquid in which the patient may be lying, such as water or urine. Once satisfied that it is safe to do so, they should press the shock button on the AED.
Once a shock has been delivered, the rescuer should restart cardiopulmonary resuscitation and continue for 2 minutes, which the defibrillator will time, before reassessing the patient's heart rhythm (Resuscitation Council UK, 2016). It may then advise another shock. If, during this time, the patient exhibits signs of life, they should be reassessed using the ABCDE (airway, breathing, circulation, disability and exposure) approach (Resuscitation Council UK, 2015).
Conclusion
The skills detailed in this article can be used alongside effective BLS skills to optimise the likelihood of a patient surviving a cardiac arrest. In particular, early recognition of deterioration leading to an early call for help, and early defibrillation, form key links in the chain of survival. However, high-quality chest compressions remain of paramount importance in resuscitation, and it must be emphasised that any interruption to these must be minimised.