This website is intended for healthcare professionals
Search menu
References
Ballard J, Bergan J Chronic venous insufficiency: diagnosis and treatment.(eds). London: Springer–Verlag; 2000
Brodovicz KG, McNaughton K, Uemura N, Meininger G, Girman CJ, Yale SH. Reliability and feasibility of methods to quantitatively assess peripheral edema. Clin Med Res.. 2009; 7:(1-2)21-31 https://doi.org/10.3121/cmr.2009.819
Clarke GH, Vasdekis SN, Hobbs JT, Nicolaides AN. Venous wall function in the pathogenesis of varicose veins. Surgery. 1992; 111:(4)402-408
Eklöf B, Rutherford RB, Bergan JJ Revision of the CEAP classification for chronic venous disorders: a consensus statement. J Vasc Surg.. 2004; 40:(6)1248-1252 https://doi.org/10.1016/j.jvs.2004.09.027
Londero LS, Lindholt JS, Thomsen MD, Hoegh A. Pulse palpation is an effective method for population-based screening to exclude peripheral arterial disease. J Vasc Surg.. 2016; 63:(5)1305-1310 https://doi.org/10.1016/j.jvs.2015.11.044
Moffatt C., Martin R, Smithdale R. Leg ulcer management: Essential clinical skills for nurses.Oxford: Blackwell; 2007
Nakano LCU, Cacione DG, Baptista-Silva JCC, Flumignan RLG. Treatment for telangiectasias and reticular veins. Protocol for Cochrane review. Cochrane Database Syst Rev.. 2017; 7 https://doi.org/10.1002/14651858.CD012723
National Institute for Health and Care Excellence. Varicose veins: diagnosis and management. Clinical guideline CG168. 2013. https://www.nice.org.uk/guidance/cg168 (accessed 18 December 2019)
National Institute for Health and Care Excellence. Leg ulcer–venous: management scenario. Clinical Knowledge Summaries. 2019. https://cks.nice.org.uk/leg-ulcer-venous (accessed 16 December 2019)
Padberg FT, Johnston MV, Sisto SA. Structured exercise improves calf muscle pump function in chronic venous insufficiency: a randomized trial. J Vasc Surg.. 2004; 39:(1)79-87 https://doi.org/10.1016/j.jvs.2003.09.036
Radak DJ, Tanaskovic SZ, Vlajinac HD, Marinkovic JM, Maksimovic MZ. Relationship between pain and CEAP C categories of chronic venous disease. Angiology. 2016; 67:(7)670-5 https://doi.org/10.1177/0003319715613179
Staines K. Safe compression and accurate ABPI—overcoming barriers. Wounds UK. 2018; 14:(1)64-67
Vowden P, Vowden K. The importance of accurate methodology in ABPI calculation when assessing lower limb wounds. Br J Community Nurs.. 2018; 23:S16-S21 https://doi.org/10.12968/bjcn.2018.23.Sup3.S16
Whayman N. Doppler assessment: getting it right. Wound Essentials. 2014; 9:(2)48-52
Willenberg T, Schumacher A, Amann-Vesti B Impact of obesity on venous hemodynamics of the lower limbs. J Vasc Surg.. 2010; 52:(3)664-668 https://doi.org/10.1016/j.jvs.2010.04.023
Chronic venous disease is a common problem that is often overlooked by healthcare practitioners. It is estimated to affect as much as 30% of the adult population although this is difficult to calculate due to a significant rate of under-diagnosis (Radak et al, 2016). Cost estimates for management of venous disease have varied from €600-900 million to as much as €2.5 billion a year across Western Europe. These costs include investigations, treatment and management, deterioration of quality of life and loss of working days (Rabe and Pannier, 2010). The main risk factors of chronic venous insufficiency (CVI) increase with age and obesity. It is therefore recognised that the prevalence is slowly rising, increasing the socioeconomic burden (Rabe and Pannier, 2010).
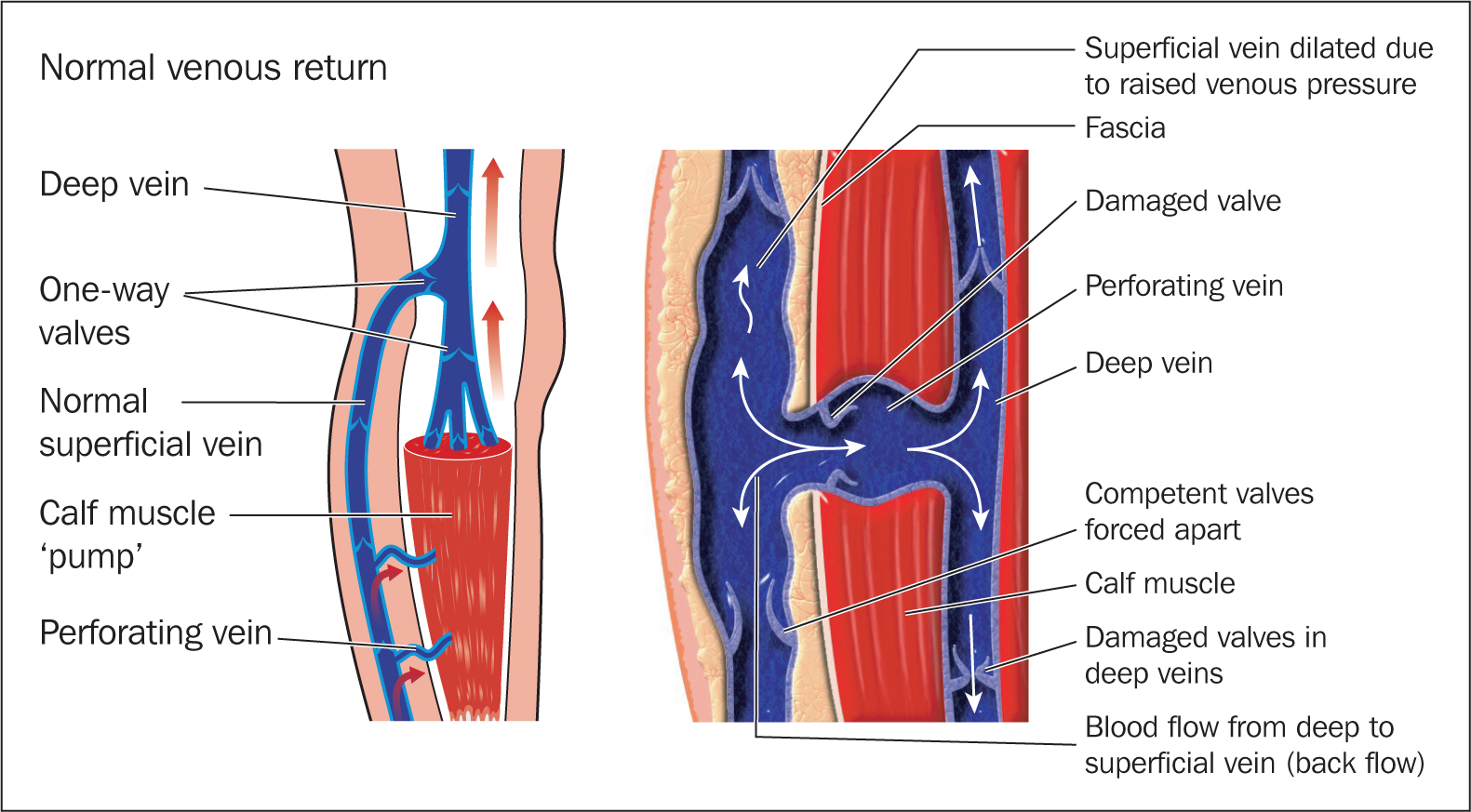
Venous blood flows from the skin to the superficial veins (found in the subcutaneous tissue), which drain into the deep veins. Bicuspid valves in the veins function to keep blood moving in one direction and prevent backflow of blood. Venous insufficiency is an impaired flow of blood through the veins caused by valve incompetence (where the valves are unable to close completely) (Woods, 2019). Blood leaks back through the valve and pools in the superficial veins increasing pressure, which can further weaken the valves and cause irreparable damage. Figure 1 shows the effect of an incompetent valve in the leg.
Figure 1. Incompetent valve in the leg causing venous insufficiency
Risk factors
Venous insufficiency includes a broad spectrum of venous complaints which range from telangiectasias or ‘spider veins’ (named for their spider web appearance) and varicose veins, to chronic venous ulcers and deep vein thrombosis (DVT) (Ballard and Bergan, 2000). The majority of the research indicates that women are more likely than men to have varicose veins (Ballard and Bergan, 2000). The risk factors for venous insufficiency include increasing age, in both men and women, genetics, occupation (prolonged standing or heavy lifting), pregnancy, and diet; some evidence suggests that a western diet of reduced fibre and refined foods leads to constipation and intra-abdominal pressure from straining is transmitted to the veins in the legs (Ballard and Bergan, 2000). Other risk factors are obesity, smoking, reduced mobility and haematological factors (Woods, 2019). Increased venous pressure over time leads to a chronic inflammatory response, which can cause the breakdown of tissue resulting in venous leg ulceration (Wounds UK, 2016).
Assessment
Early assessment, diagnosis and intervention is essential to reduce the burden of CVI and improve quality of life. The CEAP (Clinical-Etiological-Anatomical-Pathophysiological) classification tool is a standardised method used in the management of CVI (Eklöf et al, 2004) (Table 1). Originally established as a tool to assess for recurrent varicose veins, it identifies early signs of venous disease. The tool was modified in 2004 to include chronic venous disorders. CEAP is a descriptive classification and can be used in conjunction with other venous severity scoring tools.
Confirm the patient's specific requirements and reason for assessment
Ask the patient if they have had any pain. This could be due to venous wall hypoxia, venous hypertension, venous wall tension, leucocyte adhesion in subvalvular areas or areas of inflammation (Clarke et al, 1992), heaviness, which is due to increased capillary pressure and can result in oedema (Clarke et al, 1992), aching caused by oedema, night-time cramps and restless legs, swelling and itching of the lower limb. Symptoms may be typically worse at the end of the day and relieved by elevation (National Institute for Health and Care Excellence (NICE), 2019)
Consider risk factors such as immobility or a history of DVT
Assess for any comorbidities. Common comorbidities encountered with venous disease are: diabetes mellitus, arterial hypertension, peripheral arterial disease, heart failure, skeletal or joint leg diseases, renal insufficiency, emphysema or chronic obstructive pulmonary disease, inflammatory bowel disease and malignant disease (Matic et al, 2015). Additional screening for these comorbidities in patients presenting with symptoms of venous disease is recommended (Matic et al, 2015)
Ask the patient what current medication they are taking to complete a full medical history
Consider whether the person has any symptoms and if they affect overall quality of life and general health (NICE, 2019)
Ask the patient if they have any allergies such as to latex and lanolin—this may have an influence on choice of treatment.
Ankle–brachial pressure index
Following full visual assessment nurses should consider a level one assessment of the venous system with a handheld continuous-wave Doppler for an ankle-brachial pressure index (ABPI) assessment (Ballard and Bergan, 2000). The ABPI assessment is not intended for diagnosis of venous disease but rather excludes significant arterial disease by comparing systolic blood pressure between the arm and ankle (Wounds UK, 2019).
This procedure must be carried out by a competent clinician who understands and is able to interpret results to confirm safe practice. A list of contraindications to Doppler assessment is shown in Box 1.
Contraindications to Doppler assessment
Deep vein thrombosis (DVT)
Cellulitis (depending on severity and pain)
Surgery to arm or leg
Lymph node clearance
Cancer-related treatments
Amputation
Friable skin
Mental health-related issues
Dementia
Neurological disease (eg that may affect the patient's ability to sit still)
The ABPI ratio is usually above 1. A value below 0.92 is considered abnormal and an indication of peripheral arterial disease (Vowden and Vowden, 2018). Early intervention with class I or class II compression garments when C1 or C2 venous disease has been confirmed significantly reduces further complications associated with venous disease. Patients who are managed with compression should have regular vascular assessments to ensure their arterial status has not worsened (Wounds UK, 2016). Patients with a ABPI of less than 0.5 are not suitable for compression and should be referred to a vascular surgeon. Patients with an ABPI of 0.5–0.8 may be suitable for reduced compression but this must only be applied by competent nurses who have received the correct education and training.
Before carrying out an assessment it is essential to correctly assemble all the necessary equipment.
Equipment required
Handheld Doppler
Multiple size blood pressure cuffs (to accommodate different limb sizes)
Manual sphygmomanometer
Doppler gel
Clean film (to cover leg ulcers/wounds if present)
Gloves and apron
Documentation.
Procedure for ABPI assessment
Confirm the patient's identity, explain and discuss the full procedure and obtain consent
Wash hands and put on apron and gloves
Help the patient to lie down. To record the best resting ABPI the patient should be asked to remain as still as possible for 30 minutes. This is a crucial part of the assessment and should not be rushed (Moffatt et al, 2007; Whayman, 2014)
Ensure the patient is lying as flat as possible to reduce hydrostatic pressure inaccuracies, which can lead to falsely high ABPI readings. If the patient is unable to lie flat, try to bring their legs as close to heart level as possible. Document the position of the patient to ensure consistency for future readings
Observe the lower limb for any previous leg ulcer scars and ask the patient about their venous history. Check whether the patient has had any surgery for varicose veins involving ligation (tying off) and stripping (removal), or endothermal ablation (energy from high-frequency waves or lasers to seal the affected veins) (NICE, 2013)
Observe the lower limb for signs of telangiectasias (spider veins)—these are commonly found on the back of the leg. Spider veins are small superficial veins or arterioles. Spider veins measure less than 1.0 mm in diameter and occur mainly in the lower extremities. Reticular veins are located in the subcutaneous tissue, they measure less than 3 mm in diameter and are often tortuous (twisted) and widened (Nakano et al, 2017)
Check for visible, palpable varicose veins larger than 3 mm. These are the most significant indicator of venous insufficiency. It is important to explain to patients that once chronic venous disease begins, the delivery of nutrients and oxygen to the skin is being compromised and complications can easily develop
Assess lower limb for swelling, oedema and lymphorrhea (lymphatic leak). Pitting oedema is the result of applied pressure over oedematous subcutaneous tissue. This results in a depressed area caused by displaced interstitial fluid and typically worsens throughout the day (Brodovicz et al, 2009). This can be assessed by firmly pressing your thumb onto the skin for at least 2 seconds on each limb
Observe the limb for any skin changes:
Lipodermatosclerosis: defined as areas of painful, tight skin with hardened subcutaneous tissue just above the ankle (NICE, 2019). This is due to infiltration of fibrin and inflammation and results in an altered limb shape resembling an inverted champagne bottle
Hyperpigmentation: identified by a reddish-brown discolouration of the skin due to the deposition of haemosiderin
Varicose eczema: itchy, red, flaky and scaly skin, which may blister with surface crusts (NICE, 2019)
Atrophie blanche: white, star-shaped scarred areas with surrounding pigmentation (NICE, 2019)
Examine the foot, locating the dorsalis pedis, anterior tibial, peroneal and posterior tibial pulses. Palpate foot pulses. Reduced or absent pulses may indicate peripheral arterial disease (Londero et al, 2016). It is important to note that 10% of the population have an absent dorsalis pedis (Figure 2)
Measure brachial systolic blood pressure in both arms (unless contraindicated). This is the fundamental principle underpinning ABPI calculation and supports identification and management of a number of medical conditions (Vowden and Vowden, 2018)
Place an appropriately sized cuff around the upper arm. It is essential to use the appropriate cuff size for the patient. A cuff that is too small can result in an overestimation of pressure, a cuff that is too big can lead to an underestimation of pressure (Vowden and Vowden, 2018). Try to avoid repeatedly inflating the cuff before it has fully deflated as this can alter pressures (Whayman, 2014)
Locate the brachial pulse and apply ultrasound gel
Hold the Doppler probe at 45 degrees to the arm in the direction of the heart. Move the probe around until a pulse is located. If a continual ‘whoosh’ sound is heard, this is a vein and should not be used to calculate the ABPI (Whayman, 2014)
Slowly inflate the cuff until the signal is no longer heard. Slowly deflate the cuff and record the pressure when the signal returns. Avoid rapidly deflating the cuff. This may result in the highest pressure being missed (Vowden and Vowden, 2018)
Repeat this procedure on the other arm
Place an appropriately sized cuff around the ankle just above the malleoli. If required and for infection control purposes, cover leg ulcers or other wounds with clean film before the application of the blood pressure cuff
Apply ultrasound gel to the foot pulses and continue as for brachial pressure, recording in the same way. A minimum of two pulses should be used for each leg to calculate an ABPI. The anterior tibial and dorsalis pedis should not both be used in the same assessment as they form part of the same artery
Listen to the Doppler sounds to assess the level of arterial disease. A triphasic sound, where three beats are heard, is the sound of a healthy artery. Biphasic sound is where two beats are heard, often in older patients who have altered physiology due to the normal ageing process. Monophasic or a single beat heard indicates that the vessel is diseased. It is important that nurses have good knowledge of the anatomy of the four foot pulses and arterial sounds to comprehend the state of the vessel (Whayman, 2014)
Repeat for the other leg
To calculate an ABPI the highest reading on the right foot should be divided by the highest systolic brachial. This should be repeated with the left foot, taking the highest reading on the left foot and dividing by the highest systolic brachial reading. This gives ABPI for the arterial vessels in both legs (Staines, 2018) (Box 2).
Refer to local policy for interpretation of the ABPI values (NICE, 2019)
Document the assessment in the patients' records
Give the patient lifestyle advice to relieve symptoms of CVI and reduce risk factors. This should include advice around weight (obesity predisposes individuals to venous stasis—slow blood flow in the veins—which can trigger DVT and CVI) (Willenberg et al, 2010). They should be advised to engage in moderate physical activity including calf muscle pump exercises (Padberg et al, 2004; NICE, 2013) and avoid activities that require sitting or standing for prolonged periods of time (NICE, 2013). Advise the patient to elevate legs when sitting to improve blood flow back to the heart. If compression is indicated, establish safe practice.
Automated devices can simplify and speed up accurate recording of ABPI and facilitate early detection of peripheral arterial disease compared with the traditional Doppler testing. These machines can be used as second-line assessment if the patient requires extensive assessment or for reassessment (Wounds UK, 2019).
Figure 2. Location of the pedal pulses
Calculating ABPI
ABPI (Right) = P(R)/P(B)
ABPI (Left) = P(L)/P(B)
P(R) = Highest systolic pressure obtained from the vessels in the right ankle
P(L) = Highest systolic pressure obtained from the vessels in the left ankle
In summary, the most common cause of CVI is venous reflux. Early assessment, diagnosis and intervention can reduce complications of CVI and prevent further deterioration, which can lead to leg ulceration. Nurses should be competent in recognising early signs of venous disease and provide patients with information to relieve symptoms and reduce risk factors. ABPI assessment is used to ensure safe practising of compression, or it can confirm peripheral arterial disease, which can trigger appropriate referrals and treatment.
LEARNING OUTCOMES
Be familiar with clinical guidance on early indications for chronic venous insufficiency
Increase knowledge of lower limb assessment
Improve awareness of the complications of chronic venous insufficiency in the lower limb