

This article reports on the successful management of a patient in her 40s who had been diagnosed with Klippel–Trenaunay syndrome at birth and was experiencing lower left extremity lymphoedema, lymphorrhoea, and cellulitis.
Klippel–Trenaunay syndrome is a congenital condition. The symptoms associated with the syndrome are port wine stains, varicose veins and hypertrophy (extra growth) of one limb. The port wine stain is usually visible at birth but the diagnosis may not be confirmed until the varicose veins and limb hypertrophy become more noticeable later (Great Ormond Street Hospital for Children NHS Foundation Trust, 2015).
Despite having a lymphoedema diagnosis in childhood and treatment using low-strength compression therapy, the patient had experienced worsening lymphorrhoea and epidermolysis in one limb after giving birth. Subsequently, she was referred to the lymphoedema outpatient clinic at an acute hospital. The patient had concerns regarding the extensive lymphorrhoea and epidermolysis, which affected her daily life, requiring frequent changes of clothes during the day. She also experienced anxiety associated with the sudden occurrence of cellulitis, which she had experienced before. She had a newborn baby and therefore wanted these clinical concerns related to lymphorrhoea to be resolved.
Presentation and assessment
The patient presented at the lymphoedema outpatient clinic. On initial examination, moderately severe lymphoedema was noted – Stage II according to the International Society of Lymphology consensus document (Executive Committee of the International Society of Lymphology, 2020). There was also lymphorrhoea in the second toe of the left foot, and epidermal detachment in all toes on the left foot were observed. Indocyanine green lymphography (PDE NEO, Hamamatsu Photonics, Japan) was carried out to assess the functioning of the patient's lymphatic system. The left dorsal foot and ankle areas exhibited dermal backflow (Figure 1). A large amount of lymphorrhoea was observed on the second toe, leading to immediate recurrence after cleaning with gauze, as shown in the patient's self-recorded video images (Figure 2). The lymphorrhoea caused skin maceration and epidermolysis, such as skin pilling, which was observed on the second toe.


The probable cause of skin maceration and epidermolysis of the toes was the patient's use of a rubber thimble, a protective covering made of durable rubber or latex designed to be worn on the fingertip to prevent friction or needle pricks when sewing or performing other tasks to provide fingertip protection. In this case, the patient had used a rubber thimble over her second toe to avoid wetting her clothes and shoes with the lymphorrhoea. Furthermore, the patient had stopped wearing elastic hosiery for several months as the stockings became wet owing to lymphorrhoea. The mismanagement of lymphorrhoea and the discontinuation of compression therapy had led to wounds such as epidermolysis and an increased risk of developing cellulitis (Figure 2a; b; c).
Treatment
Generally, plastic surgeons and certified lymphoedema therapists (CLTs) provide treatment and care for patients with lymphoedema at the outpatient clinic; however, the team proposed that a professional with knowledge and technical expertise in skin conditions, as well as daily skin-care routines, would contribute to the better management of this patient's condition. Therefore, the team's CLT consulted a wound, ostomy and continence care specialist nurse (WOCN), who provided skin-care advice.
To minimise the lymphorrhoea's adherence to the skin during the day, a Moiskin Pad (White Cross, Japan) was used. This protective pad protects the skin and features a highly absorbent layer of gauze to absorb liquid, gently protecting the wounds and preventing skin maceration. The pad was cut to the size of the toe and wrapped around the second toe. Subsequently, its placement was secured using YU-KIBAN Surgical Tape (Nitto Denko Corporation, Japan), which peels off almost no stratum corneum when removed, preventing skin damage when changing dressings.
These methods helped to reduce the frequency with which the patient had to change her clothes. The CLT recommended elastic hosiery with 30 mmHg compression to control oedema and selected a toe-less pantyhose-type to avoid wetting the elastic hosiery with lymphorrhoea. Although compression over the toe area might have been beneficial, the team decided that the choice of toe-less stockings would reduce skin problems caused by a moist environment and skin maceration due to lymphorroea, as well as the psychological burden of discomfort and the need to change clothing frequently. Following the procedure, the CLT provided self-care instructions to the patient regarding skin-care maintenance and elastic stocking use. After a month of conservative therapy, the epidermolysis had healed (Figure 2d). This comprehensive treatment strategy by the WOCN and CLT was developed to help the patient be cellulitis-free prior to lymphaticovenular anastomosis (LVA).
LVA was performed by a plastic surgeon, involving the anastomosis of two lymphatic and venous vessels on the left dorsal foot and left lower leg (Figure 3a). It is a procedure to improve lymphatic circulation by redirecting excess lymphatic fluid into the venous system to reduce the appearance of lymphoedema and prevent it recurring. Follow-up evaluation at 1-year post-LVA revealed complete resolution of lymphorrhoea (Figure 3b).
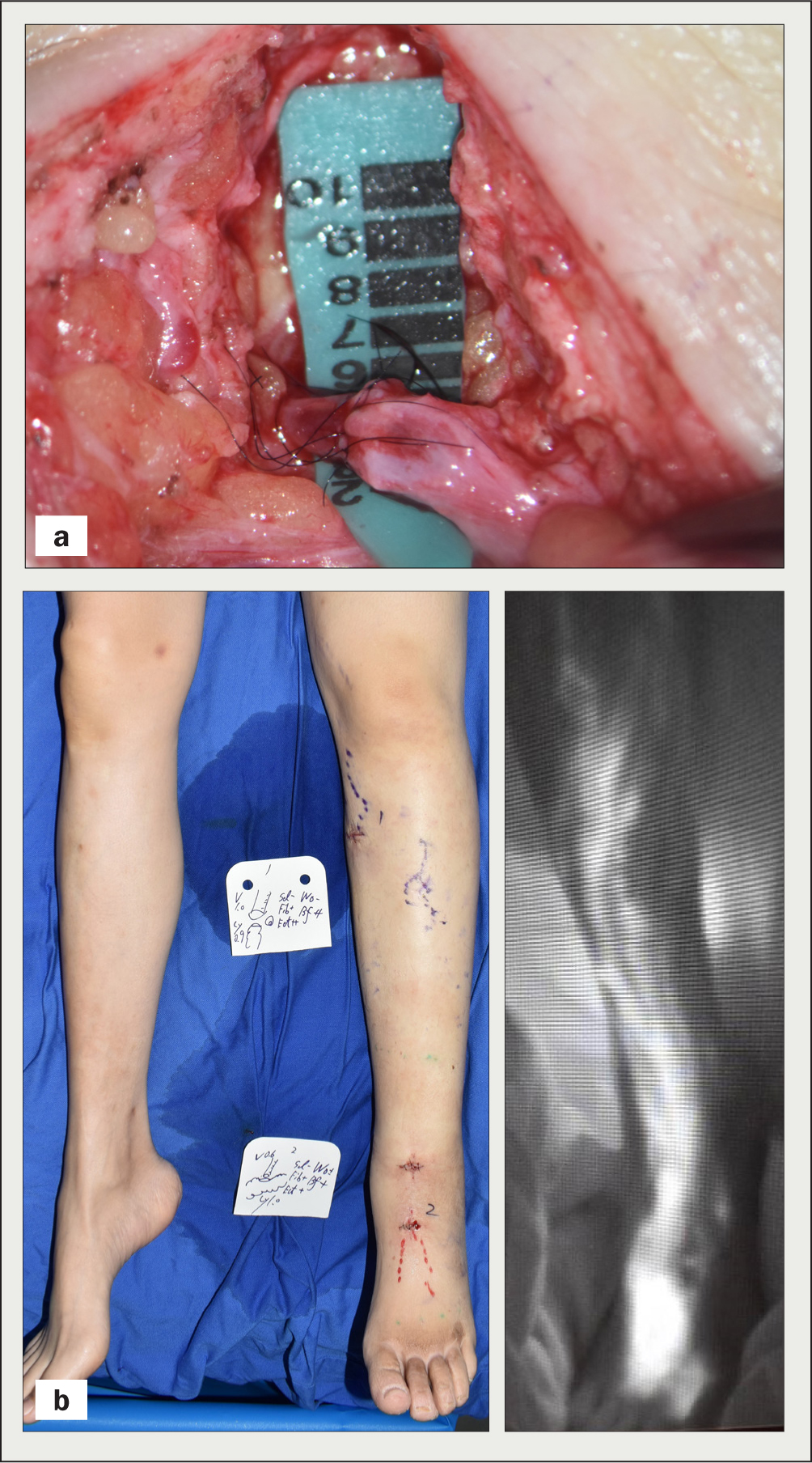
No further episodes of cellulitis occurred, and the patient reported significant improvement in limb circumference (Figure 4).

The combination of an LVA performed by a plastic surgeon to improve lymphatic circulation, skin care recommendations by a WOCN, and compression therapy by a lymphoedema therapist achieved this positive result.
Discussion
This case study highlights the effectiveness of a multidisciplinary approach to lymphoedema management, resulting in the complete resolution of the patient's lymphorrhoea at 1-year follow-up.
These findings are consistent with those of previous studies demonstrating the effectiveness of LVA in reducing lymphorrhoea and improving the skin's condition in patients with lymphoedema (Soo et al, 2008; Mihara et al, 2014). In addition, the team focused on the persistent lymphorrhoea and epidermolysis that were successfully treated through a combination of skin care and compression therapy based on the needs of the patient's daily life, and the LVA surgery. These conditions pose a risk of cellulitis, impairment of daily activities, and discomfort owing to clothing becoming wet.
The team recognised the necessity of providing skin care recommendations by skin-care professionals. Specifically, the patient demonstrated insufficient understanding of lymphorrhoea control, as evidenced by her use of a rubber thimble, which caused epidermolysis. Thus, self-care education tailored to her daily life was deemed essential in addition to compression therapy (Miller, 2017; Manduz et al, 2018; Sudduth and Greene, 2022) with LVA (Douglass et al, 2016; Executive Committee of the International Society of Lymphology, 2020; Vignes et al, 2021; Kitamura et al, 2022). Through collaboration between health professionals, the patient gained a thorough understanding of proper skin care methods, used elastic stockings customised to address the extent of lymphorrhoea and lymphoedema in the toes, and experienced improvement in epidermolysis, as well as a reduction in the limitations on her daily life. With the resolution of lymphorrhoea through LVA, successful management of lymphoedema was achieved by maintaining appropriate self-care practices.
Limitations
The main limitation of this case report is the potential variation in the cost of multidisciplinary collaboration and LVA operations owing to differences in healthcare insurance and reimbursement systems between countries, emphasising the need to consider this report as a single-facility case study from an acute care hospital in Japan. Therefore, further research should be conducted to examine how professionals can collaborate for lymphoedema management, considering the specific regulations and healthcare provisions in each country.
Conclusions
A combination of specific skin care instructions, adequate compression therapy, and LVA by a multidisciplinary team was effective in the management of lower extremity lymphoedema with lymphorrhoea and epidermolysis. This approach resulted in the resolution of lymphorrhoea and epidermolysis, with no recurrence observed at the 1-year follow-up. This case study highlights the importance of a multidisciplinary approach to lymphoedema management and the potential benefits of combining different treatment modalities for optimal outcomes. Further studies with diverse cases are required to confirm and integrate these results into regular practice.
KEY POINTS
- Lymphoedema with lymphorrhoea can negatively affect patients' quality of life
- Inappropriate self-care routines and discontinuation of compression therapy can increase the risk of cellulitis development
- Patients should be provided with recommendations regarding skin care and compression therapy to facilitate treatment adherence and efficacy
- A combination of lymphaticovenular anastomosis, compression therapy, and skin-care instructions provided by a multidisciplinary team, may be effective for the management of patients with lymphoedema caused by Klippel–Trenaunay syndrome with lymphorrhoea and epidermolysis
CPD reflective questions
- How can one increase adherence to compression therapy for lymphorrhoea owing to the impact of therapy on a patient's quality of life?
- What skin care routines should be recommended to facilitate the efficacy of concomitant treatments?
- When should a multidisciplinary approach be recommended for lymphoedema patients?