

Haemodialysis is the best known of the kidney-replacement therapies used to treat people with both end-stage kidney disease (ESKD), the final stage of chronic kidney disease (CKD) and acute kidney injury (AKI). Kidney-replacement therapies are not a cure for kidney disease, rather they palliate its effects (Mahon et al, 2013).
There are about 4 million people worldwide being treated with a kidney-replacement therapy for ESKD, of whom 69% are on haemodialysis (Bello et al, 2022). In the UK at the end of 2020 68 249 individuals with ESKD were being treated with a kidney-replacement therapy, 35.4% of whom were receiving in-centre haemodialysis and 2% home haemodialysis (UK Renal Registry, 2022); the rest either had a kidney transplant or were maintained on peritoneal dialysis.
While transplant is by far the most prevalent kidney-replacement therapy modality in the UK, with 57% of affected individuals (UK Renal Registry, 2022), haemodialysis is the most common initial therapy. However, haemodialysis is the kidney-replacement therapy that is widely accepted as being the greatest burden both for the patient (Jones et al, 2018) and financially for the NHS, each year costing between £23 403 for home haemodialysis (HHD) and £32 678 for treatment in hospital for patients requiring transport (Roberts et al, 2022).
The choice of kidney-replacement therapy for ESKD relies on a clinical assessment and discussion with the patient. Choices are informed by the patient's age, dexterity, the presence of comorbid disease and personal preference (National Institute for Health and Care Excellence, 2018).
This article introduces the reader to haemodialysis, discussing the science and basic clinical practice that underpin it. It primarily discusses haemodialysis as a chronic modality used to treat people with ESKD, other than where indicated.
Where is haemodialysis undertaken?
Haemodialysis is usually performed in one of four places:
- On a hospital ward/inpatient unit
- In a hospital-based dialysis unit
- In a satellite dialysis unit
- In the patient's home.
Where the haemodialysis is performed is a function of the need of the patient at that point in time. For example, a patient with AKI may be dialysed in the intensive care unit because they are being treated for other disease (Ellis, 2013), whereas a dexterous patient with ESKD might dialyse at home (Ellis, 2022).
Although haemodialysis is a technical undertaking, modern machines and dialysis technology have made it easier to undertake than used to be the case. This means opportunities for HHD are increasing, especially because it can be undertaken as frequently as necessary, even daily, and at a time to suit the patient's lifestyle.
What is haemodialysis?
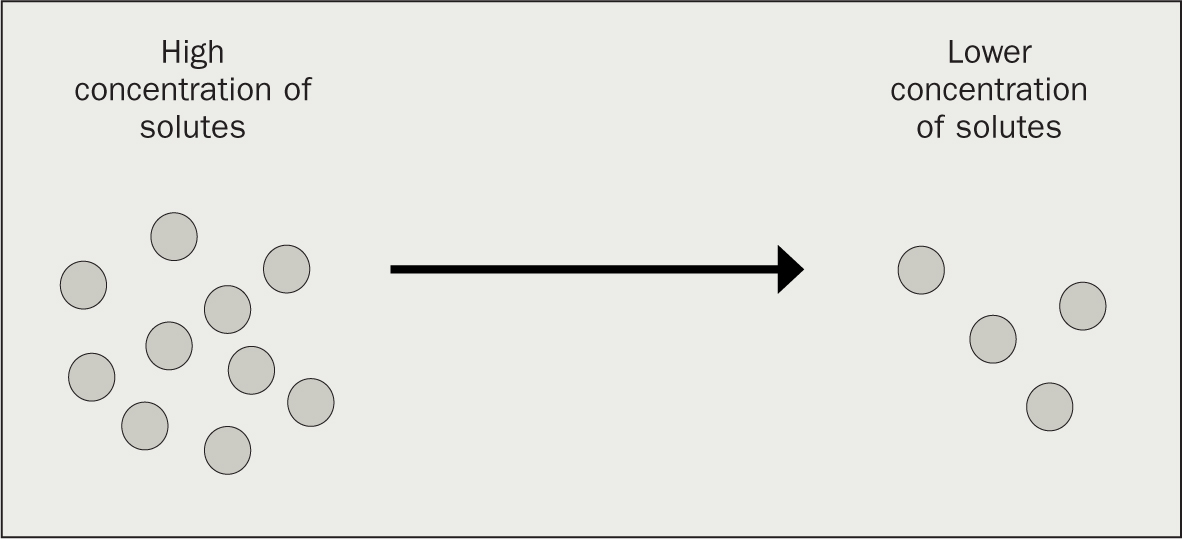
Haemodialysis is the term used to describe a process in which blood is filtered across a semipermeable membrane, in a dialyser, causing toxins and excess fluid to be removed. Haemodialysis uses mechanical means to exploit two basic principles of biology and physics, namely diffusion and ultrafiltration, although the process of dialysis is in essence a form of diffusion (Ellis, 2010) (Figure 1 and Figure 2).
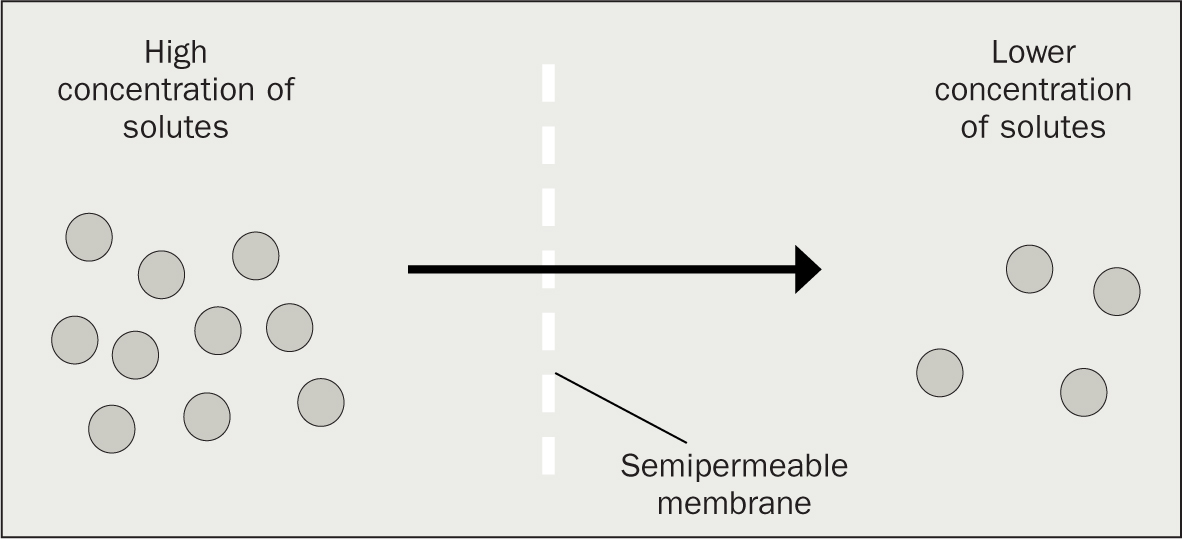
A semipermeable membrane is one that is permeable to some solutes, the size of which are regulated by the size of the pores in the membrane. The membrane is impermeable to other substances that are not in solution, such as erythrocytes, plasma proteins (such as albumin) and platelets (Ellis, 2010).
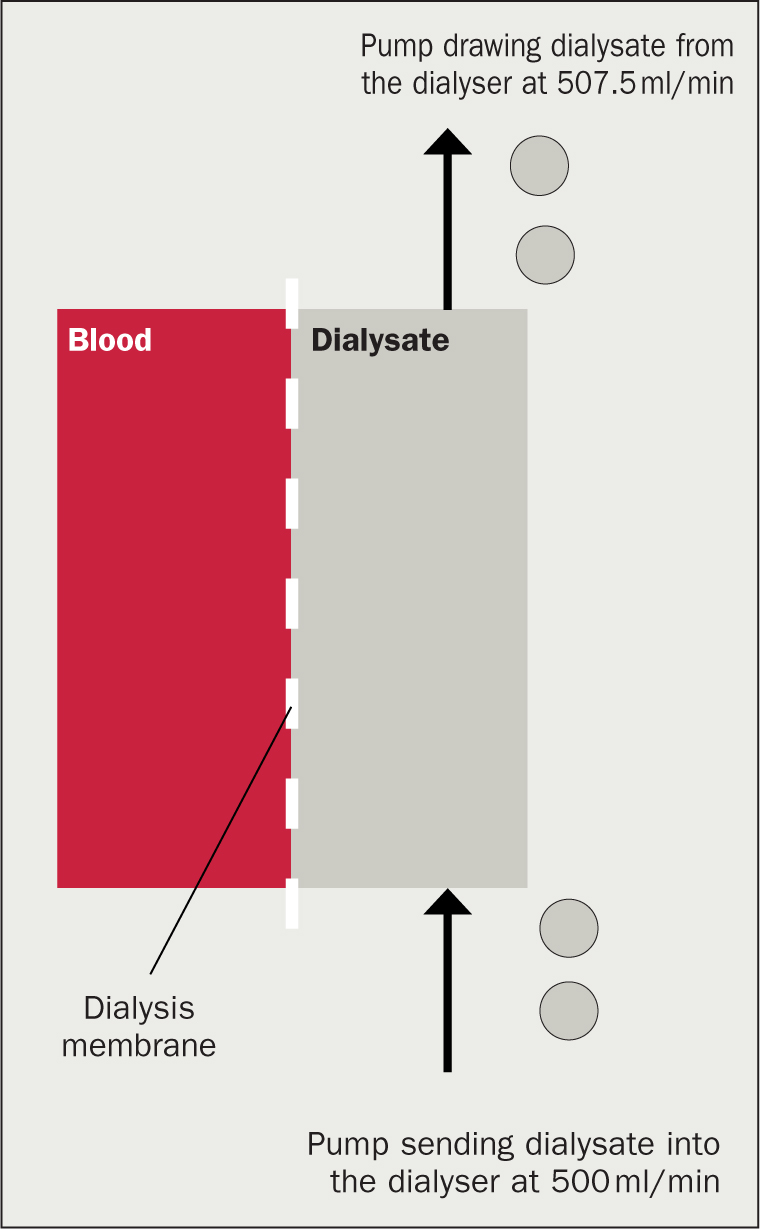
Ultrafiltration (Figure 3) is the process that removes water from the plasma of the patient across the semipermeable membrane using mechanically derived pressure (Sam, 2014). During dialysis, the dialysis machine is programmed to remove a certain amount of water from the patient's blood, which it does by creating a pressure across the dialysis membrane, with the pressure on the blood side of the membrane being higher than on the dialysate side. This effectively sucks water across the membrane to equalise the pressures (Goode et al, 2020); it also drags some solutes with it through a process called convection (Ellis, 2010).
Water removal is necessary because patients who undertake haemodialysis rarely pass urine. The amount of fluid to be removed is calculated from the difference between the weight of the patient when they attend dialysis and their ideal bodyweight, that is, what they are estimated to weigh when the excess fluid has been removed (Mahon et al, 2013). Modern dialysis machines are what is termed volumetric, that is, they control how much water is removed according to what the operator keys in at the start of the haemodialysis session.
The haemodialysis process
During haemodialysis, the patient's blood passes down one side of the dialysis membrane and the dialysate, dialysis fluid, passes down the other creating the opportunity for diffusion across the membrane, dialysis, to occur (Ellis, 2010). In dialysers, the artificial kidney, the blood passes through straw-like fibres while the dialysate passes around the outside, so under normal conditions the two never mix.
Diffusion, dialysis, happens both ways across the dialysis membrane, with toxins moving from the blood to the dialysate for disposal, while other electrolytes, eg bicarbonate, pass the other way. This occurs because of the diffusion gradient created by:
- The respective levels of solutes in the blood and dialysate
- The counter current in the dialyser (see below).
Dialysate is composed mainly of highly purified water. This water goes through a series of stages of pre-treatment, filtration, softening and purification, the last of which is reverse osmosis, which is a process that uses energy to drive osmosis in the opposite direction to normal (Kasparek and Rodriguez, 2015) (Box 1).
Box 1.Osmosis and reverse osmosis
| Osmosis | The movement of water from an area of high water concentration (low amounts of solutes) to an area of low water concentration across a semi-permeable membrane |
| Reverse osmosis | The movement of water from an area of low water concentration (modest amounts of solutes) to an area of high water concentration across a semipermeable membrane |
The highly purified water is then mixed in the dialysis machine with an electrolyte solution that invariably includes:
- Sodium
- Chloride
- Potassium
- Calcium
- Phosphate
- Magnesium
- Glucose.
The solution will include other physiologically important electrolytes. If the dialysate did not contain these electrolytes, the levels in the patient's blood would become dangerously low, leading to issues such as cardiac arrhythmias and death (Mahon et al, 2013).
This electrolyte solution is acidic: were it not acidic, the electrolytes would crystallise. This creates an issue because patients with ESKD are invariably acidotic because of their inability to metabolise or excrete hydrogen ions. This is overcome by the addition at the point of dialysis of bicarbonate, as a buffer, to the dialysate (Ashby et al, 2019). Given the elevated level of bicarbonate in the dialysate and the low levels in the patient's blood, bicarbonate naturally diffuses across the dialysis membrane and, in so doing, reverses the patient's acidosis even if only temporarily (Box 2).
Box 2.Components of dialysateDialysate contains:
- Physiological levels of electrolytes that need maintaining at physiological levels (eg sodium, chloride etc)
- Subphysiological levels of electrolytes that accumulate in CKD and need to be reduced but not entirely removed (eg potassium, calcium etc)
- Super-physiological levels of solutes that need to be increased in the blood (ie bicarbonate)
- None of the waste products dialysis seeks to remove (ie creatinine/urea)
Dialysis therefore not only removes uraemic toxins, but is also used to balance other bodily electrolytes, either by reducing their levels, limiting their removal or introducing them to the patient's blood (Ellis, 2010).
The counter-current, mentioned earlier as one of the ways in which the diffusion gradient is maintained, is important. Quite simply, while the blood of the patient usually runs down the dialyser, the dialysate runs up it (Nalesso and Garzotto, 2020). At the top of the dialyser, the blood contains its highest levels of uraemic toxins and at the bottom its lowest, while in the case of the dialysate the reverse is true – this means that the dialysis gradient, the difference between the concentrations of toxins in the blood and dialysate, is maintained throughout the dialyser.
Dialysis access and the blood circuit
To achieve a good level of dialysis, it is necessary for the patient's blood to pass through the dialyser several times. This means a good flow of blood needs to be attained. To move blood around the dialysis circuit, dialysis machines use a type of pump that provides a peristaltic-like action, which is less damaging to blood cells than other pump types. Most patients require some anticoagulation, often unfractionated heparin, to be administered into the dialysis circuit after the pump to ensure the circuit remains patent (Ashby et al, 2019).
A good flow rate cannot be achieved by the usual methods of accessing the circulation such as a simple venous catheter or simple central line. There are two reasons they would not work: the first is that there is a need to get blood out from the patient at somewhere between 200 ml/min and 400 ml/min, which peripheral veins and narrow lumen catheters will not support. The second is that the blood needs to be returned at a similar rate to that at which it is removed and, again, peripheral veins and narrow and single lumen catheters will not allow for this.
Vascular access for haemodialysis therefore needs to be established not only to allow for haemodialysis, but also in the case of patients with ESKD, to allow repeated access while minimising risk of infection (Mahon et al, 2013). Types of vascular access for haemodialysis include:
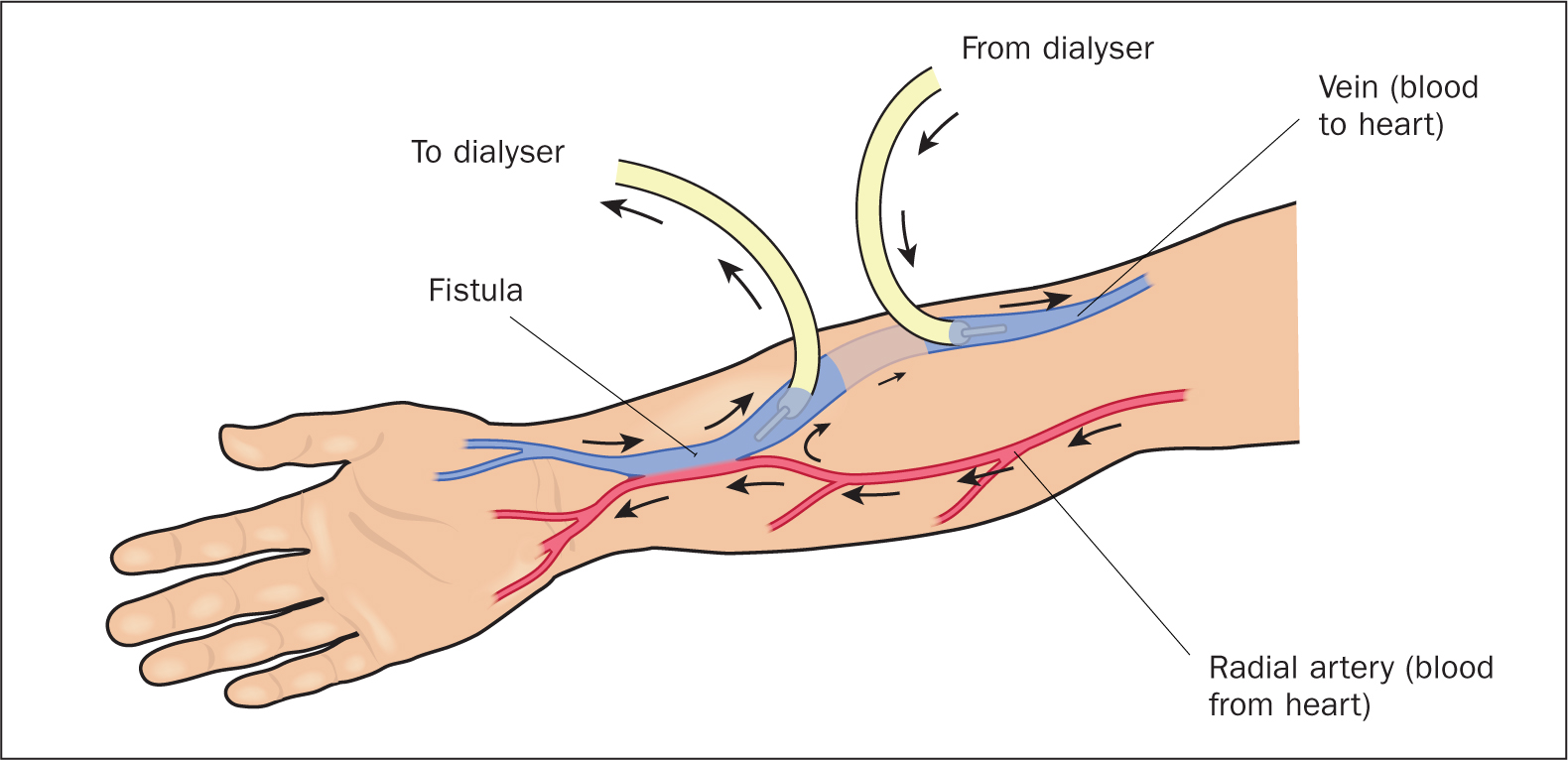
- Arteriovenous fistulae (AVF) (Figure 4)
- Arteriovenous grafts (AVG)
- Tunnelled vascular catheters (TVCs)
- Non-tunnelled vascular catheters (NTVCs).
As a rule, non-kidney care professionals should not touch haemodialysis vascular access because it is essential that they are handled correctly to avoid complications such as infections, clotting and access loss (Mahon et al, 2013).
An AVF is formed when an artery is joined, anastomosed, to a vein, eg the radial or brachial artery, and the cephalic vein or the brachial artery and basilic vein. Joining an artery and a vein creates a fistula, an unnatural opening between bodily structures. The arterial pressure from the blood causes the vein to dilate because, unlike the artery, it is not elastic. This swelling firms up over time and it is possible thereafter to insert large bore needles into the AVF, which are removed after the haemodialysis sessions.
The advantage of the AVF is that the blood flow rate through it is quite high, because it is arterial, and the AVF is entirely natural, ie there is no foreign material involved. When well treated, an AVF can be used for many years and carries a low infection risk.
An AVG is similar to an AVF, but is formed where either a synthetic graft, eg Dacron, or a natural graft, eg a bovine or autologous saphenous vein, is used to join an artery to a vein usually in older or diabetic patients with fragile veins. AVGs are accessed in a similar way to AVFs but carry a higher risk of infection, clotting and failure.
TVCs are usually inserted in individuals for whom an AVF or AVG is not suitable, isn't yet working or has already failed. A TVC is usually inserted into the internal jugular vein, the subclavian usually being avoided because it carries a high risk of clotting (Santoro et al, 2014). Rather than exiting the skin immediately, the TVC is tunnelled under the skin for a few centimetres and anchored with a Dacron cuff to reduce the risk of an exit-site infection tracking to the patient's blood (Gallieni et al, 2014). TVCs are considered to provide temporary, or semipermanent, access.
NTVCs offer temporary access and may be placed in the femoral artery (where they need to be removed after each haemodialysis session), or the internal jugular vein where they may remain for up to 2 weeks (Mahon et al, 2013).
Dialysis catheters have two lumens and are of a wide bore, so they can accommodate the flow rates needed for dialysis. They need specialist handling and should be flushed and locked, filled with an anticoagulant, such as citrate or heparin, to help maintain patency between haemodialysis sessions (Renaud et al, 2015).
The biggest risk for any vascular catheter is infection, which means that a patient, even with a TVC, has two or three times the risk of hospitalisation and death from infection than a patient with an AVF or AVG (Miller et al, 2016).
Ensuring the dialysis dose
Dialysis adequacy, as it is termed, can be measured in a number of ways but is, in essence, a derivative of the time the person spends on dialysis (how many hours and how many times a week), the size of the dialyser used (its internal surface area), and the speed of the blood flow around the circuit as matched up to the speed of the flow of dialysate (Ellis, 2012).
The dose of dialysis that an individual needs is itself a function of the person's size or, more importantly, muscle mass, dietary intake and any residual kidney function the person may have (Ashby et al, 2019). A failure to provide adequate dialysis may impact patient survival (Liu et al, 2022).
Current guidelines support dialysis for most people undertaken thrice a week for a total of 12 hours, with high flux dialysers used for patients with little residual kidney function (Ashby et al, 2019). High flux dialysers not only clear more waste product during dialysis, they also clear other harmful substances not cleared by conventional dialysers, eg β2 microglobulin (Haroon and Davenport, 2018).
Complications
There are a number of long- and short-term complications associated with haemodialysis, which include (Habas et al, 2021):
- Infections
- Hypotension during haemodialysis
- Hypertension
- Ischaemic heart disease/cardiovascular disease
- Fatigue
- Pruritis
- Cramps
- Insomnia
- Bone disease
- Sexual dysfunction
- Anxiety.
People maintained on chronic haemodialysis are often anaemic which, if not treated well, can give rise to significant morbidity and mortality (Karaboyas et al, 2020). Many studies suggest that the quality of life for people on chronic haemodialysis is significantly worse than that of the general population (Al-Nashri and Almutary, 2022), although patients undertaking HHD may fare slightly better (Bonenkamp et al, 2020).
Options for treatment and alternatives
Patients have a choice as to where haemodialysis can be undertaken. In addition, patients with ESKD can be managed using other kidney-replacement therapies, including peritoneal dialysis or kidney transplantation.
There is increasing interest in haemo-diafiltration (HDF) for managing ESKD. HDF has an advantage over conventional haemodialysis because it utilises convective clearance of uraemic toxins, as well as much larger and ‘middle molecules’, which are associated with oxidative stress and may be responsible for at least some of the high levels of cardiovascular disease and mortality seen in haemodialysis patients (Blankestijn et al, 2020).
The future
At least some of the future for the management of CKD lies in early detection and treatment delaying, or preventing, the progression to ESKD (Shlipak et al, 2021). Much of what is needed in this context is joined-up thinking and management in primary care, where nurses are well placed to contribute to the management of conditions such as diabetes and hypertension which both cause and progress CKD (Ellis, 2021).
Future research into the management of ESKD includes the need to better understand the onset and management of symptoms for people commencing haemodialysis (de Rooij et al, 2022), as well as reducing the burden of cardiovascular disease in ESKD (Jankowski et al, 2021). For patients on dialysis, the big issues requiring further research include improving social rehabilitation, reducing the symptom burden and maximising their ability to function on a daily basis (Himmelfarb et al, 2020).
KEY POINTS
- Haemodialysis is one of a number of kidney-replacement therapies that may be used to treat people with end-stage kidney disease
- Haemodialysis exploits two basic principles of science, diffusion and ultrafiltration, to remove the waste products of metabolism and excess water from the patient's blood
- Diffusion across the semipermeable membrane also enables haemodialysis to be used to correct electrolyte imbalances and reverse acidosis
- Haemodialysis access is the patient's lifeline and should be handled only by staff who are trained to do so