

History taking and physical examination skills are an essential component of the advanced clinical practitioner (ACP) role and feature prominently within ACP-related educational and training frameworks and curricula. It is beyond the scope of this article to explore the complexity of the skills required for this essential component of the ACP role; however, there are a number of resources that have been developed specifically for the ACP and mapped to national curricula, including Peate et al (2023) and Diamond-Fox et al (2023a).
The overall aim of the respiratory-focused history and examination is to identify symptoms and physical manifestations that represent a final common pathway of a wide range of pathologies that may be highly suggestive or even pathognomonic of one pathology, or multiple concurrent pathologies.
Respiratory disease remains a prominent feature in both national and international statistics regarding the leading causes of death, more colloquially known as ‘the biggest killers’ (Office for National Statistics, 2023; World Health Organization, 2024). Bronchoconstriction, inflammation and loss of lung elasticity are some of the most common pathological processes that result in respiratory compromise, all of which are potential targets for manipulation with pharmacological and non-pharmacological therapies if diagnosed in a timely manner.
The clinical features of respiratory pathology may be varied and non-specific, in addition to affecting multiple anatomical sites and organ systems. Diagnosis of respiratory conditions may be incidental or secondary to investigation of other disease processes and can be challenging due to the potential coexistence of other pathologies, particularly those of the cardiovascular system. An appreciation of the common symptoms associated with respiratory conditions is essential as several conditions share common clinical symptoms and may go unrecognised as a result of focus on the management of single-organ dysfunction.
History taking
A skilled ACP has the potential to make a significant contribution to several fundamental outcomes: patient satisfaction, patient concordance with prescribed therapies/interventions, overall diagnostic accuracy and overall patient outcomes. Table 1 includes the most common presenting respiratory complaints. A comprehensive enquiry is required to facilitate diagnosis and treatment (Innes et al, 2018). Throughout this process the ACP will be alerted to what are termed ‘red flag’ symptoms. These symptoms may be immediately dangerous for the patient, whereas others may be a clinical indicator of a serious underlying pathology. Therefore, ‘red flags’ stand to warn us of a symptom associated with a life-threatening condition and must be acted upon accordingly (Ramanayake and Basnayake, 2018) (see Box 1).
| PC/PS | Presenting complaint/presenting symptom |
|---|---|
| Cough (+/- expectorant), dyspnoea, dysphonia, wheeze, stridor, stertor, haemoptysis, sputum production, chest pain, altered respiratory pattern, weight or appetite changes, pain (tracheal, mediastinal, chest wall, pleuritic), daytime somnolence, tremor | |
| HPC | History of presenting complaint |
|
|
|
| PH | Past history |
|
Previous respiratory and linked respiratory illnesses
|
|
| DH | Drug history |
|
|
|
| IH | Immunisation history |
| Influenza, COVID-19, pneumococcus, TB | |
| FH | Family history |
| Enquire about respiratory diseases in first-degree relatives. Predisposition is higher in asthma, hay fever, cystic fibrosis and lung cancer. Recessive inheritance is also found in alpha 1 antitrypsin deficiency | |
| SH | Social history |
|
|
Red flag clinical signs and their potential causes
| Clinical sign/observation | Potential pathology/cause |
|---|---|
| Stridor – high-pitched musical sound during inspiration | Upper airway obstruction due to tracheal stenosis, airway oedema, epiglottitis, foreign body, or anaphylaxis |
| Stertor | Pharyngeal obstruction |
| Cheyne-Stokes's respiration – alternating periods of fast, deep respiration followed by periods of apnoea | Metabolic acidosis, drug-induced respiratory failure and brain injury |
| Increased respiratory effort and use of accessory muscles | Hypoxia with underlying cause |
| Asymmetrical chest movement | Pneumothorax, pneumonia, pleural effusion |
| Tachypnoea and/or inability to speak a full sentence without becoming breathless | Hypoxia, hypercapnia, arrhythmia, exacerbation of existing pathology |
| Bradypnoea, breathing rate <8 breaths per minute | Opioid toxicity, metabolic alkalosis, carbon monoxide poisoning, brain stem injury |
| Biot's respiration – irregular pattern with periods of alternating apnoea and deep breaths | Brain injury, carries a poor prognosis |
| Reduced air entry | Pneumothorax, pneumonia, pleural effusion |
Following a comprehensive history taking it is advisable for clinical practitioners to undertake a review of all systems (Table 2). This gives the opportunity for ‘safety netting’ to eliminate any chance of missing an important disease or symptom. Conducting a review of all systems can also provide a clear focus for the physical examination (Shah, 2005). This may also guide the ACP as to whether more focused examinations of alternative body systems may be required when ruling out concurrent diseases.
| General questions | How are you feeling in general? |
|
| SOB | Is there any shortness of breath? |
|
| Is it coupled with a wheeze? | Consider bronchospasm | |
| Aggravating/relieving factors? |
|
|
| Exercise tolerance? |
|
|
| Cough | Is there any cough? | No – move on to Sputum |
| Acute/chronic? | Acute <3 weeks – infection, exacerbation of existing pathology, PE, bronchitis, sinusitis | |
| Chronic >3 weeks – COPD, asthma, bronchiectasis, lung cancer | ||
| Productive? | Producing phlegm leads to further questioning (see below – Sputum) a dry cough may be due to gastroreflux or use of certain antihypertensive drugs ie angiotensin-converting enzyme (ACE) inhibitor | |
| What time of day is it worse? |
|
|
| Sputum | Are you bringing up any sputum? | No – move on to Wheeze |
| What colour is it? |
|
|
| What is the consistency? |
|
|
| How much would you produce in a day? | Large mucopurulent volumes may indicate bronchiectasis, whereas large watery volumes may indicate pulmonary oedema (note, if persistent >3 weeks may indicate alveolar cell cancer). Sudden large amounts on a single occasion may indicate lung abscess or empyema | |
| Haemoptysis | Is there any blood in your sputum? |
|
| Wheeze | Do you have any wheeze/whistling when you breathe? | Asthma, COPD, airway obstruction (by foreign body or tumour), pulmonary oedema, allergens (ask about pets, pollen and environmental factors) |
| Aggravating/relieving factors? | Inhaler, positional change, environmental change | |
| Pain | Do you have any chest pain? | Characterise using formal tool ie SOCRATES, rule out life-threatening causes |
| What is the nature of the pain? |
|
|
| Sleep | Do you sleep well? | Ask about apnoea, snoring, nocturnal restlessness/dyspnoea, orthopnoea |
| Do you fall asleep during the day? | Can be an indication of obstructive sleep apnoea | |
| Do you or anyone you live with knows if you snore loudly? | Another indication of obstructive sleep apnoea, check Epworth score | |
| Tests | Have you had any recent investigations? | Chest X-ray, spirometry, lung function, CT scan, PET scan, MRI scan, bronchoscopy |
| How recent were they? | If not recent may need a repeat | |
| Tools | Can you grade/score your findings? | See tools discussed |
The traditional history-taking format meets many challenges in the time-critical situation, and the nature of these dynamic situations often means that a quick, focused history is required. The mnemonic ‘AMPLE’, originally developed for use in the context of trauma (Zemaitis et al, 2023), may be applied to quickly obtain pertinent information:
There are a number of mnemonics that can be used as an aide-mémoire to elicit salient information at each stage of the history-taking exercise. These are explored in more detail in Diamond-Fox (2021). Diamond-Fox et al (2023b) also explore the further important aspects of obtaining a history for neurodiverse and non-verbal populations and those in ethnic minority and LGBTQIA+ populations.
Physical examination
Traditionally, the act of performing a physical examination solely with one's hands was deemed the only way in which to affirm or identify a clinical diagnosis. However, technology also has a role to play. Evidence-based recommendations for the health and social care sector, such as those published by the National Institute for Health and Care Excellence (NICE) integrate technology appraisals for the use of new and existing medicines and treatments within the NHS.
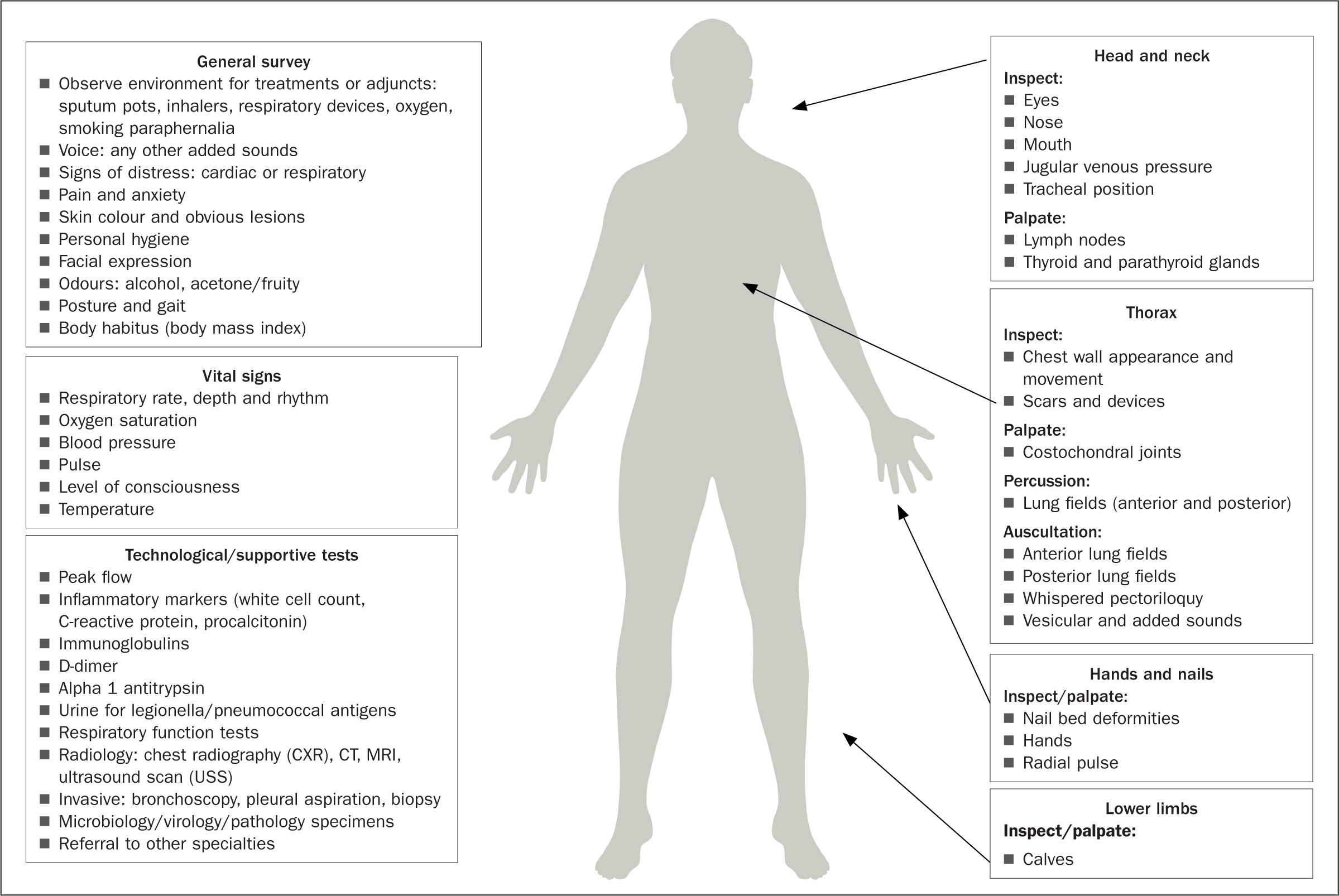
The use of technology is particularly useful where diagnostic reasoning and stratifying disease severity are concerned. This then requires the ACP to possess essential skills of diagnostic interpretation, the fundamental principles of which are explored further by Roberts et al (2023). The focused respiratory examination, depicted in Figure 1, incorporates a traditional physical examination with common technological diagnostic testing.
Abnormal signs on physical examination
Voice
Face
Hands/nails
Neck
Thorax
Breath sounds
Added sounds
Tools and scoring systems
In the presence of abnormal findings, clinicians may opt to use a risk-stratification tool or clinical scoring system. These are designed to present evidence to support decision making and treatment options as well as predicting outcomes and managing risk while improving efficiency (Dambha-Miller et al, 2020). It is pertinent to ensure any tools used have a strong evidence base supported by practice. Many have been quality checked through systematic review or other research process. Some commonly used systems/tools in respiratory diagnoses are as follows:
Conclusion
This article has explored the consultation and clinical assessment skills required to perform a comprehensive history and clinical examination of those presenting with common respiratory pathology. Through clinical reasoning and effective communication, ACPs are often best placed to determine the nature of a patient's condition and focus on appropriate investigation techniques, which will guide the appropriate course of treatment.