

A clean hospital is a cornerstone for sustainable health care because a clean environment reduces the rates of healthcare-associated infections (HCAIs), which are associated with longer hospital stays, increased use of personal protective equipment (PPE), more expensive treatment with greater risk of serious side-effects, higher acuity care, poorer surviving patient outcomes and higher mortality rates (De Angelis et al, 2010; Kritsotakis et al, 2017; Guest et al, 2019). Hospital cleanliness therefore plays a key role in both planetary health (by reducing the carbon footprint of care) and antibiotic stewardship, which is a global healthcare priority.
Although some environmental cleaning can be undertaken by cleaners, there is a significant proportion of cleaning activities that must be conducted by clinical staff (Loveday et al, 2014). The proportion of cleaning undertaken by clinical staff increases in high-acuity areas such as intensive care units (ICUs), emergency departments (EDs) and theatres. This creates a pressure on staff providing the highest acuity care to also deliver the best and most consistent cleaning results. Enabling these areas to achieve the required cleaning standards meets the financial, social and environmental triple bottom line of sustainability in health care. This is because it is:
Supporting environmental cleanliness should therefore be top of the hospital management agenda. The ‘Clean is Green' project, which took place at a large teaching hospital in the south ofEngland over the summer months ofJuly and August 2024, investigated whether promoting the sustainability benefits of cleaning would motivate clinical staff to engage more with cleaning.
Methods
Audit
Cleaning audits were conducted by the hospital's environment monitoring team (EMT), according to the National Standards of Healthcare Cleanliness (NHS England/NHS Improvement, 2021). The audits were recorded and reported using the FM First software (v2024.1, Asckey Data Services Ltd). The Functional Risk (FR) category of the clinical area was recorded as part of the audit:
Promotions
Posters were designed outlining the way in which cleaning contributed to more sustainable health care and the social impacts HCAIs can have. These were laminated and displayed in communal staff areas across the hospital, from the beginning of July, with approval sought where necessary and used as an opportunity to engage in opportunistic informal conversations with clinical staff to promote the work. The FR1 areas known to struggle with clinical cleaning were particularly targeted. Although domestic cleaners were not actively excluded from engaging with the study, a high proportion had English as a foreign language. To include the domestic cleaners and ensure their understanding and engagement would have required translating core materials into several languages and this was beyond the remit and budget of the current project.
Survey
An anonymous short survey was made available to staff in September, following the cleaning promotions. This was accessed via a QR code, which were routinely used in the Trust for short staff surveys, displayed in communal staff areas, added to ward notice boards and promoted at an Infection Prevention Awareness Event in October. The survey data were downloaded and analysed in Excel. One member of the domestic cleaning staff responded to the survey but this was excluded as one such response was insufficient to draw any conclusions.
Poll
A single question poll was conducted in October among clinical staff who attended the drop-in Infection Prevention Awareness Event outside the staff canteen. Responses to the poll and associated comments made to the auditor were recorded immediately and transcribed the same day.
Results
Promotions
The promotion of cleaning as a sustainable healthcare intervention was essentially non-targeted, with staff communal areas being used to reach clinical staff of all disciplines, from all specialties and across all bands. FR1 areas known to struggle to achieve consistent effective cleaning received the same posters but also verbal promotion of the links between sustainability and hospital cleanliness. Two aspects of sustainability were targeted in the education posters, both linking cleanliness to reduced rates of HCAI. One highlighted the environmental impacts of HCAIs and one focused on the social benefits of a clean hospital environment. The content of the posters are summarised in Table 1 and Table 2. Although the environmental impact of health care is well documented and understood by the growing population of sustainability-informed clinicians, there is still a knowledge gap for frontline staff. The aim of the posters was to start building awareness of the causes of high-carbon care and the actions that can be taken to mitigate it.
| Issue: poor environmental cleaning leads to more HCAIs | Impact on the environment | How can cleaning reduce impact? |
|---|---|---|
| HCAIs mean longer stays in hospital so more family travel, more energy use in high care, more equipment used (uses more electricity), and more staffing needed | Air pollution | Better cleaning delivers fewer HCAIs and fewer and shorter high care stays. Less travel for families, reduced energy usage, fewer machines (eg infusion pumps) needed for effective care |
| Increased use of personal protective equipment (PPE), particularly gloves, increased pollution of watercourses due to effluent-containing pharmaceuticals leads to ecosystem change downstream | Deforestation, landscape degradation, loss of biodiversity | Prevention of HCAIs reduces need for gloves for contact, reduced prescribing of antibiotics and additional medications |
| Increased use of medical equipment | Depletion of scarce resources | Equipment used for higher acuity and longer stays, so reducing these reduces need for equipment |
| Increased use of PPE, single-use plastics, medical devices | Plastic pollution, incineration of waste | Better cleaning reduces HCAIs, so fewer antibiotics given, which means fewer IV giving sets used. Patients with HCAIs likely to be nursed in isolation, so use of PPE impacted, more infusions means more devices required |
| Population group | Social impact of HCAIs |
|---|---|
| Patients | Higher risk of extended stay, which leads to lost earnings or education, higher risk of complications (may be long lasting, affecting ability to engage with education or future work), loss of social network, psychological impact of longer stays, and higher acuity care |
| Staff | Low morale associated with HCAIs and poor environmental cleanliness, higher stress with busier unit/higher acuity |
| Wider community | Parents have loss of work, loss of earnings, loss of family time with siblings, lack of social network. Impact on school attendance for children or siblings. Impact on mental health of family members. |
| Vulnerable groups (carers, disabled people, ethnic minorities, homeless) | People with complex medical histories more likely to be admitted to hospital so disproportionately impacted |
The social impacts of HCAIs are rarely addressed as part of infection prevention teaching or campaigns, yet it is arguably the most pertinent and lasting aspect for patients and families. This campaign sought to bring fresh air and greater engagement with hospital cleanliness promotions and therefore the social side was considered an important component to highlight. This list was not exhaustive and could have included impact on public faith in the hospital, reputational damage and risk of litigation.
Cleaning audit pass rate increased during the ‘Clean is Green’ project
Audit results suggested a clear drop in cleaning audit failure across the hospital following promotion of ‘Clean is Green’ in the summer of 2024 (Figure 1).
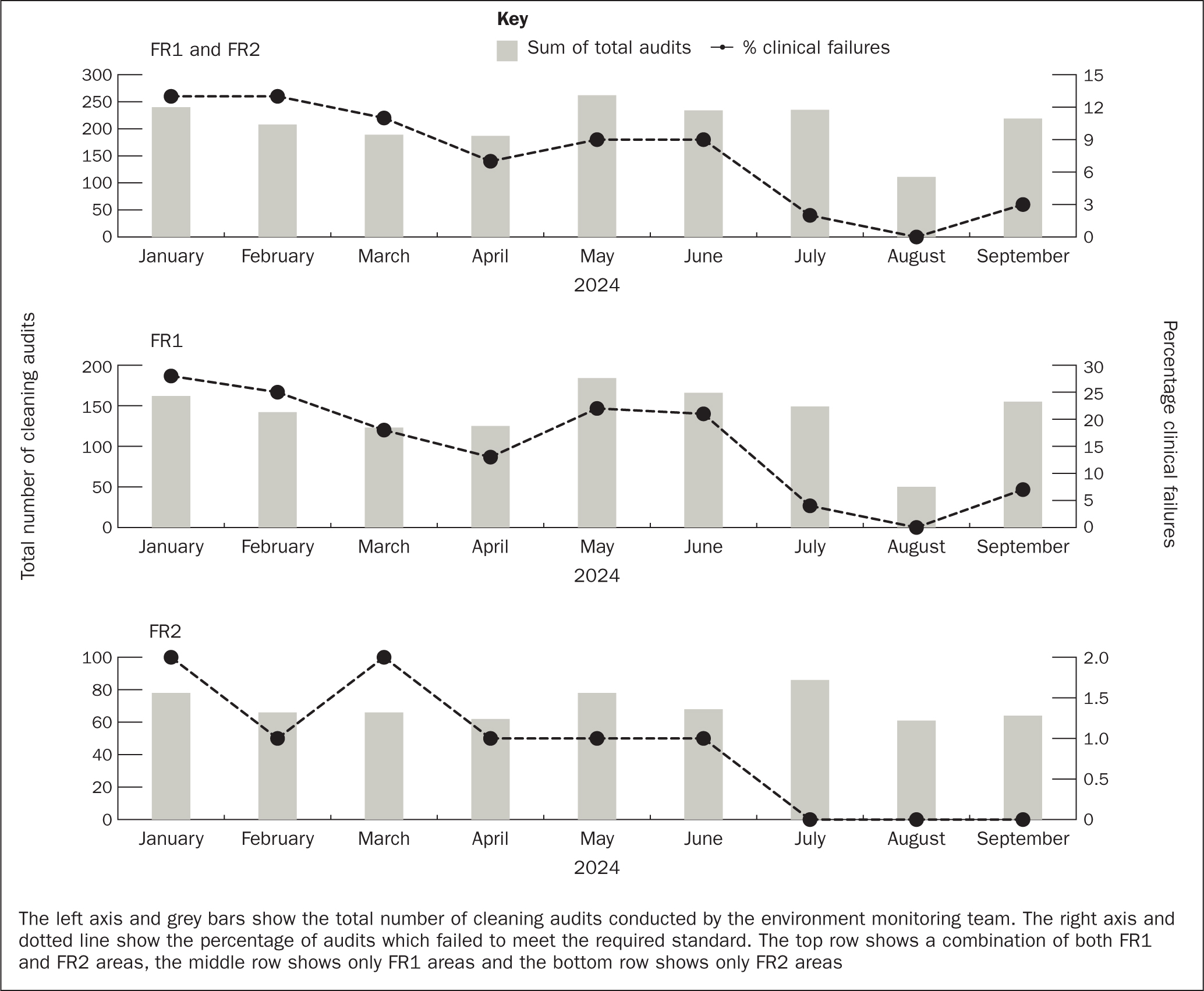
FR1 areas were audited approximately weekly and had a 98% pass mark on the National Standards of Healthcare Cleanliness (NHS England/NHS Improvement, 2021), while FR2 areas were audited monthly and had a 95% pass mark. Over the summer months of July and August of the ‘Clean is Green’ promotions, a rapid increase in audit success across FR1 and FR2 areas occurred, and the 100% pass rate was maintained for the following quarter in FR2 areas. FR1 areas experienced a slight drop in audit pass rate in September to 97%, but this was still well above the starting point of an 87% audit pass rate in January 2024.
Looking in more detail at the audit pass rate revealed some interesting patterns in repetitive failure and the further potential impact of‘Clean is Green’ promotions (Figure 2). Following the audit history reset that occurred at the start of April, by June, seven clinical areas were black in the BRAG rating (Figure 2a) indicating repetitive failure in the same areas. Throughout July and August there were no black audit failures, suggesting that clinical areas that had been struggling were now performing more effective cleaning. A similar pattern was evident in Figure 2b as the number of red and black rated areas were almost the same, but the number of areas contributing to the black bar was almost half that of the red bar. This again suggests that a small number of clinical areas were failing multiple cleaning audits and being black rated repeatedly. This offered an opportunity for targeted interventions such as ‘Clean is Green’.
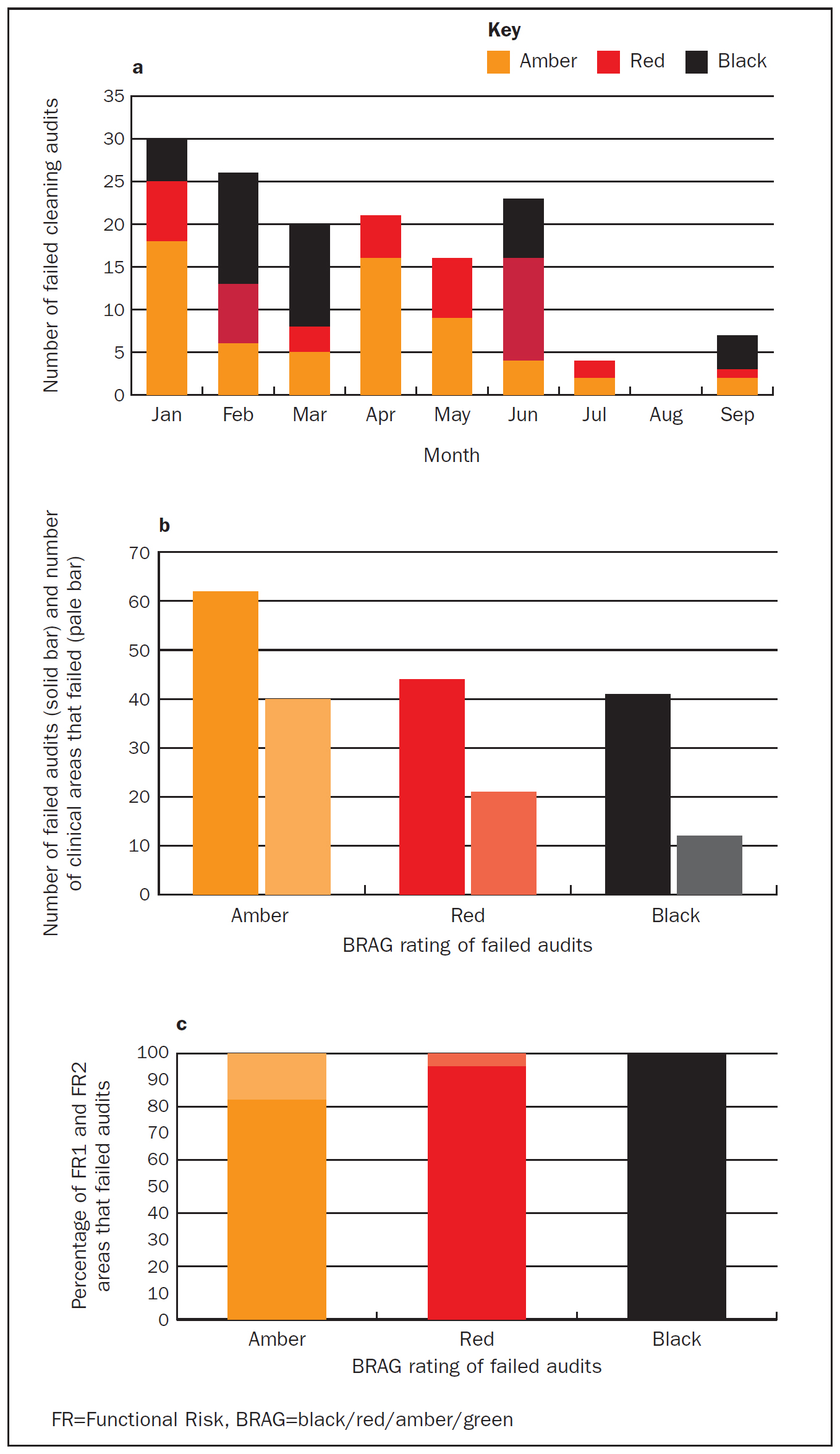
Figure 2c demonstrated that the areas contributing the most cleaning audit failures were exclusively FR1 clinical areas. FR2 areas represented 17.5% of amber failures, with most areas passing the subsequent audits as FR2 areas accounted for only 5% of red failures.
Survey and poll results
Although nursing staff undertake the majority of cleaning in many clinical areas, other clinical staff also contribute and the survey was therefore open to any clinical staff. Although aimed at clinical staff, the promotions and survey were available for any member of staff to access, so the project did not actively exclude domestic staff. Nurses were the most numerous respondents (Figure 3, outer circle).
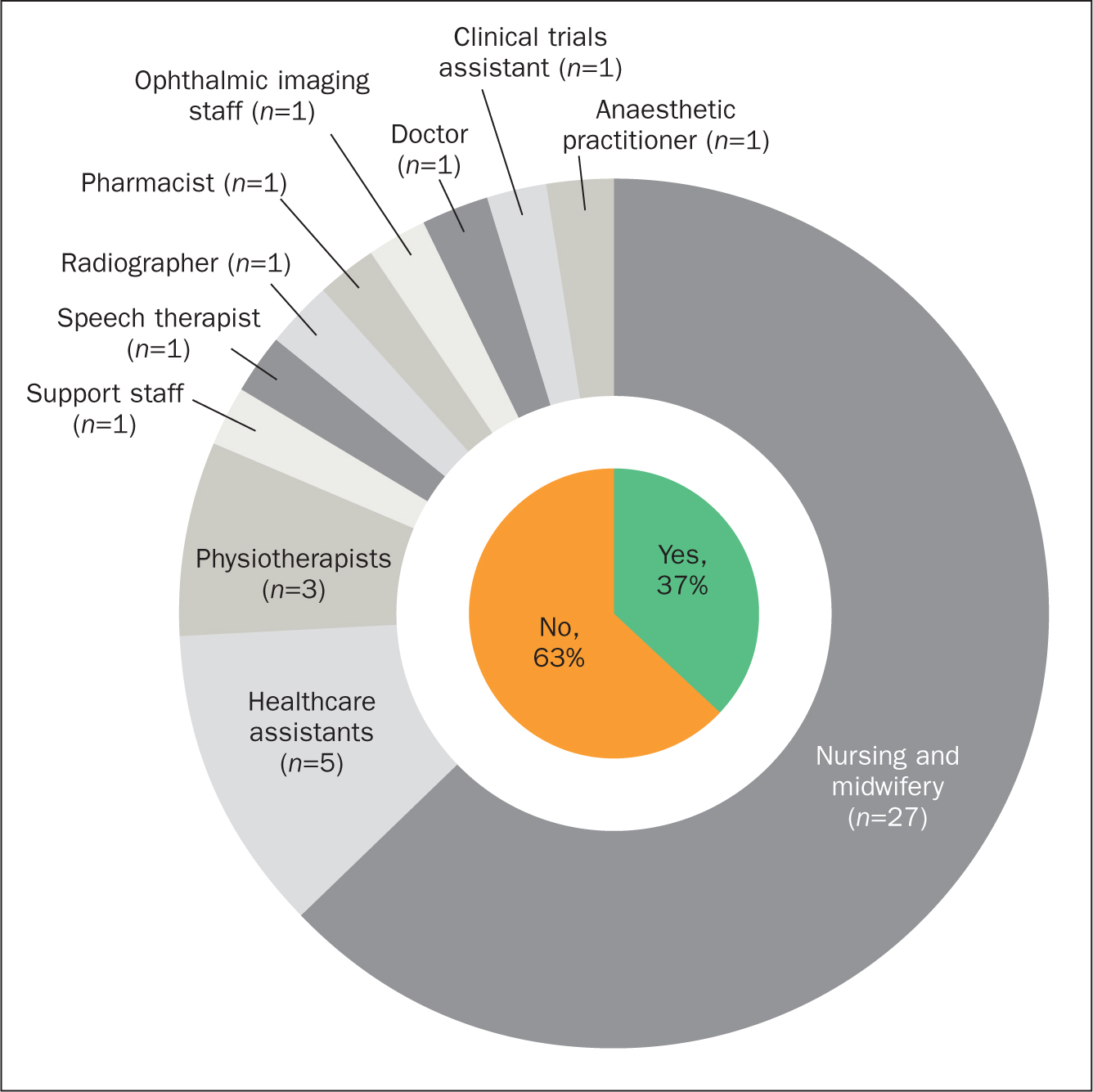
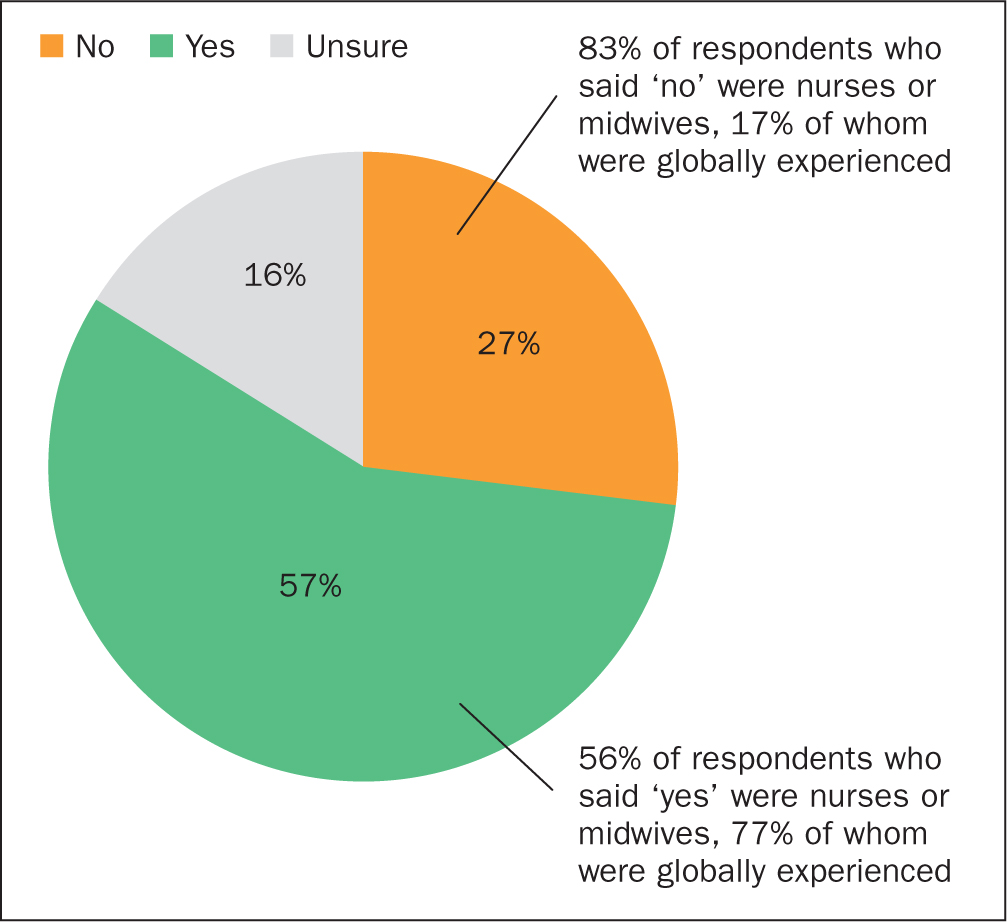
It was notable that over 5 times as many nurses responded to the survey as any other profession, suggesting that infection prevention and sustainable health care are topics with which nurses wanted to engage. Internationally educated colleagues were also well represented, with over one-third of respondents having global experience. This question was intended to draw out links between having experience in hospitals outside the UK and perceptions of sustainability. Although bands 2 to 8 were captured in the sample, by far the most represented were band 5 staff, who made up 45% of the respondents. When asked whether the hospital environmental values reflected their own values, just over half of respondents (57%) agreed (Figure 4). Of those who felt the hospital values mirrored their own environmental values, more than 50% were nurses, almost all of whom were globally experienced. Of the 12 staff who felt they valued the environmental more than the hospital did, only 2 were globally educated (just under 17%). This disparity would be interesting to follow up with more detailed interviews about global practice and perceptions of sustainability.
Of the 43 respondents to the survey, when asked about which options were part of sustainable health care, all identified correct waste segregation and 98% identified both infection prevention and effective cleaning. Enabling efficient patient flow was also ranked highly, with 93% of respondents identifying it as part of sustainable health care. Other options that were less commonly selected were recycling packaging, reducing IV medication use where possible and use of reusable blood pressure cuffs, with a few comments reflecting some concern about reduction of IV medications compromising patient care. In total, 93% of respondents identified mobilising patients to reduce the risk of HCAIs as a nursing/allied health professional (AHP) intervention that promoted sustainable health care, while 100% linked the cleanliness of the clinical environment to sustainable care. In a separate question, 93% identified cleaning as both a low-carbon and low-cost means of reducing HCAIs. Interestingly, 57% identified accurate clinical notes as a nursing/AHP intervention for sustainable care, suggesting at least some respondents were ticking every option available or thinking very broadly about how effective care is more sustainable care. Some 63% of respondents felt empowered to promote cleaning as a sustainable health care intervention.
A single question poll was conducted during an Infection Prevention Education Event for all staff. To the question ‘If cleaning medical equipment properly could reduce the carbon footprint of the hospital, would that motivate you to do it?’ 89% responded positively. Of those answering ‘no’, several said that cleaning was part of safe clinical practice and they would clean properly regardless of the impact on the carbon footprint, or that it was a very minor motivation compared with infection prevention. One consultant doctor responded ‘no, but I don't clean anything’, suggesting that educating the multidisciplinary team would be beneficial for both patient safety and planetary health. The most common response was curiosity and a request for more information on how cleaning was linked to carbon footprint.
Discussion
Taking the data from Figures 1 and 2 together suggests a picture of two halves within the same hospital. FR2 areas responded well to the BRAG rating and demonstrated the capacity to resolve underlying issues and achieve effective cleaning. FR1 areas were more likely to have repeated failures, suggesting that targeting interventions such as ‘Clean is Green’ to high-acuity clinical specialties may be fruitful. The number of black-rated audit failures reduced over the summer following ‘Clean is Green’ promotions. The project finished in August 2024 with no further active promotion. In February 2025, both FR1 and FR2 areas across the hospital maintained a 100% pass rate on all clinical cleaning audits. Cleaning performance is multifactorial and although the promotions seem to have had a lasting impact, there must be acknowledgement that many other factors could also be contributing to this. A bigger and more targeted campaign would likely produce a more environmentally literate and engaged workforce, with the potential to amplify and give longevity to the results seen here.
The demographics of the survey respondents were notable as the proportion of nurses responding compared with other clinical professions was significant. This may represent a genuine interest in sustainable health care or it may be that nursing staff undertake more cleaning than other professions and are therefore more likely to engage with the topic. When asked about the Trust environmental values reflecting their own, the vast majority of those answering negatively were nurses. The responses to the survey may therefore indicate an increasing green literacy in the profession through inclusion of healthcare sustainability in the nursing curriculum (Barna et al, 2012; Àlvarez-Nieto et al, 2022) or through personal interest and responsibility, which is not matched by opportunity or empowerment for change in the workplace. Of particular interest was the proportion of globally experienced nurses who felt the Trust attitude to sustainability reflected their own. This may be that globally experienced nurses have experienced care environments and cultures where sustainability is not currently a priority, and their current Trust in England was making good progress by comparison; or it may be that green literacy of globally experienced nurses was reduced compared with those who have always practised in the UK. This is speculative as there is a paucity of evidence. Although there are many articles on including healthcare sustainability in nursing education, very few could be found that looked at this topic in low-or middle-income countries (reviewed by Tiitta et al (2024)). The few that were conducted outside the UK, Europe and Australia, suggested that nurses' perceptions of the value of environmental literacy and engagement with sustainability education are highly variable (for example, Cruz et al (2018) and Amerson et al (2022)). The identification ofwaste management as a key aspect of sustainability by all respondents came as no surprise as this had been a focus in the Trust in recent months.
Conclusion
Continuation of the improvements seen in this project are a key factor in the ongoing impact and success. Sustainability modules as part of e-learning are an option but may not promote curiosity and do not enable discussion. It is suggested that including effective cleaning as part of the Trust/provider green plan and antimicrobial stewardship strategy would give the opportunity for infection preventionists (IPs) as well as sustainability teams to continue promotion of cleaning. IP nurses have played a key role in the introduction of many changes to sustainable health care and as clinical cleaning already sits within the IP remit, this is a comfortable fit. It is also perhaps an indicator that sustainability link nurses are needed to champion ‘Clean is Green’ at a local level. Building on from this small-scale study, the next iteration should be promotion of ‘Clean is Green’ to all clinical and domestic staff. This would involve multilingual engagement and buy-in from contract managers but would ultimately deliver a more empowered joint workforce.
The survey was a starting point for gauging engagement and knowledge of the clinical staff with the important topic of sustainable health care. Many poll respondents showed considerable interest in the idea that cleaning could impact the hospital's carbon footprint and wanted to know more. The thirst for knowledge about environmental sustainability and its application to practice underscores the epistemic and perhaps diversive nature of the curious nursing workforce and the timeliness of the ‘Clean is Green’ project as one avenue to contribute to satisfying that curiosity.