
Oropharyngeal dysphagia (OD) is a significant problem for neurological and non-neurological patient populations in acute care, occurring in up to 71% of patients with neurological disease. It is associated with weight loss, dehydration, urinary tract infections, choking, aspiration and pneumonia (Karagiannis et al, 2011).
OD is common in all critical illness, but especially neurological illness, and is experienced by up to 91% of patients in neurological intensive care units (Ponfick et al, 2015). Post-extubation dysphagia is increased in patients with neurological problems, with Macht et al (2014) finding it in 93% of patients.
OD occurs in 42-67% of patients with acute stroke (Perry and Love, 2001) and correlates with lesion site. Patients with stroke and OD are significantly more likely to get pneumonia, more likely to be treated with antibiotics, have higher mortality rates and are less likely to get discharged home.
Postoperative dysphagia following anterior cervical spine surgery is commonly reported in the literature and, in some cases, symptoms persist for longer than 12 weeks (Rihn et al, 2011). It is associated with increased admission length and mortality rates (Cameron et al, 2018).
Speech and language therapy role in acute dysphagia
An assessment by a speech and language therapist (SLT) aims to diagnose the presence or absence of OD and the cause and characteristic features. This information can contribute to overall medical diagnosis. An individualised management plan is based on this as well as the patient's wishes and the risk factors that may contribute to swallow safety. This may include: diet/fluid texture modifications, a rehabilitation programme, alternative feeding, strategies promoting safe feeding and interventions to reduce the risk of aspiration pneumonia. Acute management of OD requires a multidisciplinary approach to maintain patient safety, promote recovery and reduce the risk of secondary complications.
Risk factors for aspiration pneumonia
Not all patients who aspirate develop pneumonia. Langmore et al (1998) and Hibberd et al (2013) found that dysphagia was an important factor, but usually not sufficient to cause pneumonia unless other risk factors were present. These included: being dependent for oral care and feeding, having poor oral hygiene, multiple medical diagnoses or medication, tube feeding and stroke. Many of the identified risk factors are frequently present in the acute neurological patient population and may indicate a more cautious approach. Removal or control of risk factors may decrease the risk of aspiration pneumonia.
Identifying and referring
A core nursing role is assessing patients' conditions and coordinating the input of other professionals (Burton, 2000). They may be the person to identify a swallowing difficulty and refer to an SLT or to observe if the treatment plan is not being tolerated. People with acute stroke should have their swallow screened on admission and, if problems are identified, assessed by an SLT within 24 hours (National Institute for Health and Care Excellence, 2008).
Overt symptoms of OD include: coughing or choking when eating and drinking, being unable to chew food properly and losing food and drink from the front of the mouth. Less commonly understood is that aspiration can by silent, meaning the patient is not sensate to aspiration and does not cough in response. Garon et al (2009) found that 54.5% of patients referred for videofluoroscopy aspirated silently whereas Daniels et al (1998) found that the prevalence in acute stroke was 67%.
Suspecting silent aspiration requires different clinical observations. Garon et al (2009) found that the highest rates occurred with brain cancer and brain-stem stroke. Clinical symptoms included wet voice, dysarthria (slurred speech), drooling, inability to cough on command and an absent gag reflex. Recurrent, unexplained pneumonia (especially if right sided) in a patient with a neurological impairment should also warrant a referral to SLT and any symptoms of a new chest infection in a patient with dysphagia needs to be investigated as possible silent aspiration.
Management
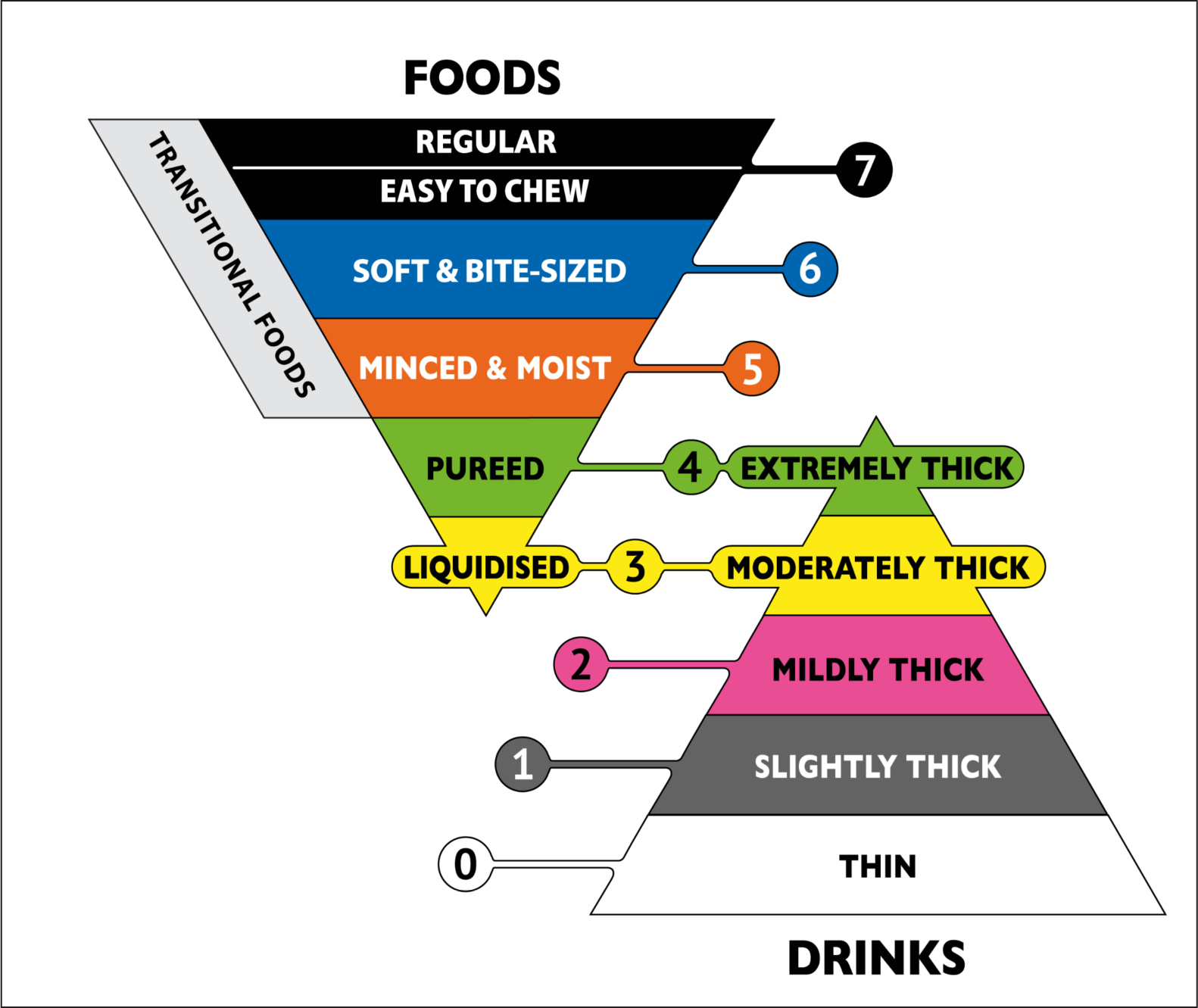
Diet and fluid modification is the most commonly known form of dysphagia management, with tube feeding in the most extreme cases. In acute dysphagia, the recommendations for food and drink will likely change frequently as the patient improves, deteriorates, or their tolerance fluctuates; often in line with their changing medical status. Clear communication between SLTs, nurses and dietitians and handover between nursing shifts is essential. Descriptors for food and fluid consistencies in the UK are changing to be in line with the International Dysphagia Diet Standardisation Initiative (www.iddsi.org) (Figure 1).
Patients with dysphagia pose many nursing challenges, including maintaining oral hygiene, hydration, nutrition, safe feeding and medicine management (Ilott et al, 2013). Nurses have the skills to anticipate and identify these challenges (Long et al, 2002) and managing them are equally important as diet and fluid modification in reducing risk of aspiration pneumonia.
There is a strong correlation between poor oral hygiene and pneumonia (Sjögren et al, 2008), including in those who are nil-by-mouth (NBM). Thorough and regular oral care with a toothbrush and toothpaste is essential for all patients with dysphagia. Foam swabs are not effective and should not be used instead of a toothbrush (Pearson and Hutton, 2002). The oral hygiene of patients who are NBM is particularly vulnerable (Ohno et al, 2016) and aspiration of oral secretions is also associated with pneumonia (Scannapieco, 2006). SLTs should liaise with nursing teams to advise on safe delivery of oral care for patients who are NBM.
To maintain safety while maximising nutritional intake, patients with OD require a personalised management plan for feeding, which will largely be delivered by nurses. Patients should be seated upright for eating and drinking and, if being fed, the feeder should sit at eye level. Other adjustments may include slow pacing of feeding, hand-over-hand feeding, prompting or checking the mouth is clear of food (Layne, 1990) and environmental adaptations such as reducing noise and distractions (Cleary et al, 2008; Cleary 2009). Feedback on problems with the feeding plan or changes in the patient are essential to safe management.
Conclusion
Many interventions essential to the safe management of patients with acute dysphagia are delivered by nurses, including oral hygiene, positioning, feeding strategies, and environmental changes. Joint working between nursing and SLT teams is vital.