
Heliotherapy, the therapeutic use of sunlight, has been used for centuries in the treatment of skin disease (Hönigsmann, 2013). Phototherapy with artificial sources of ultraviolet (UV) radiation is more effective than sunlight, because reducing exposure to harmful and less beneficial rays allows a higher dose of effective UV to be given. The phototherapies remain a treatment option for skin conditions such as atopic eczema, urticaria and vitiligo.
Psoriasis is the main indication, accounting for more than 50% of treatment courses (Ibbotson, 2018). First-line therapies for psoriasis include topical corticosteroids, vitamin D analogues, tar and dithranol. As a second-line therapy, UV treatment is considered appropriate when topical therapies are not controlling the patient's psoriasis adequately or when psoriasis is so widespread that topical application is not practicable. These treatments should be considered before the use of third-line systemic treatments, such as methotrexate or biological interventions (Ling et al, 2016), although individual patient circumstances need to be taken into account.
Psoriasis
Psoriasis is a chronic, multisystem inflammatory disease, predominantly affecting the skin and the joints, which is present in 2–3% of the world's population (Ayala-Fontánez et al, 2016). The precise aetiology remains unknown, but psoriasis is recognised as a disease with an element of inherited susceptibility. One parent with psoriasis gives their child a 1 in 4 chance of inheriting the disease. This susceptibility can be triggered/exacerbated by environmental factors such as stress, physical trauma, infection, alcohol, smoking, obesity and certain medications, including lithium and beta-blockers.
Psoriasis is an immune-mediated disease (Ayala-Fontánez et al, 2016), with immune cells (T cells) becoming overactive and producing inflammatory factors that leads to cell damage, keratinocyte hyperproliferation and inflammation (Wong et al, 2013).
The most common form of the disease is plaque psoriasis (Figure 1). The signs and symptoms of the disease vary with the subtype of the condition (Psoriasis Association, 2020) and are summarised in Table 1.

| Type of psoriasis | Presentation |
|---|---|
| Plaque psoriasis |
|
| Guttate psoriasis |
|
| Palmoplantar psoriasis |
|
| Pustular psoriasis |
|
| Erythrodermic psoriasis |
|
The history of light treatment
UV therapy has developed over many centuries, with its use increasing in the 20th century with the development of UVA and UVB sources. UV can be subdivided as follows:
The shorter UVB wavelengths have more energy and therefore more potential to burn the skin, while longer UVA wavelengths penetrate deeper into the skin. UVC is not used in the treatment of skin disease (Singer and Berneburg, 2018).
Over 3500 years ago, vitiligo patients in Egypt and the Indian subcontinent were exposed to sunlight after ingesting an extract from the plant Ammi majus (bullwort). Only relatively recently, in 1896, Danish physician Niels Ryberg Finsen developed a carbon-arc lamp to treat skin conditions such as skin tuberculosis. In 1923, American dermatologist William H Goekerman treated psoriasis using artificial broadband UVB (BB-UVB) radiation and topical coal tar. BB-UVB alone was then found to clear mild psoriasis. By 1976, the best wavelength for psoriasis treatment was identified as being around 311 nm, but it took almost a decade for narrowband UVB (NB-UVB) lamps to become commercially available (Hönigsmann, 2013). Not until 1984 was the clinical effectiveness of NB-UVB as a treatment for psoriasis confirmed (Weelden et al, 1988).
In 1947, 8-methoxypsoalen (8-MOP) and 5-methoxypsoralen (5-MOP) were identified as active ingredients in Ammi majus. By the 1970s, high-intensity ultraviolet A (UVA) tubes were developed and used with oral 8-MOP to treat psoriasis. The term PUVA was used to represent treatment with psoralen and UVA. NB-UVB and PUVA treatments remain the phototherapy interventions of choice for psoriasis (Ling et al, 2016).
The mode of action involves a number of mechanisms, mirroring the complexity of the disease. Helper T cells affect the immune response by differentiating into subsets: in humans, Th1, Th2 and Th17 are three main subsets. Psoriasis lesions have increased levels of Th1 and Th17 cytokines and an associated decrease in Th2 cytokines. Phototherapy is believed to inhibit Th1 and Th17 cells while upregulating the Th2 pathway. The treatment also initiates both apoptosis of various cutaneous cells and immunosuppression of Langherans and other key cells that play a significant role in the inflammatory process of psoriasis (Wong et al, 2013).
UV energy is absorbed by chemicals that are either present in the body (for example, melanin) or introduced into the body (for example, psoralens, which are light-sensitive drugs). In PUVA, these ‘chromophores’ pass on UVA energy, causing DNA damage and apoptosis of pro-inflammatory cells. The effects of PUVA are a result of the deep penetration of the UVA radiation combined with the use of an exogenous chromophore (Singer and Berneburg, 2018).
Psoriasis treatment: NB-UVB or PUVA?
NB-UVB treatment is an effective treatment for psoriasis (Ibbotson et al, 2004). In the 12 months following treatment with NB-UVB, 75% of patients have marked reduction in the use of steroid creams and psoriasis-specific therapies (Foerster et al, 2017), which equates to significant cost savings in drug dispensing for these patients (Boswell et al, 2018). Three-times weekly NB-UVB is more effective than twice-weekly bath PUVA (Dawe et al, 2003; Snellman et al, 2004) and is equally as effective as oral 8-MOP PUVA (Markham et al, 2003). NB-UVB is the first choice of phototherapy for patients with psoriasis because treatment is straightforward, with no evidence of increased skin cancer. It can also be used for children and during pregnancy (Ibbotson, 2018). PUVA should be considered if NB-UVB is not effective or if there is rapid recurrence after treatment. PUVA should also be considered as the first-line treatment for pustular or erythrodermic psoriasis.
The choice of treatment given may depend on availability. Currently, UVB is offered at 42 centres across Scotland, 34 of which offer PUVA treatment.
Oral 8-MOP or 5-MOP tablets are taken 2 hours before each UVA exposure, but there are certain circumstances under which topical application of psoralen is preferred. The psoralen is most commonly administered topically by soaking in a bath of 8-MOP solution, and this is recommended for patients with hepatic dysfunction or gastrointestinal disturbances that affect absorption. It is also recommended to avoid interactions between psoralens and specific drugs, such as warfarin (Halpern et al, 2000). Psoralen can be detected in the eye lens for at least 12 hours after ingestion of the tablets and protective glasses should be worn for this time to avoid increased risk of cataract formation (Ling et al, 2016). This eye protection is usually not needed after bath PUVA treatment, so patients may choose that option to avoid wearing glasses.
Because NB-UVB and PUVA have different modes of action, it is important that a lack of improvement in psoriasis with NB-UVB treatment does not preclude the use of PUVA or vice versa (Ibbotson et al, 2004).
Side effects of NB-UVB treatment
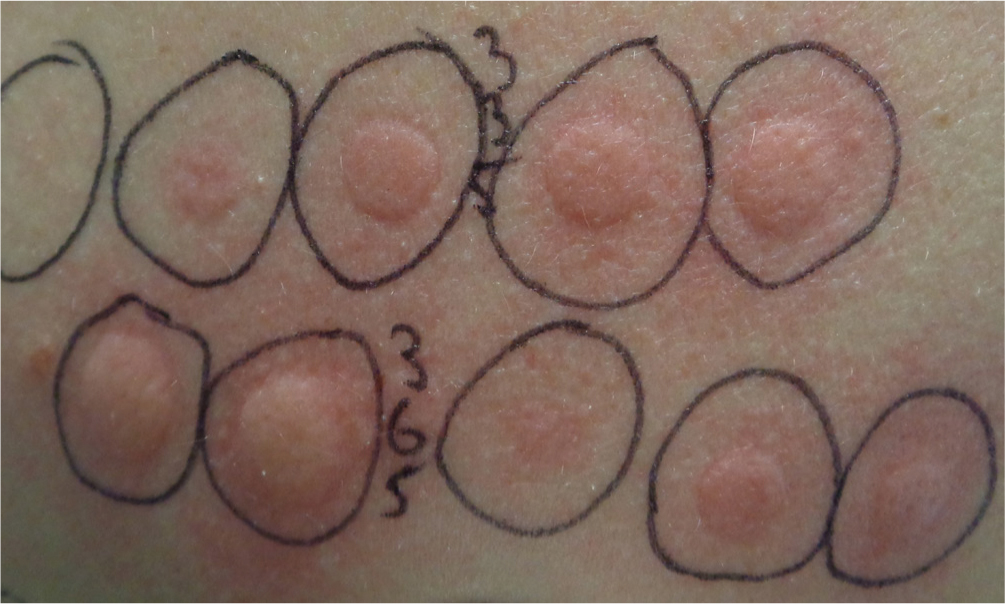
The short term side effects of NB-UVB are erythema (sunburn-type reaction), development of the photosensitivity condition polymorphic light eruption (PLE), skin dryness and tan development. To minimise the risk of erythema, patients commencing on a course of NB-UVB treatment should have a minimal erythema dose (MED) test performed. This involves exposing a small area of skin to a range of doses of NB-UVB radiation. The test area is read 24 hours later because the peak time for development of NB-UVB-induced erythema is 12-24 hours (Ibbotson, 2018). The MED is the dose that produces barely perceptible erythema. NB-UVB treatment is then started at 70% of the MED (Photonet, 2020a).
It has been argued that the MED test approach has no advantages over a fixed starting dose protocol based on the patient's skin type (Parlak et al, 2015) because both methods give rise to equally effective treatment (Dawe et al, 2011), with little difference in the number of treatments given, cumulative dose or side-effects. It was thought the fixed dose protocol would allow for quicker access to treatment.
MED-based starting doses have safety advantages. They ensure that the starting dose is not too high, but they also avoid beginning unnecessarily cautiously. MED testing also allows for drug-induced photosensitivity (Cameron and Dawe, 2000). Testing identifies unexpected photosensitivity conditions such as solar urticaria (Figure 2) or chronic actinic dermatitis (Ibbotson, 2018).
Patients should know that there may be an increased risk of skin cancer and skin ageing after treatment with NB-UVB. A yearly course of treatment with NB-UVB over a lifetime may double the risk of treatable skin cancer; skin cancer review is therefore recommended after 500 treatments (Photonet, 2020b). Although research has not yet shown any significant increase in the development of skin cancers in patients who have had a course of NB-UVB treatment (Hearn et al, 2008), the likely but presently unquantified skin cancer risk highlights that NB-UVB should be used in courses of limited duration where simpler topical therapies have failed (Ibbotson et al, 2004).
Side-effects of PUVA treatment
Patients having PUVA treatment can also develop erythema, polymorphic light eruption (PLE), skin dryness and a tan. To minimize erythema risk, patients commencing oral 8-MOP, oral 5-MOP or 8-MOP bath PUVA should have a minimal phototoxic dose (MPD) test performed. The psoralen tablets are taken 2 hours previously or a psoralen bath is taken immediately before the test. A small area of skin is exposed to a range of doses of UVA radiation. The MPD test area is read 96 hours later because psoralen, plus UVA exposure, provokes erythemal reaction peaking at that time (Ibbotson, 2018). The MPD is judged to be the lowest dose to produce perceptible erythema. Treatment is started at 70% of the MPD dose for oral treatment and 40% of the MPD dose for bath treatment (Photonet, 2020b). Testing establishes an individual starting dose and identifies abnormal responses to light. MPD testing for oral PUVA also ensures that sufficient psoralen has reached the skin to cause a reaction (Photonet, 2020c).
Psoralen tablets can cause additional side-effects (Ling et al, 2016). Nausea is fairly common but minimised by taking psoralen tablets after a light meal. Switching from 8-MOP to 5-MOP tablets can also reduce nausea. PUVA pain/itch, a rare side-effect characterised by a prickling, burning, crawling sensation in the skin can last for minutes or weeks. PUVA pain is a relative contraindication to further administration of oral PUVA as part of treatment because it is likely to recur.
As mentioned earlier, protective glasses should be worn for 12 hours after ingestion of psoralen tablets to avoid increased risk of cataract formation (Ling et al, 2016). Patients with eye problems or a family history of eye disease should wear the protective glasses for up to 24 hours following treatment.
Skin cancer is a well-recognised side-effect of oral PUVA and increased squamous cell cancer risk is dose dependent (Ling et al, 2016). This must be discussed with the patient. Benefits need to be balanced with the risks, but maintenance PUVA should be avoided and treatment regimens should be based on the best possible evidence to provide the greatest benefit with the fewest treatments
To reduce the risk of skin cancer with phototherapy, treatment regimens must be effective and quick, with a low cumulative dose and minimal side-effects (Parlak et al, 2015).
How often should patients attend?
Dawe et al (1998) studied clearance rates of plaque psoriasis in patients attending for NB-UVB treatment. Five times weekly treatment reached clearance more quickly than three times weekly treatment, but required extra exposures and a higher dose of NB-UVB overall. Disease remission time was similar for both. The accelerated clearance rate of the five-times weekly treatment did not justify the extra exposures and higher dose. The study also showed NB-UVB treatment to be more effective in clearing psoriasis when administered three times weekly rather than twice weekly (Cameron et al, 2002).
Erythema is a common side-effect, peaking 12–24 hours after NB-UVB treatment (Ibbotson, 2018), so one treatment-free day should be allowed between exposures to assess erythema response. PUVA treatment has a delayed erythemal reaction, peaking 96 hours after exposure to psoralen and UVA (Ling et al, 2016). At least two full treatment-free days should be allowed between exposures to assess erythema response. Effective, safe UVB is given three times weekly and PUVA treatment is ideally given twice weekly.
What incremental dose should be used?
PUVA treatment for psoriasis is administered in incremental doses. The doses are usually increased in 40% increments, which are reduced to 20% or 10% increments, as necessary. The incremental regimen for NB-UVB or topical PUVA is usually lower: increments start at 20% and are reduced to 10%, as necessary. Reduction in increment depends on erythemal response (Photonet, 2020a).
When should treatment stop?
Current practice is to treat the psoriasis until it is clear or until only small areas remain, described as minimal residual activity (MRA); following this, four further treatments are given. Early discharge leads to inadequate improvement of psoriasis and possibly short disease remission. Delayed discharge exposes patients to unnecessary risks and also wastes resources. A discharge protocol is essential to help determine when to stop treatment, and when the patients should seek advice (Photonet, 2020a).
The role of the phototherapist
Between 1989 and 2001, 38 legal claims were filed against dermatology departments in Scotland. Eight related to phototherapy, six of which were upheld and resulted in the largest awards made against dermatology services. All six claims involved episodes of burning after UVB or PUVA treatment (Drummond et al, 2003). In England, between 1995 and 2009, there were 166 legal claims against dermatology departments. Of these, 38 claims related to phototherapy, with 37 being secondary to episodes of burning after UVB or PUVA treatment (Ong and Coulson, 2011).
Nurse phototherapists are accountable for their decision-making in relation to treatments given and must be able to justify their actions based on sound evidence. Accurate record-keeping is essential. Knowledge of contraindications to treatment is vital and ongoing training is mandatory. Photonet, the National Managed Clinical Network for Phototherapy in Scotland, is an invaluable resource both for staff and patients. It provides training through an online module and yearly study days. Photonet also provides standards, protocols and guidelines against which departments can measure the service they provide (Photonet, 2020d). Some areas in England have set up similar groups to provide service guidance, protocols and standards. Examples are groups in the South East of England Phototherapy Network (2020) and in the Yorkshire Phototherapy Network (Yorkshire Phototherapy Network, 2020).
Phototherapists need to be aware that they offer more than straightforward light therapy (Figure 3). Psoriasis is a disease that has a significant impact on patients' quality of life, affecting their mood, sleep patterns, relationships and work-life balance. Patients' privacy, dignity and confidentiality can be difficult concepts to uphold in a busy outpatient clinic, but time needs to be made available to offer support and advice to patients, as required (Ayala-Fontánez et al, 2016).
Conclusion
NB-UVB and PUVA are effective treatments for psoriasis and, as proven second-line therapies, they avoid the need for systemic and biological therapies in many patients. Both NB-UVB and PUVA have side-effects that must be discussed with patients and weighed up against their known benefits. Careful adherence to research-based regimens for frequency of treatment, dose increments and treatment numbers will ensure that the risks to patients are minimised and the treatment benefits are maximised. The development of Photonet in Scotland and similar networks, such as South East of England and Yorkshire, has been supported by the adoption of similar standards throughout the UK (British Association of Dermatologists, 2016). This has provided a means for effective dissemination of information between individual phototherapy departments.