
For patients with chronic health issues adhering to the prescribed treatment is key to their ability to cope effectively with their illness and enjoy a better quality of life. However, research indicates that adherence is an issue for many chronically ill individuals. According to the World Health Organization (2003), adherence to treatment is a challenge for no less than 50% of patients with chronic conditions.
The same issue applies to people living with continence and voiding issues, many of whom are also chronically ill (e.g. those with neurological conditions such as spinal cord injury, multiple sclerosis or spina bifida). The gold standard of treatment for this group of patients is intermittent self-catheterisation (ISC). It is well-documented that ISC ensures better quality of life (Vahr et al, 2013) and good bladder health (Weld and Dmochowski, 2000) for this group of people. However, studies reveal that ISC adherence rates decline significantly over time. In the USA, for example, there is a 50% reduction in adherence rates in the first 5 years after rehabilitation discharge (Cameron et al, 2010).
Poor adherence rates
Why is this the case?
Although the long-term benefits of adhering to ISC treatment are clear—better bladder and kidney health and better quality of life—research indicates that these long-term benefits do not provide patients with sufficient motivation to completely change their behaviour and establish an ISC routine (Coloplast Market Study, IC Research 2015, data on file (VV-0206732). As humans, we are far more short term in our thinking. We focus on the here and now and are unlikely to change existing behavioural patterns in response to distant ‘threats’ such as long-term, negative health impacts.
‘If the patient is not experiencing incontinence, the benefit is conceptual. It's about reducing future risks. The patient must face the burden of ISC right now, yet they do not feel the benefit immediately. This is the kind of patient that may drop out.’
What can we do about it?
Changing health-related behaviour is challenging. To do it successfully, we need to understand the mechanisms governing adherent and non-adherent behaviour. Those working with continence care know, based on their clinical experience, why patients do not adhere to the treatment. But in order to systematically address adherence issues—and promote an evidence-based culture in nursing—we need to have deeper insights that shed light on the actual barriers to, and supporters of, adherence.
To collect such evidence, Coloplast embarked on a qualitative research study to identify more exactly the drivers that result in adherent behaviour. The study was conducted in the autumn of 2016 in the UK, France, Germany, Spain and the USA. A total of nine interviews were conducted, using an interview framework based on the Septigon model. Doctors and nurses were interviewed to investigate barriers and promotors for adhering to ISC as prescribed. This article presents our findings.
Methodology
To conduct the study, we started by identifying an engaged group of doctors and nurses working in urology or rehabilitation wards in five countries, all of whom had extensive experience with:
We then interviewed each of these professionals regarding their experience with patients' adherent and non-adherent behaviour. The purpose of the interviews was two-fold:
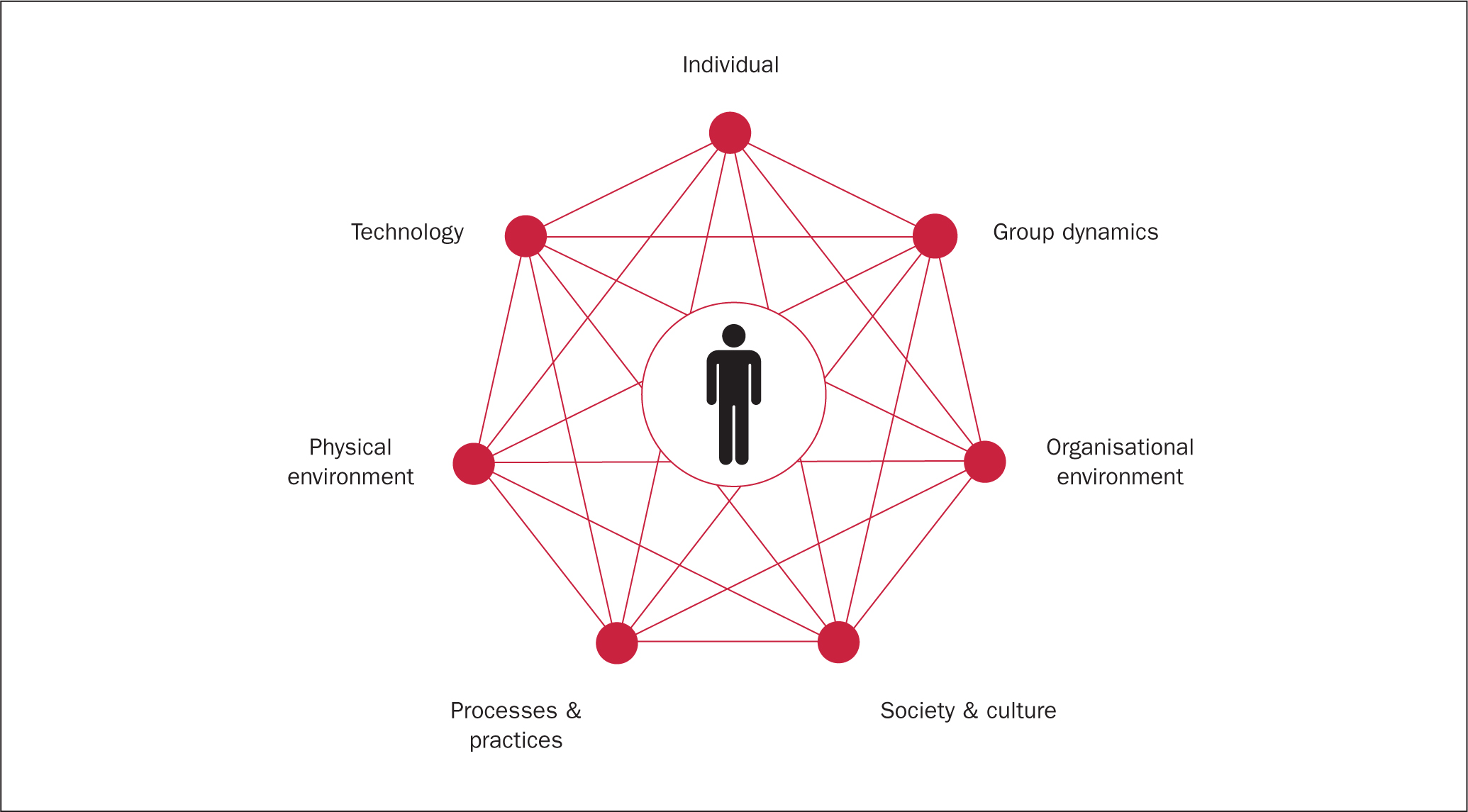
To guide our questions, we used the Septigon, or Septa, model (Grech et al, 2008) (Figure 1). The model was introduced in 2007 and provides a structured way of examining how different factors in a person's life influence their behaviour. It is used extensively to understand and identify the root causes in accident investigations and as a part of prevention programmes.
The interviews generated an abundance of barriers to and promoters of ISC. We had to structure these in a way that would allow us to understand the psychological processes that influence adherent behaviour in this particular patient population.
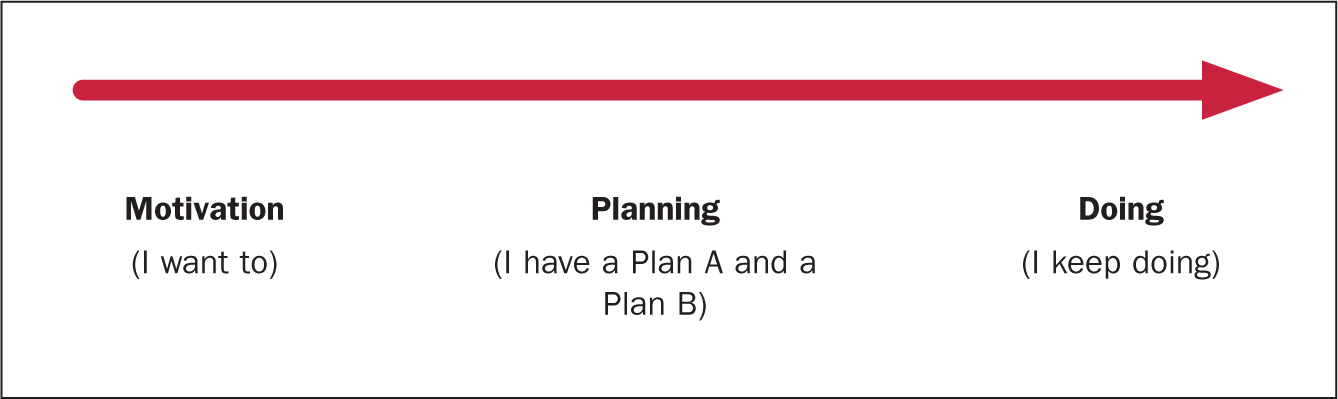
We chose to use the Health Action Process Approach for this, also known as the HAPA model. This model is a useful method for describing, explaining and predicting changes in health behaviour in a variety of situations, particularly rehabilitation settings (Schwarzer et al, 2011). It has often been applied to understand health behaviour in patients with chronic illnesses and conditions.
The HAPA model argues that a patient typically goes through three phases in order to establish a new health-related routine:
The model does not claim that this is a linear process for all patients. Patients might move back and forth between these phases. For example, if they encounter a new challenge—perhaps a setback in their condition—they can lose their motivation to adhere to the treatment. In such a case, they can only move back to the planning phase once they have rediscovered their motivation.
In the following, we will show how the interview responses helped us to understand the barriers and promoters in each phase that can influence adherent behaviour, specifically among ISC patients.
Results
Phase 1: Motivation
The key to adopting any form of behaviour is having the necessary motivation. It all starts with the proper frame of mind. The health professional's role is to structure the introduction and training of ISC in such a way that they can motivate the patient to accept the treatment. Here, it is important to provide individualised training that addresses the patient's fears and lack of understanding.
Providing individualised training
‘Every patient is a world.’
According to the health professionals we interviewed, for ISC training to be successful it must do the following:
Building trust in the treatment
Trust is a key element in the training session. The patient must trust the treatment and the person recommending it. ‘It's a kind of a contract with a promise,’ commented one nurse, ‘not just in terms of the results, but also in terms of safety and that patients will be supported when they need it.’
Moreover, the training itself has to be more than a ‘how-to’ session. As one nurse in the UK explained, ‘Just “giving” the treatment to the patient is not enough for success.’ In other words, the patient must feel supported and understood. ‘If you have a good rapport with the patient, it makes teaching so much easier,’ commented another nurse, who also provided a word of caution. ‘However, if the initial introduction to ISC is bad, there is a greater risk that the patient will drop out.’ This response begs the question of what constitutes a ‘bad’ session? The health professionals we interviewed explained that things such as lack of time, interruptions or talking down to the patient could contribute to a poor introduction.
Addressing fears
‘Fear and lack of understanding are the greatest barriers.’
Fear can be a powerful barrier to adherence. Fear paralyses and makes it difficult for us to take in new information. When patients are afraid—and present what one nurse in the UK described as ‘the “rabbit in headlights” look’—they are simply not able to grasp the concept of self-catherisation. Whether it is fear of harming themselves, social isolation or accidents, unaddressed fears and concerns can be enough to cause a patient to abandon their treatment. It is not only the patient who is fearful. As one rehabilitation nurse in France observed, ‘There is a fear … from the caregivers, the family, friends, spouse and children about intermittent catheterisation because it's a kind of invasion. [They worry about] the risk of urinary tract infections, the risk of bleedings and things like that.’
Ensuring accurate understanding
Most people go through life without giving their urinary system much thought. For this reason, there is often a fundamental disconnect between the way a patient perceives ISC and what it actually involves. ‘Some of them don't even understand their own anatomy, where things are, and how they work,’ commented a rehabilitation nurse in the UK. This lack of understanding often leads patients to draw inaccurate conclusions, both rational and irrational. On the rational side, some patients think accidental voiding means there is no need for catherisation, as the bladder empties itself. On the more irrational side, some believe that the catheter will puncture the bladder, or they feel that the catheter is too large to fit into their urethra. Uncovering and addressing these misunderstandings are critical steps in motivating the patient to accept ISC.
Because no two patients are alike, it is crucial that health professionals spend time with the patient to identify their fears and concerns. Time must also be spent talking to the patient's family. The health professionals we interviewed often identified family members as an important resource for the ISC patient. Getting them on board in the early stages and making sure that they understand the treatment will not only help to quell fears and uncertainties but their support will be instrumental in helping the patient adapt to ISC routines and keeping them on the path to adherence.
Providing consistent information
Consistency in advice among the health professionals treating the patient is equally important. As a rehabilitation doctor in France explained: ‘Everyone has to convey the same message to the patient. If one nurse says, “You have to use antiseptic,” and the doctor says, “You don't need antiseptics,” and another nurse comes along and says, “No, don't use that antiseptic, use this one,” it's a nightmare for the patient. It gives a terrible impression, because we send the message that it's not a stable treatment.’
Phase 2: Planning
Motivation is not enough to ensure adherence. The patient may want to adhere to the treatment, but this is of little use if they lack the knowledge and skills to perform ISC safely and successfully in any environment and situation. However, once the patient is in a motivated frame of mind, they are ready to work with their health professional to develop a plan of action.
For the plan to work, however, it has to accommodate life outside of the rehabilitation centre or hospital setting. Although performing ISC may seem relatively straightforward in a sterile hospital environment, or in the familiar and private surroundings of the patient's home, performing it on-the-go, at work, at school or in a public place presents a different set of challenges. As a urologist in Spain commented, ‘Once the patient gets out of the motivating environment of the hospital, they are in a helpless environment.’
Planning involves helping the patient to:
Having realistic expectations
Although some patients will immediately see the benefits of ISC, others may struggle to accept the need to self-catheterise. The treatment itself can be a constant reminder that there is something wrong with them. As a rehabilitation doctor in France observed, ‘It's very, very difficult for patients with chronic disease to deal with the here and now because of their non-verbalised expectations. They wait for recovery; they wait for a miracle; they wait for the progress of science—and there is sometimes a major gap between hope and reality.’
Here, the role of the health professional is to be honest, upfront and realistic. It is about helping patients understand the realities of their condition; what self-catheterising involves; and the benefits they can achieve by sticking to the routine. The patient must feel that they have a choice in the matter, and that they can make their own decisions based on an understanding of the risks and the benefits. One urologist in the UK recommended, ‘Give the patient the space to get things wrong. It's okay, as long as they can recognise their mistakes and correct them if necessary.’
Establishing a routine
‘Catheterisation has to adapt to their life, rather than their life adapt to catheterisation. As health professionals, we adapt what is best practice to what will realistically happen.’
Realism comes into play again when designing the patient's ISC routine. Some patients are overwhelmed by the number of times they have to catheterise and believe they will never be able to fit it into their busy lives. The key is to listen to the patient and help them to organise their day, fitting ISC into existing routines and schedules. ‘We want to aim for less than 500 ml in the bladder,’ one rehabilitation nurse advised. ‘So I suggest they do it when they get up. If they have a coffee break or a lunch break, they should go and empty their bladder. They can also make sure they empty their bladder before they leave work.’
For some patients, it is as easy as setting an alarm on their smartphone to go off six times a day. Some health professionals approach developing the routine like a negotiation, where they work together with the patient to build the schedule. The health professional starts by having the patient walk them through their day; then they agree on three possible times—morning, lunch and late evening. This makes it more manageable to fit in the remaining three times.
Creating a plan of action, including a plan B
This is all about addressing the practical aspects of performing ISC. For example, finding out how patients can carry the equipment around in an easy and discrete way. As one urologist from the UK observed, ‘As with your first child, where you end up taking out a lorry load of stuff to be prepared for everything and every eventuality. You don't want that with a catheter patient. Instead, you want to make it a natural, easy part of their everyday living.’
The health professionals we interviewed also highlighted the importance of considering the patients physical ability to perform ISC. Patients must be able to open the package, hold the catheter, insert it, unzip their trousers, etc. This can be difficult if the patient is physically impaired or uses a wheelchair. Physical limitations can also relate to the patient's body type. As one health professional observed, ‘ISC is not easy for obese people due to buried penis and urethral opening.’
The choice of product plays an important role as well. ‘The product must be adapted to the patient, not the patient to the product,’ commented a urologist from Spain. According to a urologist from France, the choice of product and process will often make the difference between the patient adhering to the prescribed number of ISC episodes per day or abandoning the treatment entirely: ‘Products that enable the patient to respect the frequency in any type of environment will enhance the ability to stay on ISC for a long time.’
Finally, some approaches need to be gender specific. For example, one nurse in the UK advises men to stand rather than sit to avoid contamination from the toilet seat. The same nurse advises some women to catheterise lying on the bed on the side with a bag attached.
Since daily life is unpredictable, patients must also have a plan B for when the ideal environment is unavailable. Having a plan B ensures that they will not be tempted to skip a catheterisation, but will still be able to cope with, and master, the situation they find themselves in.
Identifying support resources
The nurses and doctors we interviewed frequently pointed out that family members often play a more important role than peers. Some patients will never tell their friends or colleagues about their condition, whereas they will often have family members with them when they visit the doctor. Other health professionals have been successful in getting patients to identify a person—either at work or at school—who knows about the patient's condition and who will help them to remember to catheterise.
Phase 3: Doing
Doing is about perseverance. It's about patients having and using the skills they have learnt to stick with the treatment, despite the various challenges they may encounter along the way.
For patients to stay in the ‘doing’ frame of mind, and adhere to their treatment, they need to know:
Handling UTIs
When we introduce ISC as the gold standard, patients might conclude that, if they just follow the routine, everything will be fine. If they perform ISC and then get a UTI, this can make them question the efficacy of this mode of treatment. As one health professional put it, ‘UTIs can make them doubt they're doing the right thing.’ That's why it is important to be upfront about UTIs—that they most likely will occur and, if they do, this has nothing to do with ISC as a mode of treatment.
Education helps to prevent UTIs and guides patients in how to discover and treat them correctly if they occur. And education should not be limited to the ISC patient. ‘Education regarding UTIs has to be done not only for the patient but also for the general practitioners (GPs), the caregivers, as well as for the families,’ advised one rehabilitation doctor. UTI education should include helping patients to distinguish between ‘true’ and ‘false’ UTI symptoms. And it should cover when and how they should react to symptoms.
Interacting with the medical community
A number of the doctors and nurses we interviewed highlighted the role of health professionals following discharge. Many of them pointed out that it is critical that the local GP has sufficient understanding of ISC to support it as the gold standard of treatment and offer the right clinical advice to patients. One urologist from France went as far as to say that ‘the main barrier remaining is the GP. Some GPs still don't understand and believe that ISC is dangerous and will give too many infections … And, if the GP doesn't understand, [the patient and] the family won't understand.’ Another health professional corroborated this claim. ‘There have been examples of GPs accidently switching patients to indwelling simply due to cost and lack of knowledge.’
Beside ensuring clinical proficiency in ISC treatment among GPs, it is also important that all health professionals involved in the individual patient's course of treatment work together to support patients and help them stay on the path to adherence. As one urologist asserted, ‘This network is very important. It is a multidisciplinary collaboration.’
When and where to seek help
Almost all the health professionals we interviewed stressed that they had the highest rate of success when they were able to follow up with the patient over an extended period of time. One urologist observed, ‘We do quite well, but we are very lucky because we can arrange follow-up [visits]. [These sessions] help us to get a good understanding of how quickly or how slowly the patient will adapt to the technique … Our drop-off rate is quite low because we're able to offer [ongoing] support.’
Where resources allowed, many of the health professionals interviewed arranged for annual follow-up sessions with patients. At these sessions, they evaluate the patient's condition and make modifications to the routine or products if the patient's situation has changed. Regular review sessions help to ensure that the patient does not develop harmful habits, and that they are still following a course of treatment that is best for their health. This kind of follow-up is also useful because the patient returns with more experience, which can influence the course of treatment. As a rehabilitation nurse from the UK observed, ‘They become the expert in their [own] care and [our] education has to adapt to [their] experiences.’
Regular contact also helps the health professionals to address any inaccurate information the patients may have read online. Health professionals can refute negative or exaggerated reports and stories that patients might have read, and guide them to more reliable information sources that will support them in adhering to the treatment.
One session is often not enough
‘You have to give them the confidence, “You can do this”. This can take days or weeks.’
One of the conclusions that came across in every interview was that building adherent behaviour takes time. Many of the health professionals spoke of the need for several sessions and phone calls in order to overcome the patient's barriers to ISC. One nurse from the UK stressed the need for an unofficial ‘open door’ policy: ‘We have to twist the rules and adapt to patient needs under the management radar.’ This approach often helps patients to stay on track. ‘Being accessible is key, and we have great success with the “open door”. Often people just show up asking for me because they almost know my schedule and that I will take the time needed.’
Conclusion
By applying the HAPA model to our research, we were able to identify several key drivers to adherent behaviour:
Perspectives on patient support
Our interviews also highlighted challenges unique to the two patient groups the health professionals worked with: urology and rehabilitation patients. For rehabilitation patients, the overall challenge for the health professional is that, despite having plenty of time to train the patients, there are often many other challenges the patients have to deal with that can adversely affect their adherence. For example, rehabilitation patients often use a wheelchair, have poor dexterity, and have to deal with depression as a result of their condition. These factors provide both physical and mental barriers to adherence.
For urology patients, the main challenge is that the time that health professionals can spend with them is limited, and in most cases, there is no opportunity for follow-up sessions. Health professionals working in this field often will not know how the patients are doing after the initial training.
It is our hope that health professionals working in the field of continence care can use the insights from our research to structure and improve patient care. Coloplast is committed to continuing our research in this area, so we can work with the healthcare community to design follow-up routines, tools and procedures that can support long-term adherence and, ultimately, ensure better quality of life for patients living with continence issues.