
Intertrigo (also known as intertriginous dermatitis) is one of the four separate conditions that fall under the umbrella term of moisture-associated skin damage (MASD). MASD is a concept that has become generally accepted to describe the spectrum of damage that occurs as a result of the frequent exposure of the skin to various sources of moisture, such as urine or faeces, perspiration, wound exudate, mucus or saliva (Voegeli, 2019).
MASD and ‘moisture lesion’ are non-specific terms used to describe different forms of contact irritant dermatitis that comprise: incontinence-associated dermatitis (IAD); intertrigo (ITD); periwound moisture-associated dermatitis; and peristomal moisture-associated dermatitis (Figure 1).
Interest in the concept of MASD as a clinical problem has grown significantly within nursing over the past decade. However, much of this work has focused on IAD, partly driven by the established association between IAD and the development of pressure ulcers/injury (Barakat-Johnson et al, 2018; Gray and Giuliano, 2018). The 11th revision of the World Health Organization's (WHO) International Classification of Diseases (ICD-11) now contains codes for the separate forms of MASD within the EK02 irritant contact dermatitis section (WHO, 2019).
However, intertrigo has often remained the poor relation in terms of MASD research, with little strong evidence to guide practice. Therefore, effective management often presents a challenge in many areas of practice.
This article provides a general overview of intertrigo, and outlines the components of effective prevention strategies, and interventions to manage intertrigo and promote skin health.
What is intertrigo?
Intertrigo is a common inflammatory skin disorder that occurs because of skin-on-skin friction in the skin folds (called intertriginous regions), as a result of moisture becoming trapped owing to poor air circulation (Janniger et al, 2005; Mistiaen and van Halm-Walters, 2010; Black et al, 2011). The trapped moisture, normally caused by perspiration, in the skin folds causes the skin surfaces to ‘stick’ together, which increases friction leading to skin damage and inflammation, setting up a vicious cycle that often becomes complicated by secondary infection (Figure 2).

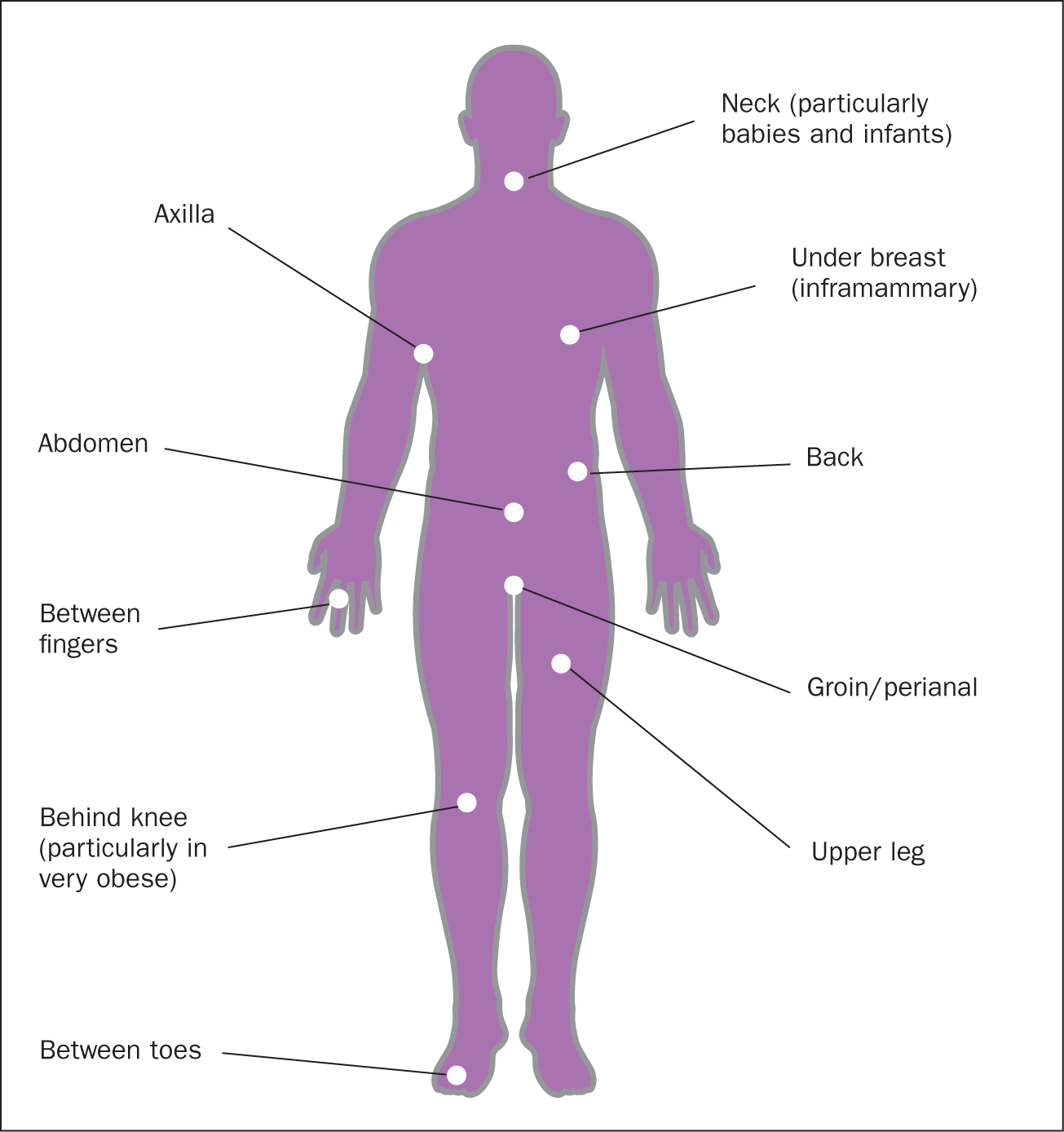
This can occur in any area of the body where two skin surfaces are in close contact with each other, such as the interdigital regions of the feet or hands, but is more common in the natural large skin folds of the body such as the axillary, inframammary, umbilical, perianal and inguinal areas (Figure 3) (Janniger et al, 2005; Black et al, 2011; Kalra et al, 2014).
Identifying and assessing intertrigo
Although intertrigo is a relatively common skin disorder, usually identified from its classic appearance and location, it can sometimes be difficult to distinguish from other dermatological conditions that may affect skin folds. To date, there is no assessment tool to assist with the identification of intertrigo or its severity.
A good patient history, focusing on previous and existing dermatological conditions, medications, allergies and sensitivities, coupled with a thorough visual inspection of the skin folds, can assist in differentiating intertrigo from less common conditions (Table 1) and is important when re-evaluating cases that have failed to respond to initial treatment.
| Condition | Characteristics |
|---|---|
| Inverse psoriasis | Occurs in axillae, behind the ears and in perianal, inframammary, genital and inguinal skin folds. Erythematous plaques with shiny/glazed appearance and less scaly than plaque psoriasis |
| Hailey-Hailey disease | Rare autosomal dominant skin disorder. Characterised by vesicles, erosions, plaques, fissures, scale and crust. Lesions symmetrically localised in intertriginous areas, such as axillae, the groin, the neck, inframammary folds, perineum and, more rarely, the vulva and mucosa |
| Hidradenitis suppurativa | Chronic inflammatory disease of skin that contains sweat glands. Characterised by nodules, abscesses, fistulas, sinus tracts and scarring in the axillae or anogenital regions |
| Baboon syndrome | Drug-related symmetric asymptomatic dermatitis with bright-red, well-demarcated lesions. Involves buttocks, intertriginous and flexor areas. Linked to some antibiotics and chemotherapy agents |
| Erythrasma | Common infection caused by Gram-positive Corynebacterium minutissimum. Occurs more frequently in men. Presents as large, brownish, well-defined, fine scaling patches in intertriginous areas |
Initially, intertrigo presents as mirror-image erythema in the skin folds, often accompanied by itching, stinging and burning. This may progress to more severe inflammation with erosion, oozing, exudation and maceration, and secondary infection is a frequent complication (Hahler, 2006). The combination of warm, moist, damaged skin provides the ideal conditions for microorganisms to breed.
In severe cases of intertrigo, infection may be more complex and involve different species (ie fungi and bacteria), including antibiotic-resistant strains (Janniger et al, 2005). Few studies have directly reported on the microbiology of intertrigo, and these have focused primarily on intertrigo in the feet, failing to separate out data from other body areas (Krishna et al, 2015; Rao et al, 2018). Interestingly, Rao et al (2018) reported multidrug resistance in 25.8% of Staphylococcus isolates and in 9.25% of Gram-negative isolates obtained from patients with intertrigo.
However, microbiological studies show that secondary fungal infections are the most common, and are usually caused by Candida albicans and dermatophytes such as Trichophyton, which often complicate interdigital intertrigo and can lead to fungal nail infections (onychomycosis). Worryingly, it has been reported that the incidence of superficial skin infections by more virulent Candida species has risen by more than 50% over the past decade (Metin et al, 2018), suggesting a need to re-examine our understanding of the microbiology of intertrigo in the large skin folds.
Candida infection is usually very itchy, with sharp margins and classic satellite lesions (National Institute for Health and Care Excellence, 2017). The depth of the skin fold should be fully examined as candidal infections are often associated with fissures, particularly in patients with existing skin disease such as psoriasis (Armstrong et al, 2016). Intertriginous infection by dermatophytes (eg Trichophyton) is more common in men, with the presence of scaling plaques, vesicles, a circular active border and central clearing being typical features, as seen in the groin in tinea cruris (‘jock itch’) or with ringworm (tinea corporis) (Ely et al, 2014). Numerous bacterial species often coexist both with each other and with Candida, including staphylococci, streptococci (especially group A beta haemolytic streptococci), Pseudomonas, Proteus mirabilis and C. minutissimum (leading to erythrasma).
In cases of inguinal and perianal intertrigo, which are often associated with incontinence, gut bacteria can also be involved, such as enterococci or Escherichia coli. The presence of ‘fiery’ red lesions, exudate and a foul odour often suggest bacterial rather than fungal infection.
If not effectively dealt with, any initial secondary infection in intertrigo can easily progress into more serious soft tissue infections such as cellulitis (particularly in patients with diabetes who have interdigital intertrigo in the feet) or even lead to sepsis (Black et al, 2011; Kalra et al, 2014). Therefore, if there is no sign of improvement after starting a management/treatment plan, or if the intertrigo appears to get worse, specialist advice should be sought as soon as possible.
Who is at risk of developing intertrigo?
Intertrigo can affect individuals of any age, with babies and infants being particularly prone to developing intertrigo in the neck folds, because of their short necks, flexed postures and drooling (Janniger et al, 2005). In adults, predisposing factors that increase the risk of intertrigo include obesity, hyperhidrosis (excessive sweating), diabetes mellitus, urinary and/or faecal incontinence, poor hygiene and being immunocompromised (eg because of HIV infection, chemotherapy or systemic steroids).
Wearing tight, restrictive clothing can contribute, particularly that made of synthetic materials, and toe web intertrigo may be associated with closed-toe or tight-fitting shoes and commonly affects people participating in athletic, occupational or recreational activities.
In patients with diabetes, particularly those with type 2 diabetes, the skin surface pH has been found to be higher, particularly in the skin folds susceptible to intertrigo, which favours the growth of pathogenic microbes (Ali and Yosipovitch, 2013; Rippke et al, 2018).
In obese individuals, several factors increase the likelihood of intertrigo developing. First, the skin folds are more pronounced, and the skin barrier function is impaired (Yosipovitch et al, 2007) favouring the development of intertrigo under the abdominal or pubic panniculi in particular. Second, the associated problems of increased sweating and reduced dexterity can make it difficult to ensure these areas are kept clean and dry.
The link between obesity and intertrigo is well established, and there is a direct relationship between the degree of obesity and the incidence of intertrigo (Waldman and Kettler, 2016; Shareef et al, 2018). This is partly because of the disruption in skin barrier function linked to obesity (Mori et al, 2017).
The rise in post-bariatric patients (morbidly obese patients who have achieved significant weight loss) means there is a newer group with a high predisposition to developing intertrigo. Many of these patients are left with significant amounts of excess skin and extreme skin folds within which intertrigo often develops (Acarturk et al, 2004).
How common is intertrigo?
Accurate incidence and prevalence data for intertrigo remains elusive, certainly in the UK, and the extent of the problem in the general population is not known. This is partly because of a previous lack of standard definitions and the use of different terms. The inclusion of intertrigo in the ICD-11 should help as it provides a simple definition to improve the quality of reporting in future (WHO, 2019).
The often cited incidence and prevalence figures for intertrigo come from a European systematic review of ITD in adults that estimated there was a prevalence of 6% in hospital patients, 17% in nursing home residents and 20% in those receiving home care (Mistiaen and van Halm-Walters, 2010). Similar figures (16.1%) have been reported by Hahnel et al (2017) and Gabriel et al (2019) in Germany, while Özer et al (2019) reported a prevalence of 5.3% in Turkish nursing home residents. In contrast, Valls-Matarín et al (2017) reported an intertrigo incidence of 15.9% in a Spanish intensive care unit, and Emre et al (2013) a prevalence of 28.9% in a Turkish intensive care unit.
In the USA, Arnold-Long and Johnson (2019) assessed the prevalence and incidence of IAD and intertrigo over a three-year period in an acute care community hospital. Compared to the European studies, the prevalence of intertrigo was found to be much higher, with a mean prevalence on admission over the 3-year period of 40%. Interestingly, they also report a significant reduction in the prevalence of hospital-acquired intertrigo during this period, which they attribute to the introduction of a specific skin fold management protocol and associated staff education.
Another US study collated data on all forms of MASD over one year in an acute teaching hospital (Werth and Justice, 2019). It found an overall prevalence of MASD of 4.34%, with intertrigo being the most prevalent form of MASD seen at 2.66%.
Recently, Kottner et al (2020) published a secondary data analysis of four annual multicentre prevalence studies from the Netherlands. In total, data from 40 340 patients were included, covering those in care homes and hospitals as well as people receiving home care. Intertrigo prevalences of 2%, 7% and 10% were reported for hospitals, care homes and home care respectively. Worryingly, this suggests there is a strong association between the presence of intertrigo and the degree of dependency on care staff to maintain hygiene needs.
It will be interesting to see if the quality of data for the UK improves now MASD is included in the pressure ulcer reporting framework (NHS Improvement, 2018).
Prevention and management of intertrigo
Optimal prevention should begin with educating patients on what intertrigo is, what to look for and how to care for their skin folds, particularly for those at high risk.
Specific advice on skin fold care should include minimising skin-on-skin friction, reducing moisture in and around the skin folds, and keeping high-risk areas clean and dry. Where possible, predisposing factors should be addressed, such as weight reduction in obesity, maintaining good glycaemic control in diabetes and incontinence management.
Patients should be advised to wear loose, light clothing made from absorbent natural fabrics (eg cotton) or athletic clothing designed to wick perspiration away from the skin, and to avoid synthetic fabrics. Attention should be paid to ensuring skin folds are kept clean and dry, with the adoption of a structured skin care regimen as would be used for any form of moisture-associated skin damage.
Ideally, cleansing should be with a no-rinse, pH-balanced cleanser and avoid the use of alkaline soaps if possible. Emollient-based soap substitutes may be used as an alternative to gently cleanse the skin and skin folds (Metin et al, 2018). Importantly, however the skin is cleansed, care should be taken to ensure the skin folds are thoroughly dried, without causing excessive friction.
The use of skin barrier products to protect the skin from moisture and reduce friction are recommended, but these are often difficult for patients to apply and remove effectively themselves. To date, there is insufficient evidence to guide choice of product. Blackett et al (2011) discussed some of the methods patients might use to address the problem themselves, such as placing cloth, tissue, pads and gauze within skin folds, as well as using talc and/or other powders to absorb moisture. There is no evidence that any of these are effective and, indeed, they may be detrimental, as any moisture absorption will be limited, and they may further irritate the skin as well as provide a medium for microbial growth (Sibbald et al, 2013; Kalra et al, 2014; Cunliffe, 2018).
Based on expert consensus opinion (Sibbald et al, 2013), moisture-wicking textiles specifically designed for skin-fold management are now recommended for the prevention of intertrigo in high-risk patients. These have been used in North America for more than a decade and are now available in the UK. The textile is designed to lie in the skin folds, wick moisture away and allow it to evaporate, keeping the skin fold dry. They also reduce skin-on-skin friction and contain broad-spectrum antimicrobial silver (Kennedy-Evans et al, 2007; Sibbald et al, 2013; Cunliffe, 2018).
Uncomplicated intertrigo should be managed by following the measures outlined above. However, intertrigo complicated by secondary infection will not resolve unless the infection is treated. In all cases, treatment should be based on local antimicrobial policies. Recommendations for treating candidal infections include the use of topical antifungal preparations, usually in an emollient base (eg clotrimazole and miconazole), and consideration of systemic therapy if infection is severe (Janniger et al, 2005; Kalra et al, 2014; Metin et al, 2018).
In the UK, topical miconazole is recommended as a firstline treatment as it has some Gram-positive bacteriostatic action (Cunliffe, 2018). Topical antifungal agents generally need to be used for at least two weeks in intertrigo, adding to the burden on patients and care givers (Hay, 2018). The addition of low-potency steroids or the use of a combination preparation containing an antifungal and steroid has been recommended, particularly where there is severe inflammation accompanied by pruritus (Kalra et al, 2014; Cunliffe, 2018). However, Mistiaen and van Halm-Walters (2010) found that there was limited evidence to show systemic therapy was any better than topical or that corticosteroids were any better than antifungals in reducing inflammation in intertrigo.
Secondary bacterial infection may be treated by topical or systemic antimicrobials such as topical or oral erythromycin for erythrasma (Kalra et al, 2014). However, in the current climate of antimicrobial resistance, antibiotic use should be judicious and based on local antimicrobial prescribing policies.
Based on several case study reports, moisture-wicking textiles containing silver also appear to have a role in treating complicated intertrigo. A case series involving two long-term care centres in the USA demonstrated relief of symptoms within a 5-day period in patients with refractory intertrigo (Kennedy-Evans et al, 2007; Sibbald et al, 2013). More recently, case reports from European centres have reported complete resolution of intertrigo after a moisture-wicking textile was used (Andersen and Gotfredsen, 2019; Brereton, 2019).
Interventions for the prevention and management of intertrigo are summarised in Table 2.
| Skin condition | Interventions |
|---|---|
| General skin fold management and prevention of intertrigo |
|
|
|
|
| Mild intertrigo, uncomplicated by secondary infection |
|
|
|
|
|
|
|
|
|
|
| Intertrigo complicated by secondary fungal infection |
|
|
|
Other treatments
There is some evidence that selected patients with recurrent intertrigo may benefit from surgical intervention, such as women with macromastia (Mistiaen and van Halm-Walters, 2010) with Nguyen et al (2013) reporting a long-term improvement in intertrigo following breast reduction surgery of 88.6%.
Previously obese patients who have lost significant amounts of body weight (post-bariatric patients) are a new, growing group who may benefit from body contouring surgery to remove the excess skin they are usually left with, which often increases the risk of intertrigo developing. Various surgical techniques are available, such as abdominoplasty, brachioplasty and medial thigh lift.
While direct evidence for whether surgery reduces the incidence of intertrigo in this group is lacking, a systematic review by Toma et al (2018) showed body contouring surgery to remove excess skin after major weight loss has a significant positive effect on body image and overall quality of life.
Conclusion
Intertrigo is a common form of MASD encountered in many different patient groups and care settings. Moisture, normally from perspiration, becomes trapped in skin folds causing the skin surfaces to ‘stick’ together, leading to friction and damage.
Unlike other forms of MASD, intertrigo presents numerous clinical challenges and lacks a robust evidence base to guide practice. Although there is the need for more research in this area, there is a growing body of expert clinical consensus to guide practice, and general principles for the prevention and management of MASD can be used.
Careful assessment and identification of risk factors can help distinguish intertrigo from less common skin disorders and enable appropriate interventions to be implemented. These should begin with the adoption of a structured skin care regimen to cleanse and protect the skin. This should be followed by methods to control the source of the excessive moisture, if possible, to keep the skin dry by wicking away excessive moisture and treating any secondary infection.
The evidence demonstrates that investment in the development and adoption of clear skin care and skin fold management protocols based on these principles can lead to improvements in the patient experience, clinical outcomes and quality of life.