
The use of indwelling urethral or suprapubic catheters is common and is not restricted to the hospital setting (NHS Improvement, 2018). The Health Protection Agency (HPA) (2012) suggested that catheters are frequently used in the community setting and usually left in place for at least 28 days. Gage et al (2016) estimated that in the UK more than 90 000 people have a long-term catheter. In many cases, patients have a catheter for neurological reasons (62.9%). According to the Chief Medical Officer, ‘urinary catheters are used relatively frequently in older patients as part of care in the management of conditions such as dementia, prostate disease and incontinence from other causes' (Department of Health (DH), 2013). However, long-term catheterisation is seldom trouble free, with most patients experiencing recurring problems, such as blockage of urinary flow and catheter-associated urinary tract infection (CAUTI) (Maeda et al, 2013; Wilde et al, 2013; Tay et al, 2016).
In England, CAUTI accounts for about 43-56% of all UTIs (HPA, 2012a; Loveday et al, 2014) and is a common nosocomial infection, second to respiratory tract infection; in older patients it comprises 17.2% of the total (HPA, 2012; Loveday et al, 2014). The DH (2013) reported that CAUTI is associated with extended hospitalisation, readmission and increased mortality. This is due to bacteriuria, which is found in one-third of patients after 2–10 days from catheterisation (Loveday et al, 2014) and in all patients catheterised for more than 30 days, even when an aseptic, closed catheter drainage system is maintained (European Association of Urology, 2015). The presence of bacteriuria and bacteria in the urine is asymptomatic in most patients, but about 24% of cases will develop symptoms of CAUTI, leading to serious complications in 3.6% of patients, who develop life-threatening infections with the mortality rate of 10-33% (Shuman and Chenoweth, 2010; Chang et al, 2011; National Institute for Health and Care Excellence, 2012). Furthermore, CAUTI can lead to delirium, increased risk of falls (Hazelett et al, 2006) and the development of antimicrobial resistance due to increased use of antibiotics to treat CAUTI (DH, 2013; Centers for Disease Control and Prevention, 2018).
Catheter-related problems contribute to the financial burden on the NHS due to unscheduled visits to emergency services, hospitalisation or delayed discharge from hospital, antimicrobial treatment and staff resources (Loveday et al, 2014; Tay et al, 2016). It has been estimated that treatment of CAUTI accounts for £99 million per year (about £1968 per episode) (Loveday et al, 2014). Tay et al (2016) suggested that 75% of patients who attended the ED with catheter problems could have been treated at home. This highlights the need to improve the quality of care and move towards a model based in the home to enable patients to self manage their catheter and reduce the risk of CAUTI.
Literature review
Aims
The review aimed to identify ways that nursing staff can support catheterised patients to maintain effective catheter care in order to reduce the risk of CAUTI. A critical integrative literature review was chosen to facilitate investigation of the topic from objective and subjective perspective by incorporating qualitative, quantitative and mixed method studies.
The inclusion criteria were as follows.
The exclusion criteria were:
Search strategy
Four databases were used to obtain relevant studies: the Cochrane Library, the British Nursing Database, CINAHL and PubMed. The following keywords were selected: support; long-term catheter; self-management; catheter-associated urinary tract infection. The Boolean operators (AND, OR and NOT) and truncation (using ‘*’ to ensure that all possible variations of the key terms were found) were used to search for articles using the search terms: support* OR help* OR train* OR educat* OR teach* OR inform* OR aware* OR knowledge AND long-term catheter* OR urinary catheter* OR urethral catheter* OR indwelling catheter* AND self-manag* OR self-care OR self-efficacy OR efficacy AND CAUTI OR infect* OR UTI OR bacteriuria.
A total of 139 articles were identified (Figure 1), with 94 remaining after removal of duplicates. A further 57 primary studies failed to meet the inclusion criteria, so they were excluded, leaving 37 articles, of which 25 were excluded for not meeting the inclusion criteria. The remaining 12 manuscripts were critically appraised for robustness, validity and quality using selected critiquing frameworks.
Quality appraisal
The following frameworks were used to critique the articles:
Data extraction
On the basis of Whittemore and Knafl's (2005) recommendation, data from primary sources were divided into logical subgroups according to type of evidence and then sequentially analysed. For each subgroup, relevant data were extracted from primary sources and compiled into a matrix by:
This was the starting point for the interpretation process (Table 1, see end of article). Each paper was individually read and reread to achieve further understanding of the findings. Data from individual sources were subsequently combined into a display by subgroups to determine patterns and relationships. The data were then compared to identify emerging themes based on any similarities and differences. The developed themes were then grouped into hierarchical subthemes using force-field analysis (Figure 2). Visualising and comparing the data in this way provided clarity for early and empirical interpretation.
| Author, year, country | Title | Aim | Study design | Sample size | Key findings |
|---|---|---|---|---|---|
| 1 Fowler et al (2014), UK | Living with a long-term, indwelling catheter. Catheter users' experience | Interpret the experiences and priorities for LTC users |
|
Purposive sampling strategy, including 27 adults aged 22–96 years old with long-term catheterisation |
|
| 2 Godfrey, (2008), UK | Living with a long-term urinary catheter: older people's experience | Understand older people's experiences related to LTC and to develop theory grounded in their realities |
|
Purposive sampling strategy; 13 participants aged >60 years old, using urinary catheters for >3 months |
|
| 3 De Jaeger et al (2017), UK | A qualitative study exploring the value of catheter passport | Investigate an effect of a patient-held catheter passport on patients leaving the hospital with IUC and to explore the experiences of hospital nurses who discharge the patients and community nurses who provide their ongoing care |
|
Purposive sampling strategy; interviews with 9 adult patients, 5 community nurses and 6 hospital nurses; in addition, 38 hospital nurses completed a questionnaire |
|
| 4 Prinjha et al (2016), UK | Exploring the information needs of people living with a long-term indwelling urinary catheter: a qualitative study | Explore the information needs of people with LTC, how their needs can be met and the consequences of inadequate information |
|
A maximum variation sample; 36 participants, age 22–96 years, living in the community with LTC | Participants felt they were told very little about the catheter when it was first fitted; they need more technical information about it and how to prevent complications, and more information to help prevent catheter-related physical problems |
| 5 Kralik et al (2007), Australia | Managing the self: living with an indwelling urinary catheter | Explore perspectives of living with a urinary catheter; raise awareness of the experiences of patients with LTC to inform community nursing practice |
|
Purposive sample; 21 participants aged 24–82 years living with LTC | The biggest concern for participants was the risk of infection, making them aware of the importance of self-care and taking control |
| 6 Wilde and Brasch (2008a), USA | An intervention to teach self-monitoring of urine flow in long-term catheter users | Assess participants' perceived value of carried out intervention of urine-flow self-monitoring to reduce episodes of CAUTI |
|
Purposive sample; 11 participants | The intervention was perceived easy to use; participants benefited as it helped them understand the importance of urine flow and increased awareness of their own patterns |
| 7 Lee et al (2015), Taiwan | A nurse-family partnership intervention to increase the self-efficacy of family caregivers and reduce catheter-associated urinary tract infection in catheterised patients | Evaluate whether a nurse-family partnership model will support family caregivers' self-efficacy and result in protecting patients against CAUTI |
|
Purposive sample: 61 participants (30 in the experimental group and 31 controls); patients without symptoms of CAUTI catheterised for >5 days | Incidence of CAUTI was lower among the test group (20%) than the controls (38.8%) |
| 8 Khan et al. (2010), UK | Strategy to control catheter encrustation with citrated drinks: a randomised crossover study | Determine whether the activity of urease-producing bacteria can be controlled by increasing the fluid intake with citrated drinks |
|
21 participants (mean age 63 years) with LTC | The simple addition of citrated drinks to patients' diet may decrease the risk of encrustation hence other related catheter problems such as CAUTI |
| 9 Wilde et al (2016), USA | Testing a model of self-managing of fluid intake in community-residing long-term urinary catheter users | Determine whether catheterised patients' self-management practices concentrated on fluid intake would be linked with self-efficacy toward decreasing CAUTI and/or catheter blockage |
|
180 participants, aged 19–95 years, with LTC | Fluid intake self-management was not associated with either frequency, or presence or absence of CAUTI. Fluid intake self-management predicted less frequency of catheter blockage but did not predict presence or absence of blockage |
| 10 Wilde et al (2015), USA | Self-management intervention for long-term indwelling urinary catheter users | Examine the effectiveness of a self-management intervention in preventing adverse outcomes (CAUTI, blockage, and accidental dislodgement). Determine whether teaching catheter users self-management skills could decrease short-term, catheter-related problems and whether improvements could be sustained over 12 months |
|
220 participants (mean age 61 years) with LTC | CAUTI rate of 6.93/1000 catheter days decreased to 4.89 (a 29% relative reduction) over a full 12 months |
| 11 Wilde and Brasch (2008), USA | A pilot study of self-monitoring urine flow in people with long-term urinary catheters | Evaluate the feasibility of the intervention of self-monitoring of urine flow in catheterised patients; assess the effect of intervention on CAUTI, blockage and participants' quality of life; evaluate formulated instruments to measure awareness, self-monitoring, and self-management of urine flow |
|
11 participants aged 28–70 years, with LTC | Cases of UTI reduced by about 50% |
| 12 Mackay et al (2017), UK | Living with an indwelling urethral catheter in a community setting: exploring triggers for unscheduled community ‘out-of-hours’ visits | The qualitative aim of the study was to investigate the experiences of catheterised patients in the community and those caring for them. The quantitative objective was IUC-related consequences on a community nursing unscheduled service |
|
Purposive sample strategy: 15 participants: 6 catheterised patients aged 68–86 years; 2 community nurses; 3 augmented home carers; 2 relative carers; 1 healthcare assistant | The quantitative data revealed that 20% of unscheduled visits by community nurses were related to urethral catheters. |
CAUTI = catheter-associated urinary tract infection
LTC = long-term catheterisation
IUC = intermittent urinary catheter
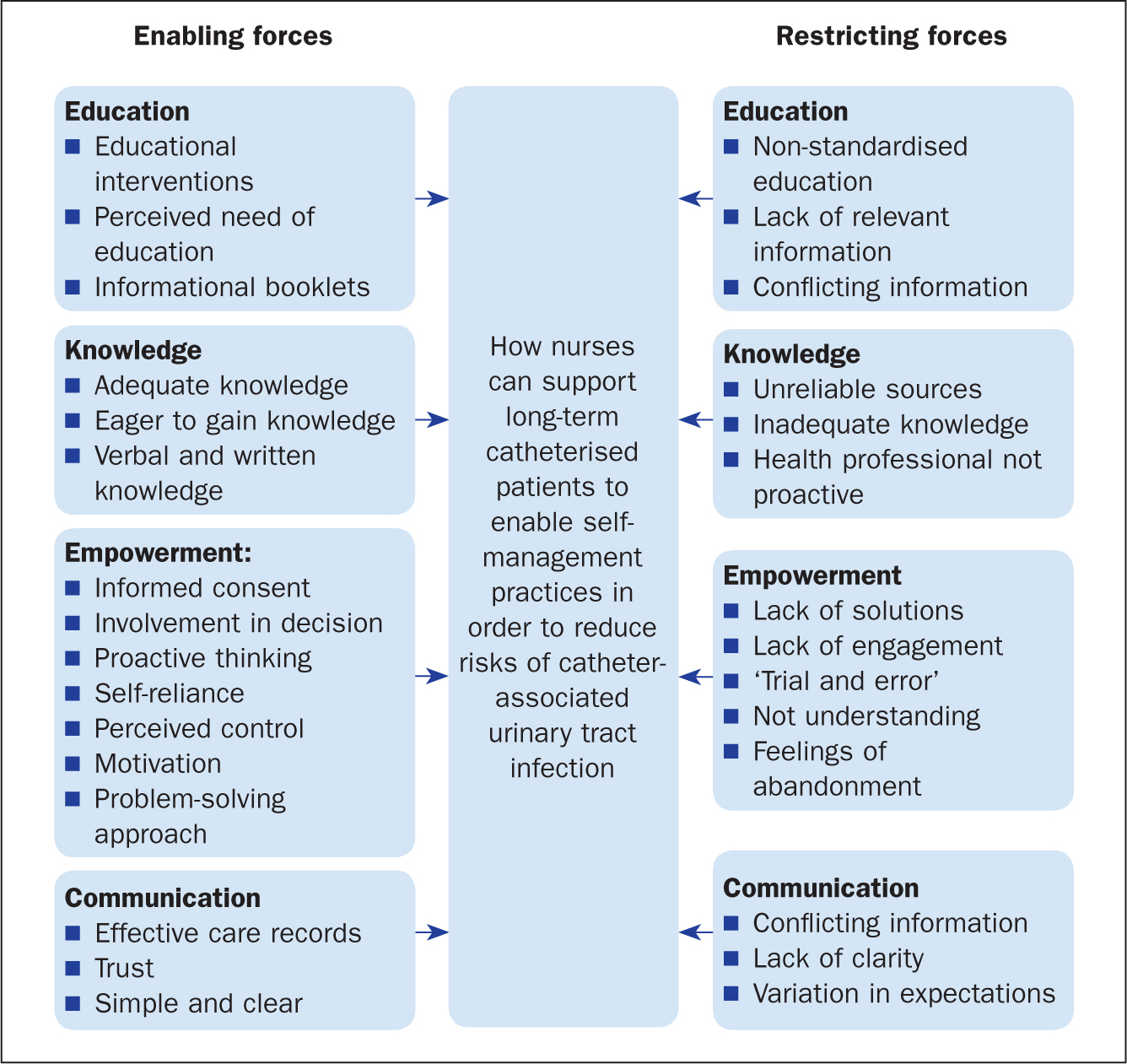
Emerging themes
The four themes identified within the selected articles were (Figure 2):
Education
The studies by Wilde and Brasch (2008), Wilde et al (2015), Lee at al (2016) and De Jaeger (2017) agreed that both informational booklets and educational interventions advising what patients should look for when self-monitoring urine flow or how much they should drink could reduce the risk of CAUTI in patients. The evidence showed that being aware of urine flow, its smell and colour, and ensuring a good fluid intake, will alert patients to early signs of infection and blockage and enhance self-management practices, helping avoid problems in future (Khan et al, 2010; Wilde et al, 2015; Lee et al, 2016).
Wilde and Brasch (2008) created educational materials to facilitate the learning of how to be mindful of urine flow and found that a 6-month intervention reduced the incidence of CAUTI by 50% and increased patients' self-management habits: this included patients noticing the colour of their urine on a routine basis, as well as increasing their fluid intake. According to the model of self-management of fluid intake created by Wilde et al (2016), confidence about urine intake led to positive self-management behaviours with regard to fluid intake. This in turn was directly connected to a reduction in the rate of catheter blockage and, indirectly, to fewer CAUTI incidents. The effect was the minimisation of CAUTI incidence by 29%. Even though the results were statistically not compelling, the decrease in CAUTI rate was clinically relevant, because it resulted in a 14.1% reduction in UTI-related hospital admissions in 14 months (Wilde et al, 2015; Wilde et al, 2016).
A similar educational process was undertaken by Lee et al (2016), who focused on family-carers. Despite the fact that the 20% reduction in CAUTI was not statistically significant, the study showed the importance of nurse–carer interaction in managing indwelling urinary catheters. Interestingly, according to Fowler et al (2014), patients with spinal-cord injury, who benefitted from support and education from a spinal-cord centre, seemed more self-reliant and knowledgeable about the catheter. In contrast, Mackay et al (2017) discovered that there was no standardised approach to the way in which patients and their carers were offered relevant information or educational materials regarding their catheter and thus frustration and confusion developed about conflicting or superficial guidance received from healthcare practitioners.
Knowledge
Patients' knowledge is closely connected with education, which contributed to the findings of Godfrey (2008) and Prinjha et al (2015). Patients in these two studies developed proficiency in recognising the signs and symptoms of infection. Researchers emphasised the dilemma of antibiotic treatment versus the risk of developing resistance (Godfrey, 2008; Fowler et al, 2014). Prinjha et al (2015) found that patients with catheters desired to become knowledgeable about how to avoid infections, and asked for information on hygiene, fluid intake, kidney physiology, follow-up appointments with the urologist, and wanted to know about the long-term effects of intermittent use of antibiotics (Prinjha et al, 2015). However, Mackay et al (2017) reported that nurses provided guidance and information reactively and superficially. Although the patients had positive motivational intentions, some nurses' inability to quantify ‘drink plenty’ or ‘just make sure it is kept clean’ resulted in advice that was often vaguely phrased and could thus inadvertently have led to detrimental effects. Some patients had taken in an average of 8000 ml of fluids a day, unaware of the fact that this quantity was excessive (Wilde et al, 2015)
Without timely information, catheter care was a process of ‘trial and error’ or patients sought information from unvalidated online sources. Some patients emptied their catheter bags at the first signs of urine and restricted their liquid intake when travelling long distances. In addition, prime reasons for infection included the use of inappropriate cleaning methods to prevent blockages and a lack of care to the bladder neck by using an unsecured bag (Prinjha et al, 2015). Mackay et al (2017) reported that patients often forgot or misinterpreted advice; however, in another study this was simplified by the use of a patient catheter passport (Jaeger et al, 2017), which offered reassurance to patients following discharge.
Some patients preferred face-to-face interaction with health professionals to help them understand catheter management involving, for example, step-by-step instructions and troubleshooting guidance, as well as the use of graphics to aid understanding (De Jaeger et al, 2017; Mackay et al, 2017). These results show that nurses can support catheterised patients through education, disseminating knowledge about CAUTI.
Empowerment
Kralik et al (2007) highlighted the need for patients to be involved in decisions pertaining to catheter care, to enable them to accept and recognise the cues of catheter malfunction. Patients benefited from the control gained from monitoring urine flow themselves and checking for signs of blockage or infection, which fostered confidence in their own ability to take decisions (Wilde and Brasch, 2008; Lhussier et al, 2015). Godfrey (2008) suggested that patients who did not understand the need for the catheter were less involved in their care and tended to feel discouraged. Moreover, limited consultation resulted in patients feeling dissatisfaction and that they had been coerced into accepting a catheter. Some reported feeling abandoned rather than empowered (Mackay et al, 2017): for example, some nurses simply told them that these problems just happen, without offering a solution or any help.
In De Jaeger et al's (2017) study, some nurse participants hoped that a catheter passport would bolster patients' ownership of their catheter, making them feel in control and confident. Interestingly, patients in this study used the passport as a form of reassurance and, in particular, used it to educate themselves on basic hygiene. Other patients used the passports proactively, finding answers and options to problems such as bag positioning and drainage.
Communication
Communication was a key topic in the studies reviewed. This referred to many aspects of communication, including whether the information that was shared between carers, nurses and patients was useful, adequate, relevant, fragmented or timely. In Mackay et al's study (2017), patients and relatives or carers agreed that they had received conflicting information from health professionals. This was a decisive factor in causing confusion and frustration among patients and their relatives, and sometimes resulted in a dilemma about trust and reliable information. The burden of responsibility on the patient was accompanied by them feeling vulnerable in terms of their level of knowledge, and the lack of clarity about role responsibility of catheter care. There was also a lack of clarity concerning who does what, which was due to the unique nature of each patient's needs, catheter-related consequences and the ability to involve the patients in self-care (Mackay et al, 2017).
The catheter passport did bridge the communication gap between community and acute settings, and between patients and nurses (De Jaeger et al, 2017); and there was an awareness of the information gaps when patients were discharged with a catheter. The catheter passport therefore represented an up-to-date, safe record of patients' catheterisation, which could be shared across settings, communicating information about when and why a patient had been catheterised; it was simultaneously a tool to better communicate with patients, encouraging them to ask about catheter issues (De Jaeger et al, 2017).
Discussion
There is a lack of robust research to inform guidelines on catheter care and on preventing CAUTI. Many guidelines are based solely on expert opinion, rather than on methodologically robust outcomes of randomised controlled trials (Cottenden et al, 2013). It is also worth noting that nearly all the research used to underpin evidence-based practice has focused on preventing CAUTI in patients with short-term catheterisation (Pickard et al, 2012), with little research addressing the problem with long-term catheterisation (LTC). In addition, most of the research into possible interventions to reduce the incidence of CAUTI was hospital based and nurse focused, with none being patient led, based on the studies reviewed (Jenkinson, 2005; Fuchs et al, 2011; Andreessen et al, 2012). This may have occurred because CAUTI was seen as a nosocomial infection, and most national initiatives have been associated with reducing CAUTI rate in acute settings, by introducing ‘bladder bundles’ and educating nurses about preventive measures, such as early catheter removal, aseptic technique and maintaining a closed drainage system (Saint et al, 2009; Meddings et al, 2013).
Although multiple strategies are required to reduce the incidence of CAUTI, analysis of the findings of these studies strongly indicates that patients want to become more empowered. Therefore, nurses' support in improving their knowledge, skills and confidence is a prerequisite to reducing the risk of CAUTI and successful catheter management. These findings support those of Orem (2001), who showed that improving patients' knowledge about their condition enhances the ability to self-care. Nurses' role in assessing patients' needs and ensuring ongoing education and support are invaluable. LTC inevitably requires lifestyle changes and affects the behavioural, cognitive and emotional responses needed to maintain a good quality of life.
Living with or offering support and care for people with LTC is a complex experience. However, because the problems face by people living with LTC on a regular and recurrent basis are not classed as life threatening, they tend to get forgotten (Mackay et al, 2015). Nonetheless, infections were repeatedly cited as one of the issues experienced by patients and had a great effect on their quality of life (Kralik et al, 2007; Godfrey, 2008; Prinjha et al, 2015). Patients felt insufficiently prepared to manage LTC when something went wrong, and usually learnt through experience (Fowler et al, 2014). This reality limits patients' ability to self-manage and contradicts the recommendations, which encourages health professionals to provide support and information for patients with LTC (Wound, Ostomy and Continence Nurses Society, 2016).
While the studies that were included in this literature review provide examples of educational interventions and promote these as one solution—for example, teaching patients how to self-monitor urine or complete fluid input/output charts—the studies did not provide information about the feasibility and the cost-effectiveness of these programmes in the UK (Wilde and Brasch 2008; Lee et al, 2014; Wilde et al, 2015). Robinson (2004) prompted nurses to accept training and knowledge limitation regarding catheter problems, because managing LTC is a complex process led by the culture where care is given, local service provision, health policies and available resources that are normally finance-dependent (McEvoy 2014).
These policies determine that people living with a chronic illness should become more responsible for self-management of their condition. However, knowledge alone—which should start with nurses providing patients with adequate information—is insufficient and cannot enable optimal self-management. Patients also need to learn how to express their needs, find and analyse health information from a variety of sources, and have wider knowledge about the available treatments and the role of health professionals.
Suboptimal health literacy will hinder many patients from having an active role in managing their condition, even if they desire to do so (Coates, 2017). Thus, advocating catheter self-care is not only about educating the patients about their condition or providing relevant information, and the correct response to take, it is also about positive interactions. Clear communication between health professionals and patients can help develop confidence and motivate patients to use their own skills to be effective in taking control of their situation (De Jaeger, 2011). Patients view catheterisation as a very personal matter, and may associate it with sexuality, body image and desirability. It is therefore important that nurses work towards developing a transparent, open and trustworthy relationship to encourage patients to be honest about their catheter self-care to reduce the risk of CAUTI (Box 1).
Limitations of review
It is important to acknowledge the limitations of this analysis. In relation to the data reviewed, the inclusion and exclusion criteria placed limitations on the types of studies retrieved and considered appropriate for this literature review, which may have led to some relevant studies being overlooked; it must also be acknowledged that the findings within the studies selected may have been influenced by publication bias.
All the studies included in the review were published in English, so that pertinent studies in other languages may have been overlooked. Findings using thematic analysis are also prone to interpretation—and this is also a limitation of the analysis presented in this article.
Conclusion
Analysis of the findings shows that patients with catheters would value practical information and education on the management of LTC and CAUTI. The evidence showed that extensive written, verbal and visual information about the catheter itself and living with it would be advisable (De Jaeger et al, 2017). Furthermore, written advice provided on discharge, including a catheter passport, would increase patients' awareness of catheter issues and support problem solving (Wilde and Brasch 2008; De Jaeger et al, 2017). These simple changes can help detect and enable swift treatment of any early signs of infection.
In addition, the decision making process when decided whether to have a catheter does require a collaborative relationship between the patient and health professionals to enhance self-care and problem-solving strategies.