

More than 300 people joined the fifth annual webinar discussing the results of research into occupational exposure of nurses to hazardous drugs and the protective role of closed system transfer devices (CSTDs).
The webinar, held on 18 April 2024, was organised by Aesculap Academia, the educational arm of B Braun Medical. Earlier webinars in this series have been reported in previous British Journal of Nursing oncology supplements (Clark, 2021a; 2021b; 2022; 2023).
The programme included research findings on occupational exposure to cytotoxic agents, a case study on the implementation of closed systems for the administration of systemic anti-cancer therapy (SACT), an update on the PeCan study and tips on preparing a business case for closed systems.
Co-chair Naomi Clatworthy, acute oncology nurse consultant at Royal Devon University Healthcare NHS Foundation Trust, launched the webinar with an audience poll that showed that 63% of respondents were ‘very concerned’ about the health effects of hazardous drugs. Co-chair Mark Foulkes, nurse consultant and Macmillan lead at the Royal Berkshire Hospital NHS Foundation Trust, said that this ‘shows the level of worry’ among nurses.
Exposure and health effects of hazardous drugs
Concerns about the dangers of SACT began to emerge in the 1970s when second malignancies were first reported in cancer patients treated with alkylating agents, explained Dr Melissa McDiarmid, professor of medicine and epidemiology at the University of Maryland School of Medicine. This rapidly led concerns that healthcare workers might also be at risk.
A study demonstrated that the mutagenicity of nurses' urine steadily increased during the working week and then fell again at weekends (Falck et al, 1979).
‘This was the first biologic documentation that there was a concern for nurses handling [SACT] drugs,’ said McDiarmid. At that time, gloves were not worn when injections were being prepared, she acknowledged.
These findings were the initial driver for safe handling guidance, which came first from the American Society of Health-System Pharmacists, followed by the Oncology Nursing Society and the Occupational Safety and Health Administration (both in the US).
About 18 of the drugs commonly used for cancer treatment are classified as group 1 human carcinogens by the International Agency for Research on Cancer, the cancer arm of the World Health Organization. Another 11 out of 58 are classified as ‘probable human carcinogens’ (group 2A) and a further 13 of 249 are ‘possible human carcinogens’ (group 2B).
In addition, many of these drugs are well documented as reproductive and developmental toxicants in both women and men. Ganciclovir is an example of a male-mediated toxicant. The drugs are associated with biologically plausible health effects (e.g. myelodysplastic syndrome and secondary malignancies) in exposed populations, McDiarmid stated.
Recent guidance
A number of guidance documents have recently been published, including the European Trade Union Institute's (2022) list of hazardous medicinal products, the ISOPP Standards for the Safe Handling of Cytotoxics (ISOPP, 2022) and European Commission (2023) guidance. Furthermore, the European Parliament's recent Stop Cancer at Work initiative has increased the emphasis on this topic.
These are good developments which probably mean that we will need to ‘step up our resolve and get a little better at the safety aspects of handling these life-saving drugs in the care of our patients', noted McDiarmid.
Exposure to systemic anti-cancer therapy drugs
Studies have repeatedly shown surface contamination in areas where SACT drugs are compounded or administered (European Biosafety Network, 2018). Even if SACT drugs are compounded in isolators (as is common in the UK and Europe), contamination is contained but the finished products often have cytotoxic contamination on their outer surfaces (e.g. the surfaces of infusion bags) and this can be spread elsewhere when they are transported to wards and administered to patients (Crauste-Manciet et al, 2005).
Every study carried out on surface contamination has shown the spread of at least one hazardous drug, she said. ‘So, for every study that's been done, at least one drug has been found to be positive,’ she said.
Moreover, studies have showed the presence of such drugs in the urine of healthcare workers, confirming that they had been exposed (Villa et al, 2021; Leso et al, 2022). A meta-analysis of studies looking at biomarkers of genotoxicity in health practitioners (Roussel et al, 2019) showed there was ‘a significant association between occupational exposure to antineoplastics and increases in chromosomal aberrations’, said McDiarmid.
Finally, a study led by McDiarmid showed that healthcare staff who regularly handled alkylating agents developed abnormalities of chromosomes 5 and 7 – those targeted by alkylating agents (McDiarmid et al, 2010). This she described as the ‘smoking gun’.
There is also evidence of reproductive risk – ‘spontaneous abortion is been quite well documented in nurses and pharmacists exposed to antineoplastic drugs’, she said (Lawson et al 2012).
Immune modulators
Although immune modulators were previously thought not to be hazardous, second malignancies have now been reported with, for example, adalimumab and tacrolimus. Immunomodulators have toxic effects and need to be treated with respect, she emphasised. In the US, anti-TNF agents now have a black box warning on the package insert, indicating the risks of serious infections and malignancies.
In addition, a long list of monoclonal antibodies (mAbs) - ‘the-abs and -ibs’ as McDiarmid called them – is included on the National Institute for Occupational Safety and Health's (2020) list of hazardous drugs. Many of these are targeted anti-cancer drugs and most are toxic to reproduction and should be avoided in women who are pregnant or breastfeeding, she stressed.
Managing the risk
Managing the risks effectively depends on using a hierarchy of controls. Level 1 concerns engineering controls, such as safety cabinets and containment devices. Level 2 is about administrative approaches, and includes safe work practices and training. Level 3 is personal protective equipment (PPE) (Health and Safety Executive, 2024).
Hazardous drugs exposure registry
At the University of Maryland, work to establish a national exposure registry on a web-based platform is in progress. Data are now being collected on colleagues who handle drugs on both their work practices and their cancers. Reproductive experiences are also logged and self-reported cancers are validated using the state cancer registry. ‘We think this will be a quite robust way to look at this problem,’ said McDiarmid.
In summary, McDiarmid said that biologically important exposure to genotoxic drugs is occurring. It is resulting in dose-dependent increases in chromosomal aberrations and reproductive abnormalities. Appropriate provisions for risk management and surveillance of staff need to be in place.
Improving safety and efficiency with closed systems and advanced infusion pumps
An audience poll showed that 82% of audience members experienced intravenous therapy delays because pumps had to be reprogrammed to clear the residual volume in infusion bag or because of air in the line.
Careful documentation of the resources used and the time required enabled Sarah Wellington, lead chemotherapy nurse at University Hospitals, Plymouth NHS Trust, to show that implementing closed systems for SACT administration saved both time and money. It improved overall workflow, saving working time for nurses and chair time for patients.
The 27-chair oncology day unit was equipped with old, inefficient infusion pumps. Over-filled SACT bags required frequent reprogramming of the infusion pumps to infuse the whole drug volume (ie reprogramming the Volume to Be Infused (VTBI)). But over-estimations of VTBI often led to air entering the line. Opening the system to remove the air created infection and spillage risks that delayed treatment and reduced efficiency, she explained. This cumbersome operation also generated a large amount of cytotoxic waste, she added.
A time and motion study was undertaken to identify inefficiencies with the existing workflow processes. The old system used Luer-based devices for SACT administration. It required multiple connections and disconnections for priming the giving set, administration of the chemotherapy and then flushing the giving set. Pumps often had to be reprogrammed to finish the SACT bags and there were risks of air entering the line and droplets of drug solution escaping. In addition, port disinfection was time-consuming. A multi-SACT treatment could need 5-10 changes, with a new bag spike for each treatment, said Wellington.
Closed systems were implemented including: new pumps (Infusomat Spaceplus SMART infusion pumps); Cyto-Set AirStop giving sets for use with SACT bags; and Chemfort CSTDs for use with SACT syringes (Figure 1).
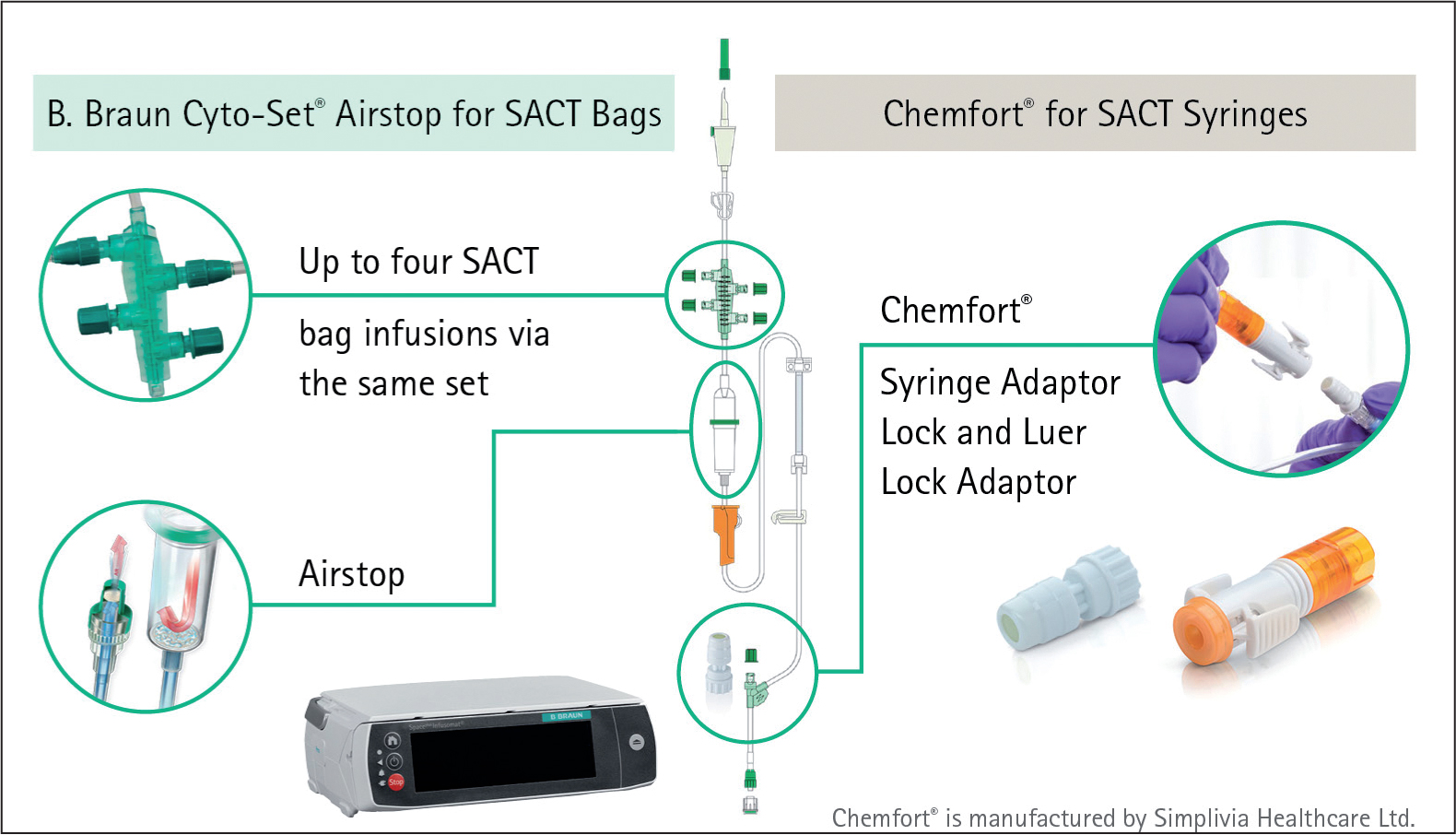
The giving sets each have four ports for secondary lines. Wellington explained: ‘This enables all the infusion bags to remain connected until the end of the infusion and thus the system remains completely closed. There is no need to prime secondary lines and there's no risk of air entering the line due to the AirStop technology in the drip chamber. Chemfort is a membrane-to-membrane closed system transfer device that we're using for SACT boluses and for mAb preparation.
‘The new system allows you to overestimate the SACT bag volume so, when the infusion is complete, the flush is already in situ [and] ready to connect. Simply clamp the line and reprogram the pump. The infusion interruption is greatly minimised and the exposure risk is eliminated as you're not swapping any bags - and therefore the infection risk is reduced as well. As the system remains completely closed, there is no need to don and doff PPE,’ Wellington said.
Time is saved by minimising the number of alarms and consequent reprogramming of pumps and not having to attach new flush bags to the patient's pump, recheck prescriptions or don and doff PPE.
Before the closed system devices were implemented, approximately 150 sharps bins were used per week. Now 80-litre purple bags are used instead. A sharps bin cost £2.44 but a purple bag cost 6p – and one bag holds as much as nine sharps bins.
Savings
Considerable savings have been made:
- A time saving equivalent to 33 10-hour shifts per year
- A saving of 10 000 flush bags per year
- A saving of 10 000 flush-bag spikes per year (plus a time saving equivalent to 22 10-hour shifts per year through no longer having to clean Luer ports)
- A sharp reduction in the number of ‘volume to be infused’ alarms (time taken fell from 1 hour 19 minutes to 12 minutes) - this is based on a Time Motion Study monitoring 43 treatments
- A saving of £19 000 per year on sharps bins (minus the cost of purple waste bags of ~£100).
A further benefit has been that the new pumps are more accurate and, as a result, infusions are more often completed on time, said Wellington.
Nurse perceptions of occupational exposure
UK Oncology Nursing Society (UKONS) president Dr Karen Campbell, Macmillan associate professor in cancer nursing at Edinburgh Napier University, provided an update on the ongoing PeCan study, which has now produced a wealth of data. This two-year study, funded by the UKONS, is examining nursing experiences and perceptions of potential occupational exposure to cytotoxic drugs.
The study comprises several elements – a systematic review, a UK survey and a series of in-depth interviews. The findings are now being prepared for publication.
One key finding from the systematic review was that, regardless of the level of knowledge among staff, ‘the chaos of clinical practice means that you know what you've got to do, you know how to do it but, in the chaos of that, it's not that you forget, but… things just slip,’ said Campbell.
She added that ‘people are reporting similar side effects from similar drugs across the globe’.
A total of 675 respondents from all over the UK completed the survey. The majority were women aged 31–50 years from cancer centres or district general hospitals. The results showed almost universal use of plastic aprons and chemotherapy gloves but also considerable variation in the use of closed systems.
‘There's a lot of variation and you can see where the debate is coming in about closed systems and implementation of them,’ said Campbell.
An audience poll showed that 24% of participants had experienced adverse effects from SACT and a further 50% were unsure. In the PeCan study, the most commonly reported side effects were headache, hair loss and eye irritation.
The results of in-depth interviews are still undergoing analysis but one important finding is that the fact that the study is being carried out has raised awareness of the risks among participants.
‘They suddenly become aware of the fact that they could be exposed - it struck a chord with them,’ said Campbell.
In conclusion, she said: ‘I still think we've got a bit of a fight on our hands to actually make sure that everyone gets the safety that they require to deliver these drugs.’
Building a business case
More than 50% of cancer patients survive and live for >10 years, although they may require continued treatment. The incidence of cancer is also increasing, with the result that the gap between capacity and demand for treatment is widening. Expanded services will be needed to deal with the increase in demand and safeguarding of staff will be paramount in developing effective services, Marius Nicola, market development manager at B Braun Medical, told the audience.
Some 47% of the audience were already using closed systems for SACT administration involving both bags and syringes, a further 18% for bags alone and 6% for syringes alone, according to a poll.
Implementing closed systems for SACT administration can satisfy a series of key objectives for hospitals and this can be built into a robust business case. The key to a good business case is describing the problem precisely and identifying clear objectives. As examples, Nicola suggested that the objectives could be:
- Reducing the risk of exposure to cytotoxic drugs for patients, staff and visitors by introducing closed systems for SACT administration
- Reducing the risk of exposure to SACT drugs by using CSTDs for preparation of mAbs in the clinical area
- Improving productivity and patient satisfaction by eliminating preventable delays in SACT administration
- Minimising the risk of hospital-acquired infection in SACT patients by eliminating de-spiking or disconnection of SACT bags and using a CSTD for safer SACT syringe administration.
All of these objectives could be met while ensuring adequate safeguarding of the health professionals involved.
The case for change should be built on evidence from the literature e.g. reports of occupational exposure, guidance from official bodies such as European Commission (2023) guidance and NHS guidance (NHS Pharmaceutical Quality Assurance Committee Guidance, 2018). The latter document states that:
- The practice of de-spiking ‘empty’ cytotoxic chemotherapy bags should be stopped
- Closed-system caps should be added to syringes before they are connected to the patient.
In addition, local risk assessments should be undertaken by carefully observing the ways in which SACT drugs are handled and noting the opportunities for environmental contamination. For example, when ‘empty’ SACT bags are taken down, they could still contain up to 2 ml of drug solution, which could vaporise from the chemotherapy waste bin. Up to 150 bags per day are used on some units so this adds up to a lot of discarded drugs, he noted. Such findings should be logged on the hospital risk register, he advised.
Every SACT nurse experiences delays resulting from overfilled SACT bags and consequent repeated alarms and reprogramming of pumps, said Nicola. The introduction of closed systems such as the Cyto-Set AirStop can eliminate these types of delays by removing the need for pump reprogramming, de-spiking and re-spiking of flush bags, as Wellington described.
The business case for the solutions proposed should be supported with evidence such as technical and clinical evaluations (showing what the devices do that is useful and the fact that they also work in a real-life clinical situation), as well as the economic impact that could be expected.
B Braun Medical can help with these because the company has experience of previous successful examples, said Nicola. Testimonials from satisfied customers can also help and the company has received numerous testimonials for Cyto-Set AirStop and Chemfort, he added.
Staff education in the use of closed systems is important and B Braun has a dedicated team of 12 clinical therapy specialists, all of whom are registered nurses or midwives, for this purpose. They can also help with implementation.
In summary, he said that there is now an opportunity to build a business case for change to prepare services for the future and to safeguard health professionals.
Discussion
During the discussion, a number of practical points were raised.
Asked whether the DNA change study (McDiarmid et al 2010), which was done with alkylating agents, might be repeated with monoclonal antibodies, McDiarmid said this would not be carried out because, unlike alkylating agents, monoclonal antibodies are not associated with specific chromosomal changes. Moreover, there is already epidemiological evidence for their adverse effects, such as increased risks of tuberculosis.
Participants asked if survey responses about PPE referred to practice in the past or now. Campbell noted that the responses depended partly on the respondents' backgrounds and interests and could include previous as well as current practice. She was not surprised by the variations because there is no standardised approach in the UK. Campbell added that people need to see where cytotoxic drugs are on wards – contamination studies help to generate awareness and drive action.
Participants asked about evidence for the safety of using purple disposal bags instead of sharps bins for disposal of SACT bags and giving sets. Wellington explained that when sharps bins were used in the past, the giving sets and bags were connected using Luer devices which were potentially contaminated with cytotoxic drugs that could aerosolise so containment in the sharps bins was necessary. With the Cyto-Set AirStop, the entire system stays closed all the time so there is no risk of leakage. The sets are placed in double purple bags in a metal bin before being transported to an on-site incinerator.
Wellington's advice on implementation was to recognise that the major barrier is always cost. Although the Cyto-Set AirStop is more expensive than standard giving sets, when the costs of the flush bags and nurse time are taken into account, its implementation resulted in savings in both costs and time.
Summing up, Foulkes said he concluded from the day's events was that ‘it would be better for patient safety, worker safety and nurses' perception of risk if closed systems were to be implemented’.
Conclusions
This meeting was the fifth in a series to examine the risks for nurses of exposure to hazardous drugs and the measures that can be taken to mitigate them. There was general recognition that nurses are exposed to hazardous drugs during administration and disposal of SACT and also during preparation of mAbs at ward level. Several conclusions can be drawn from the presentations:
- Appropriate provisions for risk management and ongoing monitoring of staff should be implemented
- Risk management measures should follow the hierarchy of controls and use the strongest available methods first i.e. start with engineering controls such as CSTDs
- The long-term effects of exposure to mAbs are as yet unknown but CSTDs should be used when they are prepared on wards to minimise the risk of exposure
- The implementation of closed systems – Cyto-Set AirStop and Chemfort – in an oncology day unit resulted in savings in time and costs for SACT administration.
- The implementation of the closed Cyto-Set AirStop system allowed major savings to be made in waste disposal as cytotoxic residues were completely contained.
- A 2-year study to determine nurses' experience and perceptions of occupational exposure to cytotoxic drugs has been completed and being prepared for publication.