

The fourth webinar discussing the results of research into the risks to nurses of occupational exposure to hazardous drugs and the protective role of closed system transfer devices (CSTDs) was held on 30 March 2023. The webinar was organised by Aesculap Academia, the educational arm of B Braun Medical Ltd. The earlier webinars in this series, held in November 2020 and April 2021, were reported in previous BJN oncology supplements (Clark, 2021a; 2021b; 2022).
Opening the meeting the chair, Naomi Clatworthy (Acute Oncology Nurse Consultant, Royal Devon University Healthcare NHS Foundation Trust) commented that previous meetings in this series generated excellent feedback. Some 500 people took part in this webinar and an audience poll at the start showed that 54% of respondents were ‘very concerned’ about the health effects of hazardous drugs.
Health effects of exposure to hazardous drugs
‘Biologically important exposure [to hazardous drugs] is occurring in the oncology work setting’, Dr Melissa McDiarmid (Professor of Medicine and Epidemiology, University of Maryland School of Medicine) told the audience.
The story begins more than 100 years ago with the weaponisation of mustard gas – an alkylating agent - during the First World War. Animal studies showed that this was associated with shrinkage of lymphatic tissue and led to the suggestion that it might be useful for treating lymphomas. By the 1960s alkylating agents had become a standard part of cancer treatment. However, by the 1970s there was a clear epidemiological signal (of drug-induced harm) – there was an increase in the number of secondary malignancies in patients who had been treated with the drugs. This prompted the next logical question: could healthcare workers also be exposed? By the late 1970s and early 1980s it was clear that healthcare workers were at risk.
A number of the drugs commonly used for cancer treatment are classified as Group 1 human carcinogens by the International Agency for Research on Cancer (IARC) (the cancer arm of the World Health Organization). About 18 of the drugs that we use are Group 1, ‘no holds barred’ human carcinogens. Another 11 out of 93 are classified as ‘probable human carcinogens’ (Group 2A) and a further 13 of 319 are ‘possible human carcinogens’ (Group 2B). In addition, many of these drugs are well-documented reproductive and developmental toxicants – in both women and men. They are associated with biologically plausible health effects (eg, myelodysplastic syndrome and secondary malignancies) in exposed populations. The Health and Safety Executive (HSE) (2023) recognises the hazard posed by these drugs and has published safe handling guidance.
There is variability in perceived risks associated with hazardous drugs and data from the European Biosafety Network (EBN) shows that about 55% of members undertake regular surface monitoring (EBN, 2018: 29). Of note, 42% of samples contained busulphan, 35% contained ifosfamide and 25% had cyclophosphamide (EBN, 2018: 20), showing that ‘contamination is fairly widespread’, said Dr McDiarmid.
Containment methods are needed to reduce contamination. In the UK, isolators are frequently used for compounding of cytotoxic doses whereas biological safety cabinets (BSCs) are more commonly used in the USA. A study in France (Crauste-Manciet et al, 2005) showed that most contamination was contained in an isolator, but traces of drug were also present on the exterior surface of IV bags and syringes and hazardous drugs were exported to other areas in this way.
Another study compared the use of needle/syringe (traditional) method with a closed system transfer device (CSTD) and showed that using a CSTD within the isolator resulted in markedly reduced surface contamination of products (Vyas et al, 2016).
Furthermore, numerous studies have provided good evidence of widespread contamination in areas where hazardous drugs are prepared and administered, said Dr McDiarmid. ‘Every study has been positive for at least one drug’, she added.
If the environment is contaminated, is there evidence that the drugs are getting into the staff? In one study analyses of urine found that 38% were positive for cyclophosphamide and 21% for ifosfamide. Worryingly, hazardous drugs were also found in the urine of other staff such as secretaries who did not compound drugs. (Wick et al, 2003)
The next step was to look for evidence of harm. Several types of studies have been used to demonstrate genotoxicity such as chromosomal aberrations or the presence of micronuclei. ‘Biologically important genotoxicity events are taking place in workers who have absorbed the drug’, she said. A meta-analysis confirmed that there was a significant association between occupational exposure to hazardous drugs and an increase in chromosomal aberrations (Roussel et al, 2019). Another way of looking at this was through the use of fluorescent in-situ hybridisation (FISH). This demonstrated deletion of the long chain of chromosome 5. A study of healthcare staff responsible for handling alkylating agents showed significant abnormalities of chromosomes 5 and 7 – those targeted by alkylating agents (McDiarmid et al, 2010).
Cancer experience in healthcare workers
Early studies of nurses and doctors in Denmark (Skov et al, 1990;1992) had shown 2.85-fold and 5.37-fold increases in the occurrence of leukaemias and haematopoietic cancers. Increases in cancer mortality in pharmacist and nurse workers have also been reported (Petralia et al, 1999). These types of study are difficult to do in the USA because there is no national cancer registry, noted Dr McDiarmid.
Occupational exposure to antineoplastic drugs among nurses was associated with a two-fold increase in spontaneous abortions, according to one study (Lawson et al, 2012)
It had been hoped that immunomodulatory drugs (such as adalimumab and etanercept) would be less dangerous but some do appear to cause an increase the numbers of lymphomas. So far, lymphomas, drug-induced lupus and neurological problems have been reported as adverse drug reactions so that definitely makes them hazardous, said Dr McDiarmid.
Anti-TNF (tumor necrosis factor) agents probably also need to have safe handling practices applied, she said. The updated National Institute for Occupational Safety and Health (NIOSH) hazardous drug list has yet to be released but the existing list is a reasonable guide (Connor et al, 2016). Many of the ‘-abs’ and ‘-ibs’ are reprotoxic and almost all carry warnings to that effect. They are categorised as ‘reprotoxicity Class D’ by the US Food and Drug Administration (FDA) for treated patients and so presumably should be handled as hazardous drugs by healthcare workers. At any rate, they should avoid exposure to these drugs when breastfeeding, she added.
Managing the risk
Managing the risks depends on using a hierarchy of controls. Level 1 is engineering controls, eg, safety cabinets, containment devices. Level 2 is administrative, eg safe work practices and training, and level 3 is personal protective equipment (PPE).
At the University of Maryland work to establish a national exposure registry has now reached an advanced stage. Safe handling guidance needs to be enforced, noted Dr McDiarmid.
In summary, Dr McDiarmid said that biologically important exposure to hazardous drugs was occurring in the work setting and that appropriate provisions for risk management and surveillance of staff need to be in place.
Reducing hazardous drug exposure risk and improved patient pathways
It has been known for some time that chemotherapy nurses are at risk but so far protective measures have focused largely on PPE and administrative controls and not on engineering controls such as CSTDs, according to Mr Thomas Marler-Hausen (Head of Nursing Operations, HCA Healthcare UK). Furthermore, HSE (2018) guidance advises using ‘totally enclosed systems where reasonably practicable’, but this is not followed. It also calls for monitoring of exposure in the workplace but this is not routinely done either, he said. Moreover, he doubted that occupational health departments had the specialist knowledge to advise on this.
He also noted that the HSE guidance effectively disregards the ‘low-level exposure risk’. A stronger stance has been taken in the USA where CSTDs are required when nurses administer hazardous drugs, he said. A UK team had undertaken a Cochrane review but had reached no firm conclusion. However, ‘We know that the risk exists …. [and ] we have this hierarchy of controls which tells us that engineering controls are better than PPE’, he said (ie, offer a more effective level of protection).
‘Our nursing practice in the UK is putting nurses at risk’ and the HSE guidance is out of date, he argued. We should be using closed systems wherever reasonably practicable and monitoring exposure, he emphasised.
He also called for studies to assess the effectiveness of environmental decontamination methods and studies to gain a better understanding of effective PPE. In addition, health and safety law should be changed to reflect the known risks involved in chemotherapy administration and an epidemiological study to assess the health outcomes of nurses who have worked in chemotherapy units should be set up, he said.
Improving patient pathways
Mr Marler-Hausen called for improved patient pathways. He explained that the existing pathways for prescribing, preparation and administration of injectable drugs do not always work well in practice. The widespread use of monoclonal antibodies (mAbs) is growing as they are now used for numerous conditions including many cancers, arthritis, psoriasis and asthma. The whole team needs to come together to develop the best clinical pathways, he suggested.
Ideally, many injectable products would be provided as dose-banded, long-expiry, ready-to-use items prepared in outsourced aseptic facilities. This facilitates an ‘off-the-shelf’ model that can be very efficient, although it can be more costly than nurse preparation of mAbs. When nurses prepare these injections the pathways work smoothly, ‘but is it safe and should we do it?’ he asked.
The question of whether mAbs are safer than cytotoxic drugs had been raised many times. In the absence of occupational health studies, toxic risks are extrapolated from the side effects of therapeutic doses – and nurses should adopt a cautious approach, he suggested. In 2009 a team of nurses and pharmacists had compiled a risk assessment tool and proposed a scheme for mitigating the risks (Langford 2009). It concluded that simple precautions such as the use of PPE during the preparation and administration of mAbs, and robust surface cleaning of handling areas were likely to be sufficient. However, it also acknowledged that the long-term risks of chronic low-grade exposure to the multiplicity of mAbs used in clinical practice were unknown.
More recently, Bauters and Vandenbroucke (2019) had proposed a scheme, which, if followed, would have demanded more aseptic compounding capacity in pharmacy departments. In 2022 the Clinical Oncology Society of Australia published a position statement that set out guidance on safe handling of mAbs in healthcare settings (Ryan et al, 2022). However, the guidance appeared to be inconsistent, he noted. One recommendation says that centralised preparation of mAbs is preferable but then a later recommendation advises the use of PPE alone and fails to stipulate the use of CSTDs (to minimise the risk of exposure) when mAbs are prepared and administered in clinical areas, he said.
If mAbs are prepared in clinical areas, a closed system should be used, Mr Marler-Hausen emphasised. Each institution should develop its own risk assessment tools. One advantage of preparing doses remotely in a pharmacy aseptic unit is that there are fewer interruptions and so errors are less likely, he said. However, there are advantages associated with nurse preparation of mAbs. For example, a comparison of pharmacy-prepared and nurse-prepared doses of bevacizumab had shown that when the nurse prepared the dose on the ward, patients could be turned round in 30 minutes compared with 3 hours when doses were prepared in the pharmacy. He noted that a nurse in one UK hospital had reported an adverse reaction when preparing a dose of bevacizumab (Barrott and Foreman, 2020) but this was likely to have been associated with the use of ‘a poor quality closed system device that did not satisfy the NIOSH definition’, he said.
Mr Marler-Hausen concluded that CSTDs should be used together with PPE. In addition, exposure in the workplace should be monitored, environmental decontamination methods should be assessed, health and safety legislation should be changed to reflect known risks, and epidemiological studies should be undertaken to assess health outcomes of nurses who have worked in chemotherapy units. He also suggested that a UK-wide risk assessment protocol for mAbs should be developed and that patient pathways should be mapped at local level.
Nurse perceptions of occupational exposure
Dr Karen Campbell (Macmillan Associate Professor in Cancer Nursing, Edinburgh Napier University) provided an update on the ongoing PeCan study. This 2-year study, funded by the UK Oncology Nursing Society (UKONS), is examining nurse perceptions of potential occupational exposure to cytotoxic drugs.
It is imperative that employers assess the risks to staff handling hazardous drugs and take suitable precautions, said Dr Campbell. The UK perspective is important because variations in practice across the globe cannot directly be matched to the UK, she added. Part of the underpinning rationale for this study is that the growth in the numbers of patients being treated for cancer and the absence of epidemiological evidence of the impact of hazardous drug handling is fueling continued debate and anxiety among nurses, she explained.
The study comprises several stages. The first stage is a systematic review that has now been completed. The second stage is a UK survey that was, she said, likely to be completed by the end of April 2023. The third stage will involve in-depth interviews with cancer nurses. Finally, the data will be triangulated to give a broad overview of the current landscape of experiences and perceptions of potential occupational exposure to cytotoxic drugs across the UK. Presentations at UKONS conferences in 2022 and 2023 will provide feedback to members and encourage discussion and debate, said Dr Campbell. The final results are expected in 2024, she added. In future, it should then be possible to build on the findings of this study to recommend evidence-based standards for practice. Dr Campbell encouraged cancer nurses to make contact with her if they are interested in participating in the in-depth interviews.
Building a business case for CSTDs
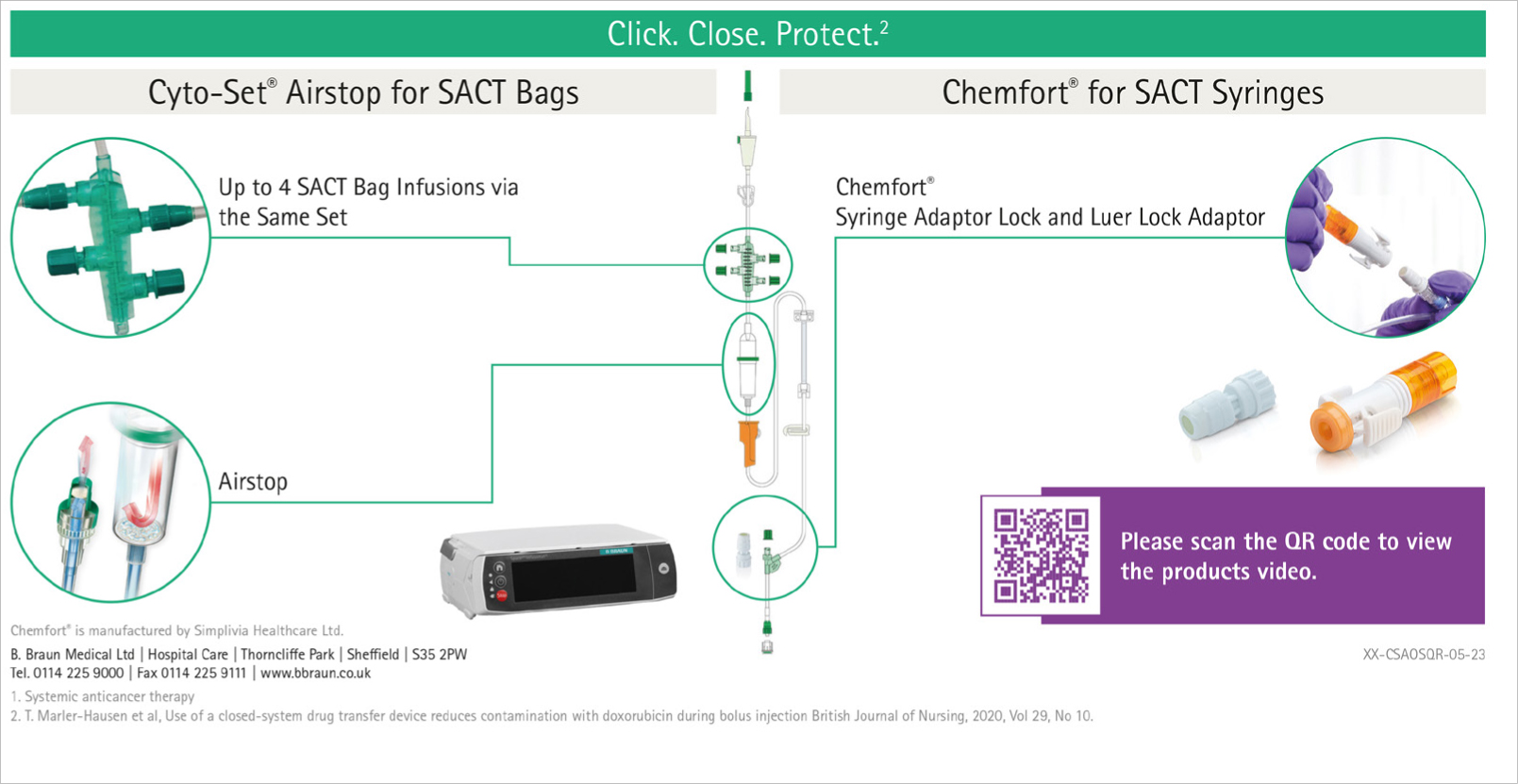
In the UK there are 385 000 new cases of cancer per annum and growing numbers of people survive and live with cancer. Since 28% of all cancer patients receive chemotherapy, there is increasing pressure on cancer services as they struggle to keep pace with demands. Against this background, nurses now have the opportunity to build a case for change to address critical challenges and prepare the service for the future, according to Marius Nicola (Market Development Manager, B Braun Medical). He described how a business case for the implementation of two products – the Infusomat Cyto-Set Airstop and Chemfort CSTD – might be built.
The ‘Click.Close.Protect.’ system for systemic anti-cancer therapy (SACT) administration comprises the Infusomat Cyto-Set Airstop for SACT bags and Chemfort CSTD for syringe administration. The Cyto-Set Airstop is designed for administration of up to four SACT bags without having to disconnect. Chemfort incorporates all of the features of its predecessor (Tevadaptor) together with some new features. The Chemfort CSTD relies on Toxi-Guard air cleaning technology and elastomeric, membrane-to-membrane, linear connection and disconnection. No ‘pushing and twisting’ is required.
In building a business case for the implementation of closed systems for preparation and administration of hazardous drugs, key objectives are the elimination of preventable SACT therapy delays, prevention of occupational exposure for healthcare staff and tackling the shortage of aseptic unit capacity while maintaining or increasing the level of service, and safeguarding and retention of staff.
It is important for a business case to have a clear structure. Ideally this should start with a description of the problem, followed by the case for change and then the solution. The case for change should incorporate local data such as risks recorded in the local risk register and specific, preventable delays in treatment. Risks could, for example, include the risks of leakage or droplet release (of hazardous drug solutions) during administration of SACT from IV bags or syringes when using open or semi-closed systems. One important source of potential contamination is empty IV bags of SACT solutions that have been despiked ready for disposal. Although ‘empty’ such bags can contain up to 2 ml of drug solution that could end up vaporising from the chemotherapy waste bin, said Mr Nicola. A guidance document from the Specialist Pharmacy Service (Santillo et al, 2018) provides useful information on this point, he added.
Time delays of up to 20 minutes can occur when conventional administration sets are used for SACT bags. The nurse will set the volume to be infused in the volumetric pump to administer the required dose volume but because the IV bags contain up to 10% overage, a significant amount is left in the bag when the pump signals the end of the infusion. Additional nurse time is needed to reprogram the pump again and again to make sure all the drug is infused while avoiding the risk of pushing air into the line. This delay can be eliminated using Cyto-Set Airstop as it allows over-estimation of the volume to be administered without the risk of air entering the line. Thus, if a unit administers 10 000 SACT bags per year and saves 4 minutes per bag, delays of up to 600 hours can be avoided, improving patient satisfaction and productivity, he explained.
Another opportunity for time saving arises where chemotherapy bags are routinely despiked to allow for the attachment of a flush bag. This requires time for the nurse to don PPE and obtain the flush and for the despiking and respiking procedures. If CytoSet AirStop is used instead, the flush solution is in place from the outset (on the primary line). Even if the time saving is only 1 minute per administration this would amount to 166 hours per year in a unit that administers 10 000 doses per year.
This type of information could be used in a business case to show how the implementation of a closed system could not only help reduce the risk of exposure to hazardous drugs but could also streamline working procedures and improve efficiency.
Discussion
During the discussion a number of practical points were raised.
Some centres do not permit staff of child-bearing age to prepare mAbs. Mr Marler-Hausen said that in the past the decision had been left to individual nurses but he now believed that the decision should be made by the occupational health department. Dr Campbell noted that staff may not wish to move out of the SACT unit because the working hours may be less convenient. Also, the majority of staff are at an early stage in their careers and may be reluctant to ‘shout out’ or ask for protection, she added. Dr McDiarmid said that any transfer had to be non-punitive with no downside for the staff involved. In addition, ‘the hazard communication needs to be crystal clear’; when the manufacturer declares the risks in the package insert ‘the bright line cannot get brighter’, she added.
Asked how best to monitor exposure in the workplace samples, Dr McDiarmid said that regular monitoring of surface contamination is recommended in some countries (such as Germany). It is also recommended in the USA, as a good work practice, although the ‘rules’ are not always followed assiduously. Even intermittent monitoring can have a value because a positive result may surprise people and can be used to reinforce the importance of hazard avoidance, she said.
Conclusions
This meeting was the fourth in a series designed to examine the risks for nurses of exposure to hazardous drugs and the measures that can be taken to mitigate them. There was a general acknowledgment that nurses have not always been adequately protected and, in view of the growing demand for cancer treatment, better protective measures need to be implemented. Several conclusions can be drawn from the presentations:
- Appropriate provisions for risk management and ongoing monitoring of staff should be implemented.
- Risk management measures should follow the hierarchy of controls and use the strongest available methods first, ie, start with engineering controls such as CSTDs
- The long-term effects of exposure to mAbs are as yet unknown but CSTDs should be used when they are prepared on wards in order to minimise the risk of exposure.
- Wherever possible, hazardous drugs should be made available (by the pharmacy) as dose-banded, ready-to-use products.
- The use of some closed systems leads to considerable time savings and this information can be used to support the business case for their implementation.
- The 2-year study to determine nurses' perceptions of occupational exposure to cytotoxic drugs is in progress and on course for completion by 2024.