
The legislations around organ and tissue donation changed in 2019 and 2020 with the implementation of Human Transplantation and Anatomy (Jersey) Law 2018 and The Organ Donation (Deemed Consent) Act 2019 in England.
Wales was the first nation in the UK to move from an opt-in to an opt-out system in 2015, with the implementation of the Human Transplantation (Wales) Act 2013 (Madden et al, 2020). With the opt-in system, people have to actively sign up to the register to donate their organs and tissue after death. The opt-out system works on the understanding that all adults agree to become organ donors when they die, unless they have made it known that they do not wish to donate by opting out or raising an objection. There are safeguards in place and, as such, certain groups are excluded:
- Individuals under the age of 18
- Those who lack the mental capacity to understand the new arrangements and take the necessary action
- People who are not ordinarily resident in England or Jersey.
The changes from an opt-in to an opt-out system of organ donation were introduced to save and improve more lives by increasing donor numbers. The blended training approach has been discussed in previous articles (Hubner et al, 2020; Miller et al, 2020; Walton et al, 2020), and we are now in the implementation and embedding phase of the change.
Learning from Wales
The key activity at the start of the legislation change programme was a listening event with colleagues from the Welsh organ donation team. We wanted to better understand the rationale for the approach taken for training and embedding the change, and what could be done to build on that for England and Jersey. In addition, the impact of the change in the clinical environment, the specialist nurses and the families involved in the donation process was documented by Noyes et al (2019) for Bangor University in conjunction with NHSBT, providing essential learning to inform our delivery.
The two essential interventions to ensure success of embedding the change in England and Jersey and to gauge the workforces readiness for the change were:
- Debriefs, which provide staff with the opportunity to bring their own ‘real life’ clinical experiences to work through the deemed legislation criteria
- Regular temperature check surveys, which are part of organisational change that enable staff to provide feedback on how they feel the change has enabled them to work within a new framework.
Effective change management
Not only have we undertaken a legislative change, but following an organisational restructure, Tissue and Eye Services (TES) have moved into the same directorate as organ donation. Becoming the Organ & Tissue Donation and Transplantation Directorate (OTDT) has enabled consent process documents from both directorates to be combined, enabling even greater collaboration and better aligned, consistent practice. Legislation ‘champions’ were identified across the entire directorate to disseminate key messages among the workforce and to feed back to the legislation change team.
Organ and tissue donation colleagues reviewed the documents used for consenting organ and/or tissue donors collaboratively. Within the quality assurance (QA) system, procedural documents are written to detail what the role of the specialist nurse is for all aspects of the donation process. The process documents pertaining to consent were updated in line with the new legislation and all documents streamlined into a consent manual and an accompanying rationale document to provide an evidence base for the consent process. The consent documents were reviewed and validated by lead specialists in consent, scheduled purposes (research) and QA to ensure that all the information included was relevant and up to date with current practice.
Operational temperature checks
Over the course of the legislation programme it was essential to ‘check-in’ with the operational workforce to gauge their understanding of the law, its practical application and to hear feedback about how the changes were understood. This is good practice in change management and built on learning from the Welsh experience of introducing deemed legislation, which provided an opportunity to garner opinion and support for the changes, and allowed us time to remedy any concerns as they arose through a number of forums.
There were three temperature checks before the legislation was enacted, which were questionnaire surveys to gain insight and understanding as to how the staff feel the change has enabled them to work lawfully within the new framework. One was undertaken before the changes in law, one immediately after the change, and a final one 6 months post implementation. Giving ownership of the change to the workforce has proven to be a vital component in embedding new practices, as well as for receiving reliable and timely feedback and providing the opportunity to demonstrate we have heard those messages by flexing our approach to delivering change.
Embedding the change
Throughout the change process, the legislation change team (LCT) has been planning how to transfer the in-depth knowledge pertaining to the law into all training for organ and tissue donation staff. The LCT has been working closely with the professional development specialist (PDS) and TES teams, and these colleagues were involved in the creation and training delivery of the final module.
Although the law change is significant, it does not cover all aspects of the consent process for organ and tissue donation. It has therefore been important to continue to work on all aspects of consent, while implementing this historical law change, such as advanced communication skills, the training of new specialist nurses and the facilitation of donation from those who fall outside the criteria for inclusion in deemed consent. A continual exchange of information and handover of well-developed networks and resources is essential to ensure knowledge has been transferred back into the wider PDS team, and this should form part of the organisation's continuous improvement strategy.
Each regional PDS facilitates shared practice sessions within the regional organ donation services team, which helps to focus on regional trends to make improvements. Each of the regional PDSs is planning to run local ‘deemed focused’ sharing practice sessions: these will focus on any local trends and the needs of the team. In some regions, an anonymous questionnaire was forwarded to the specialist nurses in order to gauge confidence in the application of deemed consent and any other potential problems with the legislation. The results of this questionnaire guided the regional shared practice session.
Debriefing
As part of the ongoing transfer of legislation knowledge, we have facilitated more than 120 debriefs (more than half of all deemed approaches in the first 6 months) involving the specialist nurses who have been part of family conversations where deemed consent may apply. As part of this, specialist nurses are encouraged to complete a semistructured ‘debrief form’ to capture the main learning points from their conversation, as well as a virtual debrief.
The debrief is facilitated by members of the LCT, together with the workstream lead responsible for operational readiness, and includes operational members of staff involved in the conversation, as well as the regional PDS. These learning points will form the basis of future national practice sharing in the regional teams across England. These will be facilitated by the regional and national PDS team and will help embed the change in legislation and support the specialist nurses, having an unanticipated yet positive impact on mental health and wellbeing, by being able to ‘offload’ difficult cases or experiences.
The debriefing exercise will continue after the legislation has been implemented to capture as much learning from the live environment as possible, which will inform future training activities and ensure that the training environment reflects that experienced in the real world. They will also provide assurance that the law is being implemented appropriately and effectively in practice, having spent significant time with specialist nursing colleagues ascertaining their understanding, as well their acceptance of the change in practice. After 6 months, the debriefing video calls transitioned into the PDS team and are an ongoing feature of local and national shared practice forums.
Feedback from the 6-month operational temperature check has illustrated how effective and popular the debriefing model has been and demonstrates that there is a clear appetite for the debrief sessions to continue in future.
It was considered that to use debrief scenarios based on the DONOR acronym (Figure 1) and key areas of training such as diversity and inclusion would help ensure that the PDS team would be able to incorporate these in all training, either within sharing practice in regional teams or during national courses.
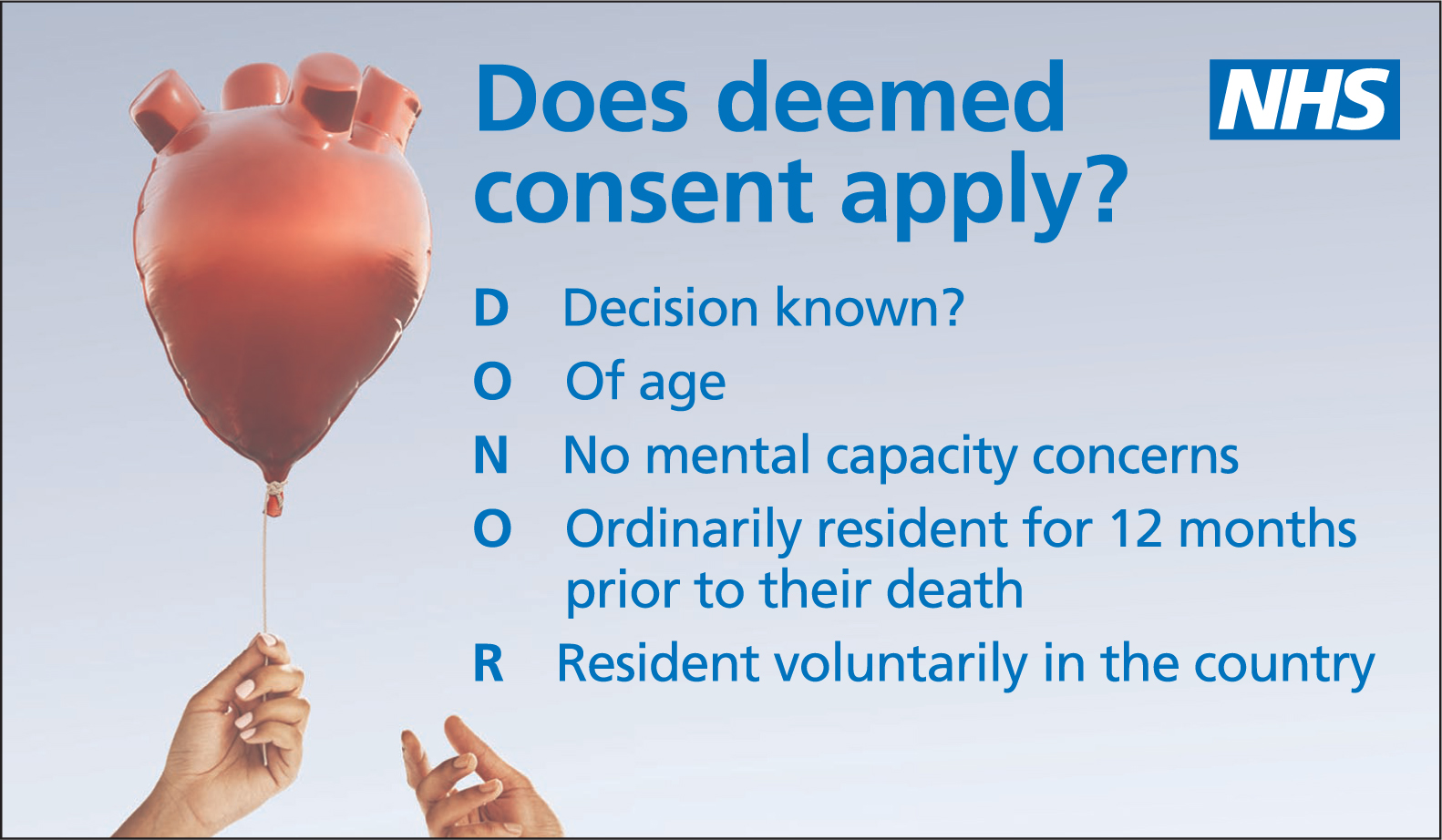 Figure 1. As part of training, the debrief scenarios have included the use of the DONOR acronym
Figure 1. As part of training, the debrief scenarios have included the use of the DONOR acronym
Embedding the change
According to the Kotter (2012) model (Figure 2) efforts should be made to ensure that change is present across all aspects of an organisation, ensuring that all leaders are brought into the change. We are working on this by talking about progress at every opportunity, sharing success stories about the change process, and being part of debriefs. It is important, through the handover process, that plans are created to ensure the legacy of the law change is not lost or forgotten.
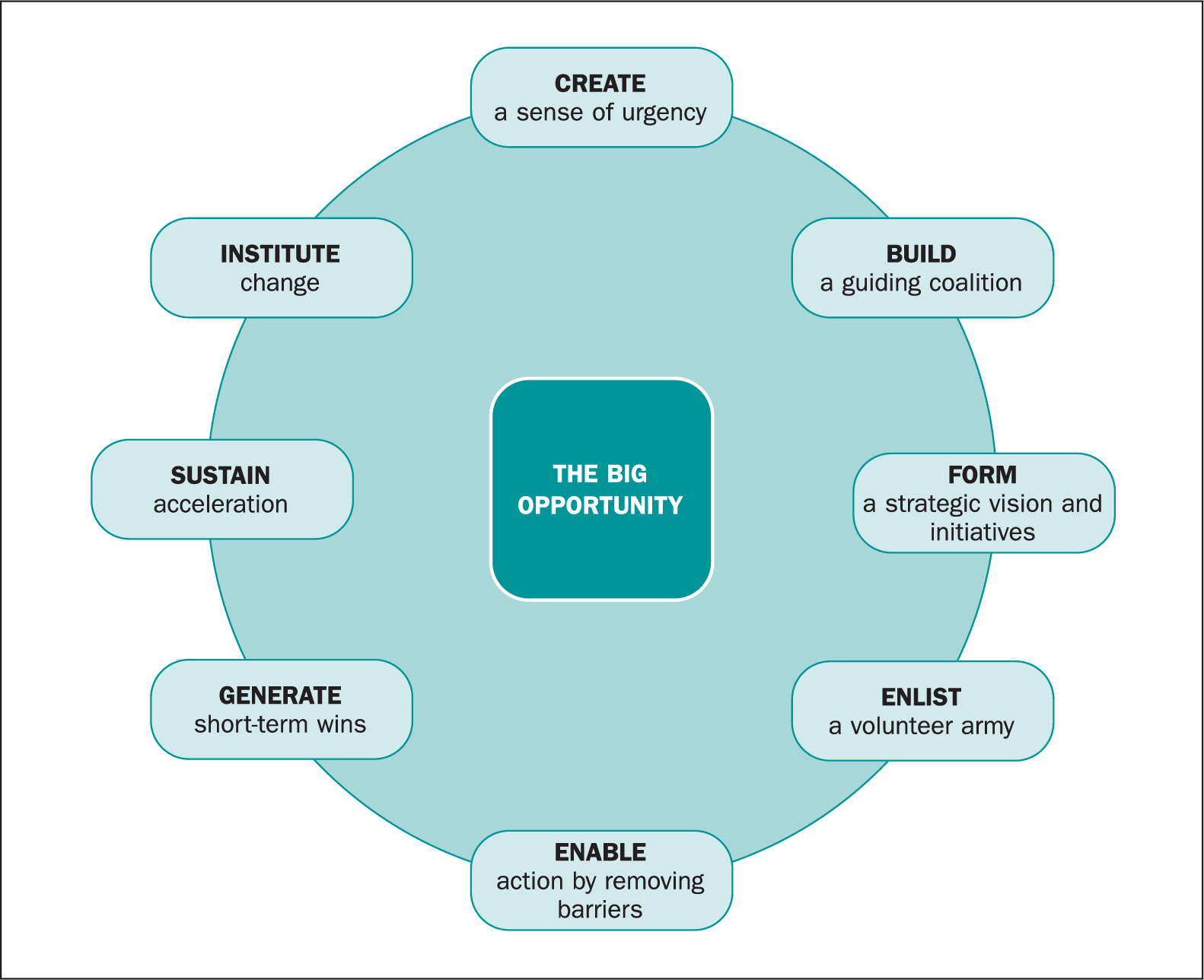 Figure 2. Change model illustrating the breakdown of eight change management steps of organisational change
Figure 2. Change model illustrating the breakdown of eight change management steps of organisational change
Legacy: supportive resources
There is now a variety of resources held in digital applications that can be accessed by specialist nurses in the OTDT when out in the clinical environment. The range of available resources therefore is able to suit a variety of learning styles.
The resources include the Human Tissue Authority Codes of Practice, procedural documents for the consent process, videos of hypothetical deemed consent scenarios filmed with specialist nurses and professional actors playing family members, training slide sets, conversation pointers, and faith, beliefs and culture resources. The applications containing the resources are an important legacy for the LCT to have for specialist nurses to access and as part of the handover to the permanent PDS team.
Summary
The multifaceted approach and the delivery of the three modules, the handover to the PDS team, embedding into clinical practice and the debriefs have meant that the implementation of the legislation into clinical practice has been possible during the difficult time of a pandemic.
Where debriefs have been undertaken, it has been possible to assess in real time whether the training has been understood, and to identify and discuss any gaps and misconceptions as part of our ongoing commitment to the change management approach.
A positive trend of specialist nurses completing medical and social history questions prior to the organ and tissue donor consent form was identified. This has helped specialist nurses confirm the deemed consent exclusion criteria prior to consent being formally written, meaning that questions such as those around ordinary residence can be ascertained without the need for asking the question directly and in a more conversational manner.
During the implementation of the legislation change in England it was identified that the ‘Consent for organ and/or tissue donation’ form requires an update to reflect the ‘order of consent’ and reduce the risk of consent errors.
The organisation is supporting the ongoing plan to continue with the debriefs. It has been identified that there was an appetite from the specialist nurse workforce to be able to debrief soon after an approach to a family for organ donation has been undertaken.