
In recent years there has been a plethora of guidance about the safe insertion and general care of enteral feeding tubes. However, nurses continue to be concerned about many aspects. This article provides some strategies to deal with some of the most common problems nurses will encounter when caring for patients with enteral feeding tubes, as well as looking at national guidance around the safe care of these tubes.
What is an enteral feeding tube?
An enteral feeding tube is one that allows feed to be administered via a tube directly into the stomach or the small bowel (Druml et al, 2016). It is used in individuals who have functioning guts but who are unable to meet their nutritional requirements orally. A report by BAPEN's British Artificial Nutrition Survey (BAPEN, 2018) suggested that there are about 3216 patients in the community receiving enteral tube feeding. There is a wide variety of tubes and the most common devices are listed in Table 1.
| Type of tube | Method of insertion | Common conditions used in |
|---|---|---|
| Fine-bore nasogastric feeding tube | At the bedside | Short-term feeding in a variety of conditions: generally, when it is expected that the patient will be able to tolerate oral nutrition again or until a long-term nutrition plan is made |
| Nasojejunal feeding tube | Bedside or radiologically; sometimes endoscopically | Short-term feeding for patients who cannot absorb feed into the stomach and so need to be fed into the jejunum |
| Percutaneous endoscopic gastrostomy (PEG) tube | Via endoscopy | Patients with neurological disorders, where there is little or no oral intake and the tube is not likely to be needed long term |
| Radiologically inserted gastrostomy tube (RIG) | Via X-ray | As above, in cases where it is not possible to pass a tube using endoscopy |
| Jejunostomy tube | Surgically, endoscopically or radiologically | For patients who cannot absorb feed into the stomach and so need to be fed directly into the jejunum (small bowel) |
Although there are many types of tube and different methods of insertion, what they all have in common is that they need to be well maintained and the patients who have them need to be cared for in the safest manner possible.
Fine-bore nasogastric feeding tubes
It is estimated that over 790 000 nasogastric feeding tubes are inserted in the UK each year (NHS Improvement, 2016), the majority of which are passed and used safely without causing harm. However, evidence from NHS Improvement (2016) has shown that patients were still coming to harm or dying as a consequence of tubes being misplaced into the lungs and the patient then being fed without the error being detected. This is despite the fact that tube misplacement was designated a Never Event in 2009 and Patient Safety Alerts were issued in 2011 and 2012 by the National Patient Safety Agency (NPSA) (now part of NHS Improvement), highlighting steps that must be taken and actions that must be avoided to prevent patients coming to any harm (NHS Improvement, 2016).
There still seems to be much confusion and anxiety among nurses around the safe insertion and ongoing care of fine-bore nasogastric tubes. However, certain rules must be adhered to and all trusts should ensure that these are embedded in their practice. The rules are that:
One example of a dangerous practice is flushing water into a tube when it has not been possible to get aspirate. This should never be attempted because there is no guarantee that the water is not going directly into the patient's lung.
The auscultation test
Known as the ‘whoosh’ test, this is the practice of injecting air into the tube and listening with a stethoscope over the stomach for a ‘gurgle’ or ‘whoosh’ because this is assumed to indicate that air is reaching the stomach. This method has been proved unreliable because the tube could actually be inside the oesophagus or the lungs (Turgay and Khorsid, 2010).
The auscultation test was banned by the NPSA (2005) more than a decade ago. This is because patients had died as a result of the tube being passed into the lung, but assumed to be in the stomach because practitioners had heard the gurgling sound.
The latest case in which this occurred was cited 3 years ago by NHS Improvement (2016) when it reported that two patients had died after having their tube placement ‘confirmed’ by the so-called whoosh test and consequently fed. It is the responsibility of every nurse involved with nasogastric tube placement and ongoing care of the patient to challenge this practice, if they see it happening.
Other types of feeding tubes
To many people, a percutaneous endoscopic gastrostomy (PEG) tube refers to any tube that goes into the stomach, regardless of where it is feeding into. It is, however, vital that nurses understand what type of tube they are looking at so they can provide the patient with the most appropriate care.
Nurses caring for patients with a feeding tube need to be knowledgeable about the different types of tube available and how each of these is placed.
PEG tubes
A PEG tube is placed under sedation in an endoscopy department. It has an internal retention device often known as a ‘bumper’, which sits in the stomach to hold the tube in place and an outside disc that sits close to the abdominal surface (Figure 1). These are not sutured, but together they keep the tube in place.

To prevent a condition called ‘buried bumper’ the tubes must be advanced and rotated 360° daily (Thompson, 2017). Table 2 illustrates the immediate, early and late complications that can occur with PEG placement.
| Immediate (occurs straight after the procedure) | Early (occurs within the first 4 weeks of having the procedure) | Late (occurs after the first 4 weeks of having the procedure) |
|---|---|---|
|
|
|
|
Radiologically inserted gastrostomy tubes
Radiologically inserted gastrostomy tubes (RIGS) are placed in radiology—under local anaesthetic—often with sedation. Due to the nature of the insertion, RIGS are sutured on the outside of the patient's body. The sutures either fall off or can be removed after 14 days. The tube is held in place on the inside with a balloon (Figure 2), which is inflated with a small amount of water. The complications listed in Table 2 also apply to radiologically inserted tubes. The balloon should be checked weekly for leakage and the water changed. The tube itself should be changed at between 3 and 9 months, depending on the manufacturer's instructions, by appropriately trained registered nurses or doctors.

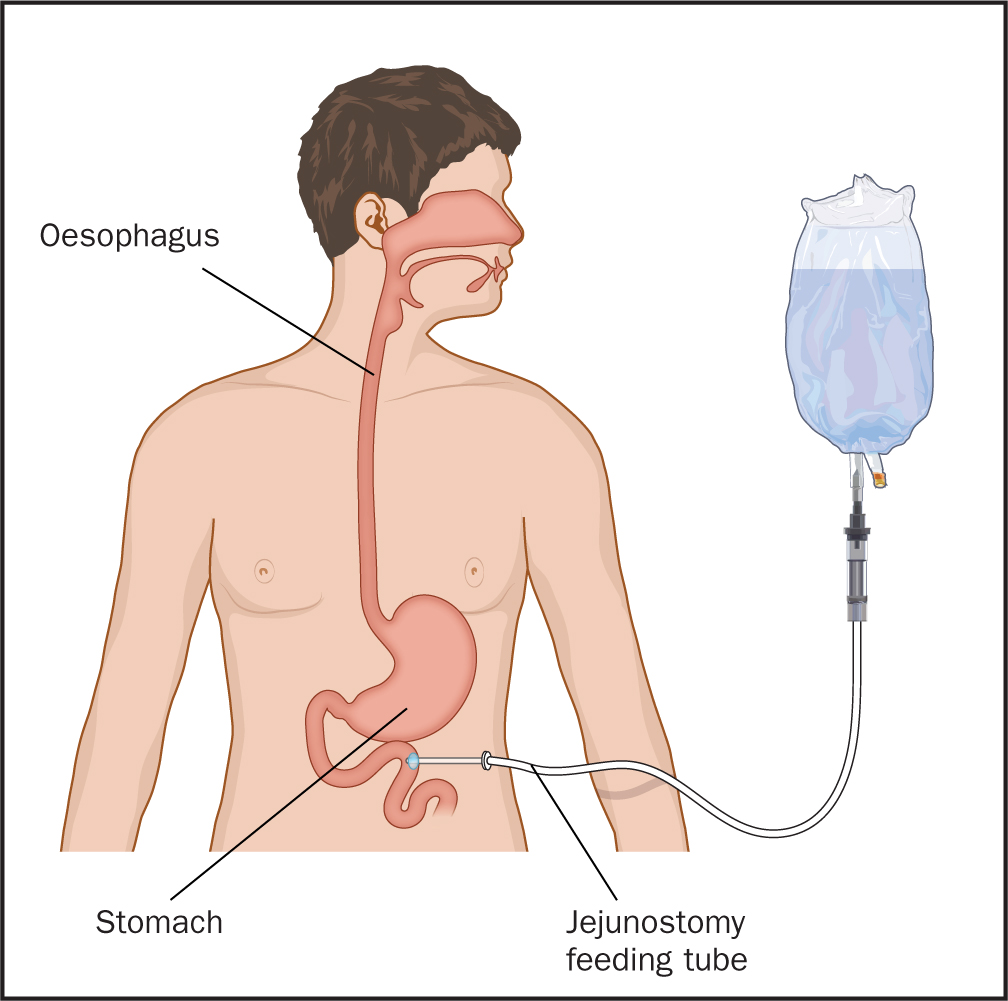
Jejunostomy tubes
Jejunostomy tubes can be placed using endoscopy, radiology or surgery (Figure 3). They are either sutured on the outside or have an inner Dacron cuff to hold them in place. Long-term securement of these tubes can be problematic. In general, they last between 6 to 9 months.
The care of these tubes is reasonably straightforward and is much the same as for that of the other enterally placed devices. The main difference is that jejunal tubes must not be rotated—the tube design means that, if rotated, they can become twisted or knotted inside the jejunum.
Troubleshooting guide
Does the tube need a dressing?
Tubes that are inserted via the nose will need a dressing or tape to hold them in place. In general, it is advised not to put a lot of tape around the nostrils because this can be uncomfortable for the patient and perhaps encourage pulling and tugging, which can lead to displacement. Curtis (2013) suggested that the tube should be taped to the nose and cheek using soft hypoallergenic tape. Before fastening the tube, nurses should ensure that the patient's skin is clean and free from oil, which can cause the tape to lose adherence. The skin should also be regularly inspected and the dressing changed to prevent pressure damage.
PEG/RIG/jejunostomy tubes
It is recommended that these tubes should not have a dressing at the exit site unless clinically indicated or the patient has requested it (Thompson, 2017). For the first 14 days after placement, the site should be treated as a surgical wound and cleaned with sterile gauze and water using an aseptic technique. Subsequently, it can be cleansed using a clean, single-use cloth and soap and water. It must be dried thoroughly and it is advisable not to put creams or powders on the site because these can increase the risk of infection or skin breakdown (Simons and Remington, 2013).
The external fixation plate must not be further than 2–3 mm from the skin to prevent leakage of stomach contents and to help form a good stoma tract.
Blocked tubes
Prevention is always better than cure. However, should a tube become blocked there are ways to deal with this safely. Simons and Remington (2013) have recommended that rolling the tube between thumb and forefinger can help break down any blockages. Concurrently pulsatile flushing with warm water in a syringe has also been known to help (Thompson, 2017). However, it is not advisable to put too much pressure on the tube using this method because it could lead to damage or even break the device.
Some organisations continue to advocate the use of fruit juices and carbonated drinks such as cola to clear blockages. However, this should not be done—it can make a blockage worse because the acid in the liquid will mix with the feed, resulting in more blockages (Shipley et al, 2016).
Before attempting or considering the unblocking of a nasogastric tube, you must check your organisation's guidance on the method to use. If unblocking a nasogastric tube, it is important to remember that it could have become dislodged before the blockage, and therefore introducing fluids into the tube to disperse a blockage could be seen as a risk. The tube may have become displaced and may no longer be in the stomach. This means that the patient could subsequently be fed into the lungs.
The biggest reason for blocked tubes is insufficient flushing. This is particularly important when administering medications. However, medicines given via enteral feeding tubes are often not licensed to be given via this route, so the Care Quality Commission (CQC) (2018) states that the prescriber needs to give:
When administering medication via the enteral route, nurses should follow a few simple rules:
If you have any shadow of a doubt always consult a pharmacist. Do not leave it to guesswork.
Enteral tube feeding is becoming more commonplace both in the community and in hospital settings. It is important that nurses looking after patients with gastrostomy feeding devices ensure that they keep professionally up to date with best practice national and local guidelines and undertake appropriate training to ensure the delivery of high-quality ongoing care.
This article has provided a brief overview of the most common types of enteral feeding tubes and the problems that nurses may encounter. However, nurses should be aware of the full range of devices by undertaking further reading and training, if necessary.