

An injury to the skin and underlying tissues caused by pressure is called a pressure injury (European Pressure Ulcer Advisory Panel (EPUAP), National Pressure Injury Advisory Panel (NPIAP) and Pan Pacific Pressure Injury Alliance (PPPIA), 2019). Previously known as bed sores, pressure injuries are among the most common wounds managed by healthcare staff (Al Aboud and Manna, 2023).
Certain people are at a significantly higher risk (Mondragon and Zito, 2023): for example, those with limited mobility after surgery (usually orthopaedic patients), people with neurological or cardiovascular disease and those with malnutrition or dehydration (Wood et al, 2019). Long-term conditions that put patients at greater risk including brain injury, dementias, stroke, heart failure and hypotension (Zaidi and Sharma, 2024).
In the UK,Wood et al (2019) found that over 700000 patients are affected by pressure injuries each year, and people aged over 75 years who developed a pressure injury in hospital had their stay extended by 10 days.
Pressure injuries cost the NHS £1.4 million each day, which is 4% of its total expenditure (National Institute for Health and Care Excellence (NICE), 2024).
It is estimated that just under half a million people will develop at least one pressure ulcer and around one in 20 people admitted to hospital with a sudden illness will develop a pressure ulcer in any given year (Al Aboud and Manna, 2023).
The above highlights the importance of understanding how to prevent and manage pressure injuries.
Causes
The causes of pressure injuries are multifactorial, and both external and internal factors can contribute to their development (Zaidi and Sharma, 2024).
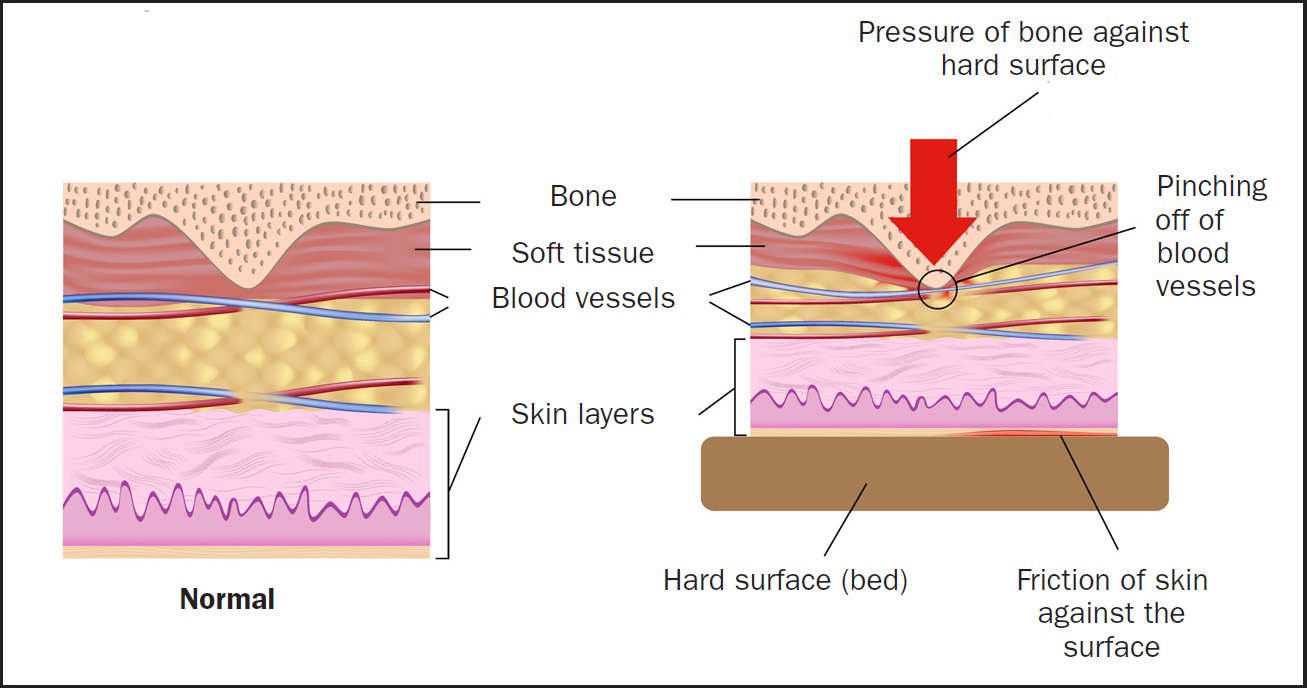
Oxygen and nutrients in the blood are needed to help keep tissue healthy. Tissue that is damaged will eventually die without a constant blood supply. When blood flow to tissue is restricted by pressure for any length of time, there is a risk of a pressure injury developing (Figure 1) (Al Aboud and Manna, 2023). Pressure, moisture and friction can lead to tissue ischaemia, while malnutrition and anaemia can accelerate tissue breakdown (Kottner et al, 2020).
Once the blood supply is cut off, tissue damage can begin in a short time depending on how much pressure is applied. If hard pressure is applied, a stage 3 or 4 pressure injury can develop in as little as 2–3 hours (Hess, 2004).
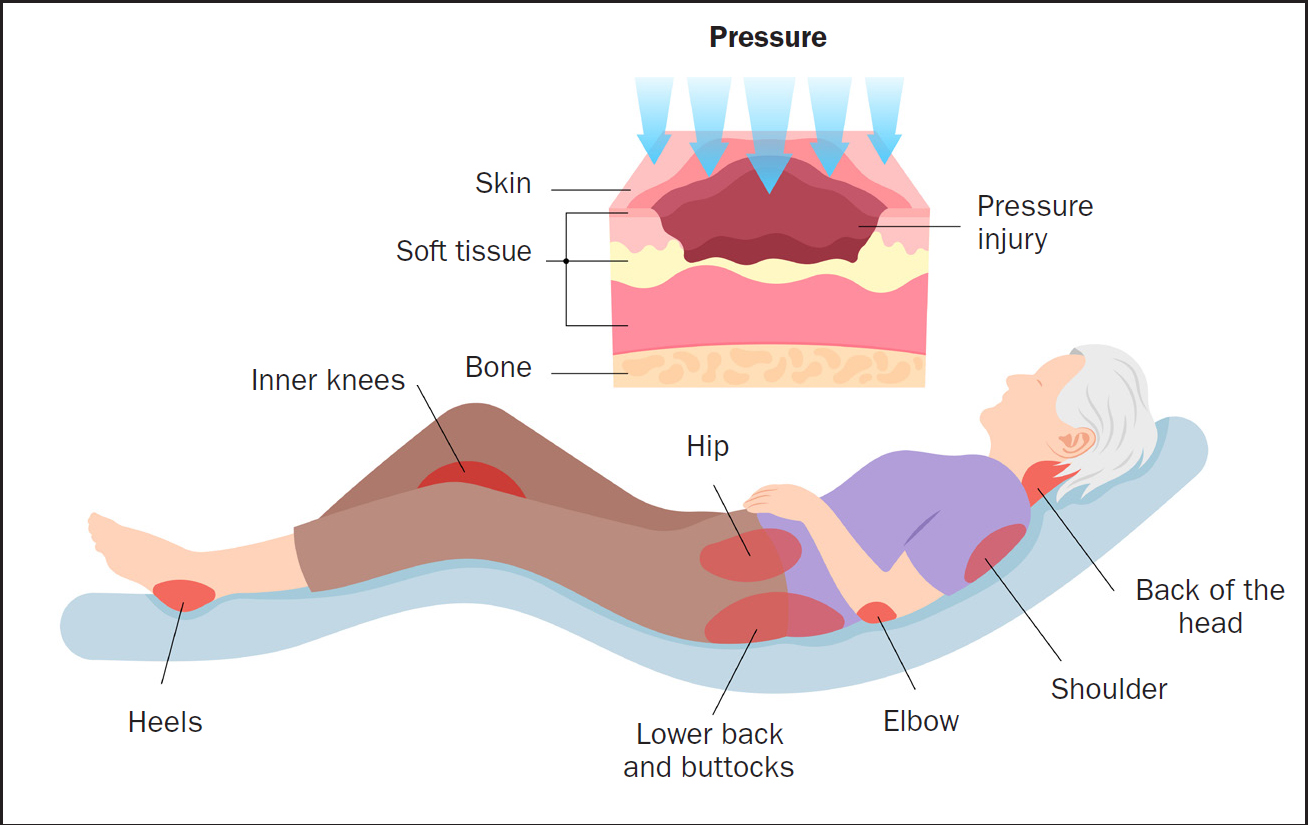
Anyone can develop a pressure injury; therefore, it is crucial to check areas subject to pressure regularly to ensure early detection and treatment. Bony prominences, including those listed in Box 1, are at risk of developing pressure injury when added risk factors are applied; irrespective of position, pressure will always be applied to these areas (Figure 2).
Areas of the body at risk of pressure injury
Sources: National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance, 2014; NHS Inform, 2023
Patients who are malnourished with a BMI <18.5 or have comorbidities are at greater risk. These are classified as internal risks. External risk factors include equipment, immobility, humidity, incontinence, pressure, friction and shear force (Chaboyer et al, 2018).
Pressure injuries are classified by the NPIAPand the International Statistical Classification of Diseases and Related Health Problems (ICD-11) (Kottner et al, 2020). The NPIAP uses the term stage while the EPUAP uses the term classification to described the level of damage caused by pressure.
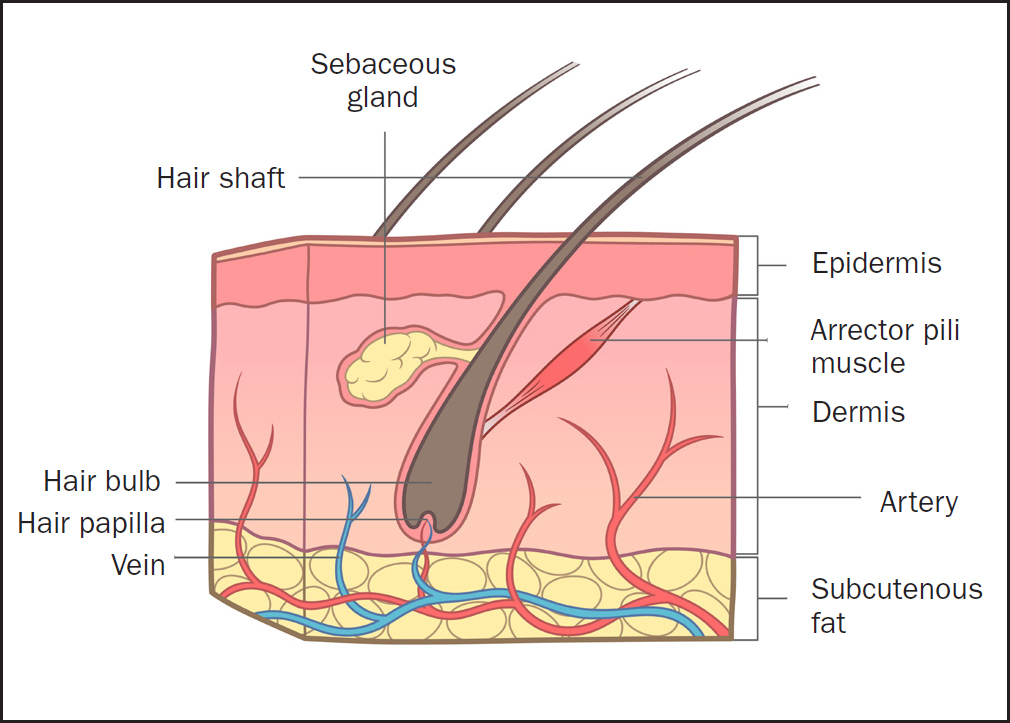
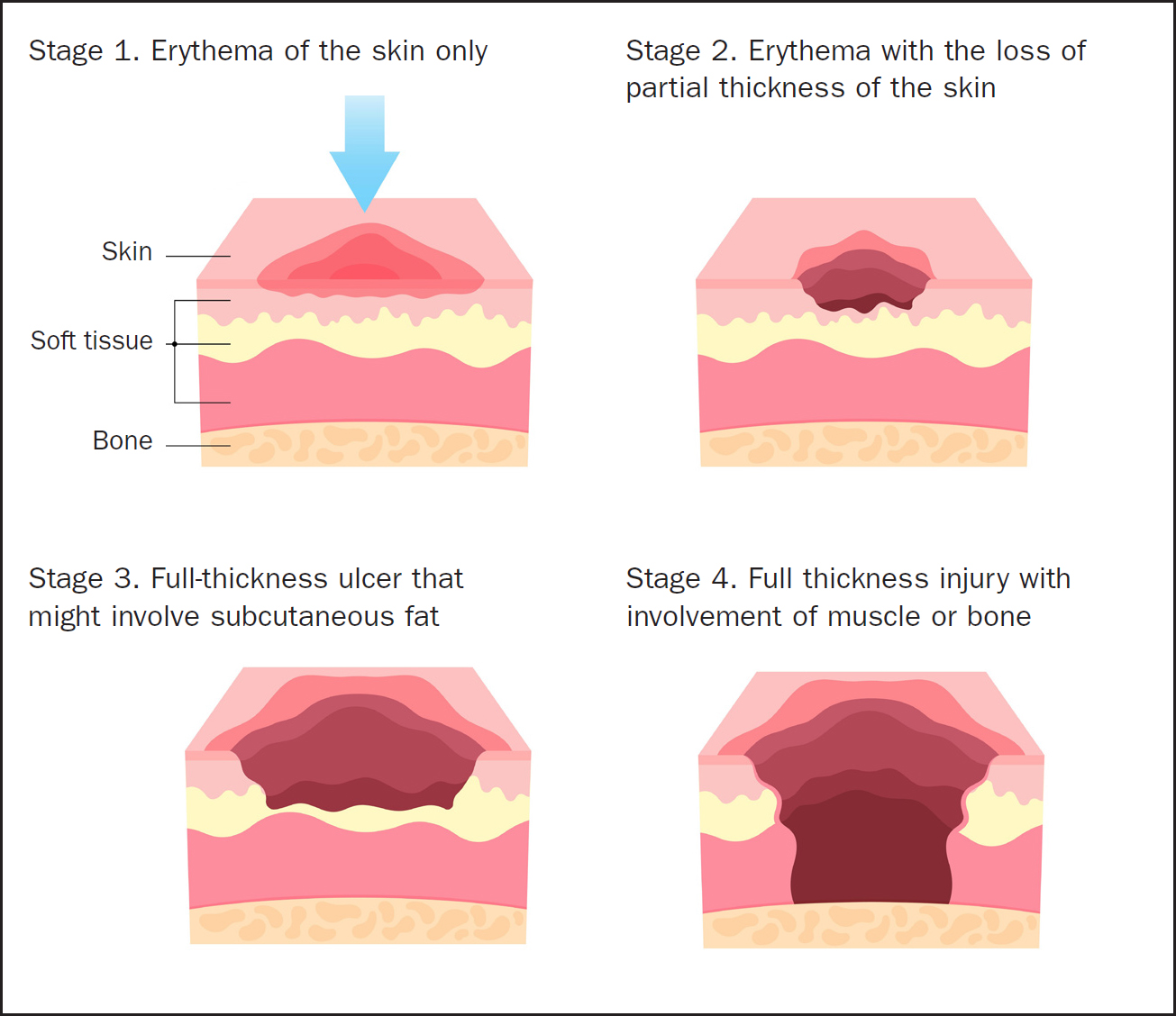
Pressure injuries are categorised into stages 1–4. It is important to understand the structure of the skin (Figure 3) in order to understand the four stages (Figure 4).
The National Wound Care Strategy Programme (NWCSP) (Fletcher, 2023;) has dropped the terms ‘unstageable’ and ‘suspected deep tissue’ injury from the UK classification of pressure damage (NWCSP, 2024). However, concerns have been raised by practitioners about the changes, prompting the Wound Care Association UK to seek a discussion with the NWCSP and to recommend members that no changes be made to the categorisation of pressure ulcers in the interim until the NWCSP has provided clarification (see Wound Care Alliance UK survey, pages S16–S22).
Symptoms
When pressure injury occurs, the skin may blister or become discoloured.
However, a pressure injury will not change colour when pressed – this change is called blanching – or may be slow to blanch (Kirman, 2024). Normal, non-injured skin in a healthy patient with no surface capillary damage should blanch when light pressure is applied and return to normal within 2 seconds of this being released (McGuire et al, 2023).
Pressure injuries present as red, blue or black, depending on skin colour; when touched, the area can feel spongy or hard and may have localised heat (Kottner et al, 2020). Patients may report itching or feel some pain in the early stages of a pressure injury; however, it has been reported that at stage 4, while the ulcer looks very painful, the patient often feels little to no pain as the full-thickness injury means that the nerves are damaged (Chaboyer et al, 2018). Although patients with a stage 4 pressure injury on their sacrum may report no pain, it is not uncommon for the person cleaning and dressing it to be able to feel bone.
Once an open wound has developed, if left untreated, it can worsen or become infected, eventually reaching the deep layers of tissue or bone (Lin et al, 2020). Staff should also monitor thje area for necrosis. Necrosis is irreversible cell injury and eventual cell death, which often presents as black in colour (NICE, 2024).
Prevention
Regular pressure area care is important. This includes repositioning a patient who cannot relieve their own pressure areas at a minimum of 4-hourly intervals (Gillespie et al 2020). For any patients deemed to be at risk this should be shortened to 1- or 2-hourly (NICE, 2024). At-risk patients include but are not limited to those with a very low BMI, spinal injury or reduced mobility and those in neurological or critical care. A Waterlow score must be used to identify if a patient is at risk (Waterlow, 1985).
Pressure-relieving equipment should be used for patients deemed to be at risk (NICE, 2024). Aids can be used in beds or on chairs: these work by redistributing the pressure and are effective when used correctly. If a patient is sat in a chair, they should be encouraged or assisted to stand every 2 hours to relieve pressure (Chaboyer et al, 2018).
Maintaining a healthy diet can also help prevent pressure injuries, so patients should be referred to a dietitian if malnourished (Lin et al, 2020).
It is essential to keep the skin clean and dry to prevent pressure injury. This is especially true for people who have incontinence, and the right amount of creams and lotions should be applied to avoid too much moisture (Informed Health, 2022).
Preventive and treatment strategies for pressure injuries are shown in Table 2.
| Strategy | Description | Examples | Considerations |
|---|---|---|---|
| Prevention | Strategies aimed at avoiding the development of pressure injuries through risk assessment, skin care and nutritional support |
|
|
| Pressure-relieving devices | Devices designed to reduce pressure on vulnerable areas of the body, thereby reducing the risk of pressure injuries |
|
|
| Skin care | Regimens focused on maintaining skin integrity and preventing damage from moisture, pressure and shear |
|
|
| Nutritional support | Ensuring adequate nutrition to support skin integrity and promote healing |
|
|
| Advanced treatments | The use of cutting‑edge technologies and materials to promote the healing of established pressure injuries |
|
|
| Rehabilitation and support | Services aimed at aiding recovery and preventing recurrence through physical, psychological and educational interventions |
|
|
Source: National Institute of Health and Care Excellence, 2014
National Institute for Health and Care Excellence quality standards
NICE (2015) quality standards identify high-priority areas for quality improvement in a specific area of care or service area; each standard consists of a prioritised set of specific, concise and measurable statements. The NICE (2024) quality standards for pressure ulcers state that:
Assessment tools
The Waterlow scale is a validated tool developed in 1985 by Judy Waterlow. It allows practitioners to work out a patient's level of risk for developing a pressure injury and should be done on admission, then weekly for every patient on change of inpatient area or on change in condition. It should also be recalculated after surgery (Waterlow, 1985). The scale is used to calculates a score, taking into account the patient's weight, sex, age, skin condition, continence, mobility and special risks including neurological deficit and tissue malnutrition.
The Waterlow score can be used alongside other tools such as the Malnutrition Universal Screening Tool (MUST) to inform patients’ risks (BAPEN, 2011). The score is used to understand what level of assistance a patient needs and which specialist equipment should be used to help prevent the development of a pressure injury. The MUST score has only five aspects and is designed to identify whether a patient is malnourished or at risk of this. The score is in range of 0–3 and has five stages. The Braden scale for predicting pressure ulcer risk is also a useful tool (Bergstrom et al, 1987).
Assessment tools are outlined in Table 3.
| Assessment tool | Scoring system | Key parameters evaluated | Strengths | Limitations |
|---|---|---|---|---|
| Waterlow score | Numeric score based on risk factors. Incorporates MUST score | Skin type, mobility, sex, age, BMI, specific risk factors | Comprehensive, widely used, includes a broad range of risk factors | May be complex to use, requires regular updating and specific patient details, eg BMI and weight loss |
| MUST (Malnutrition Universal Screening Tool) | Numeric score based on BMI, unintentional weight loss and effect of acute disease on intake for >5 days | Nutritional status, weight loss, effect of disease on intake | Simple to use, focuses on nutritional risk, applicable in various settings | More focused on nutritional status; may need to be used alongside other tools |
| Braden scale | Numeric score based on sensory perception, moisture, activity, mobility, nutrition, friction and shear | Skin integrity and risk factors related to mobility and nutrition | Easy to administer, well validated, includes sensory perception | Might not cover all specific risks, especially in complex cases |
Sources: Waterlow, 1985; BAPEN, 2011; Bergstrom et al, 1987
Assessing a pressure injury
Assessment of a pressure injury involves the following steps:
There are many aetiologies of skin wounds and ulcers, so it is important that any injury found is assessed to determine the type of injury. The differential diagnosis of the skin injury needs to be determined. Examples of injury include pressure ulcers, skin tears, moisture-associated skin lesions and injury from shear or friction (Lin et al, 2020). The mechanical forces of shear and friction contribute to the formation of pressure ulcers, but only shear can be seen at the skin level, whereas friction damages the tissue below the skin (Chaboyer et al, 2018).
Any injury that causes the skin to break has associated risk factors. Where there is no blood, there are also no white blood cells, so the main risk factors include infection, which, in severe cases, can lead to sepsis (Centers for Disease Control and Prevention, 2024). The two most susceptible sites for developing infection are the coccyx area and the buttocks, with heightened risk if the patient is incontinent. Sepsis is the body's extreme reaction to infection; it is a life-threatening emergency and requires immediate care (NICE, 20241).
Caring for a pressure injury
On first finding a pressure injury, it is crucial to prevent it from becoming worse. A referral must be made to the tissue viability team so a specialist nurse can assess the patient and make a plan of care. They will also provide any dressings or equipment needed.
The injured area should be kept clean and dry and, if there is an open wound, this should be dressed using aseptic technique with washed hands and personal protective equipment, including gloves and apron to prevent infection (Kottner et al, 2020).
Dressings that are often used include ribbon packing, as well as those containing honey or silver to aid healing and help prevent infection (Lin et al, 2020). If infection is suspected, a wound swab should be sent for analysis and the patient started on antibiotics (Chaboyer et al, 2018). Creams and ointments can also be used to protect the skin.
Documentation is imperative in health care, and all patients requiring pressure area care should have a pressure area chart (Department of Health and Social Care, 2024). Each positional change should be documented along with regular skin checks and notes made on pressure injuries. Body mapping can also be useful. At stages 3 and 4, surgical intervention may be required for debridement (Kirman, 2024).
These injuries go through the same four stages of healing as any other wound: haemostasis; inflammation; proliferation; and remodelling (Lin et al, 2020). If a wound does not decrease in size by 50% within 4 weeks, it has a 91% chance of not healing in 12 weeks, thus becoming chronic, meaning an extended stay for the patient and additional costs (Wound Source, 2021).
Recommendations for practice
Nurses can review local policies for preventing and treating pressure injuries/ulcers and consult national policies, including the NICE (2014) clinical guideline on pressure ulcers prevention and management. Practitioners can also speak with their tissue viability nurse for specialist advice.
It is also beneficial to involve other members of the multidisciplinary team, such as physiotherapists, dietitians and speech and language therapists, to ensure robust holistic patient care (Lin et al, 2020; NICE, 2024).
Conclusion
Pressure injuries are one of the most prevalent and costly wounds healthcare staff manage. They can lead to extended hospital stays and complications such as infection can impact a patient's recovery and increase mortality. It is crucial to provide gold-standard care and use an evidence-based approach in the prevention and treatment of pressure injuries to achieve the best possible outcomes for patients and other service users. Early specialist care can significantly enhance patients’ chances of recovery and ensure a good quality of life.