

An estimated 44% of the 3.8 million people with a wound managed in the UK have an acute wound such as an abscess, burn or surgical, open or traumatic wound (Guest et al, 2020). Of all acute wounds, surgical wounds are the most commonly managed type in the UK (47%) (Guest et al, 2020). The annual costs to the NHS of caring for surgical wounds in 2017–2018 has been reported to be about £546 million of the total £8.3 billion expenditure on wound management (Guest et al, 2020).
The World Health Organization (2018) defines a surgical wound as one that is created when an incision is made with a scalpel or other sharp cutting device then closed in the operating room by suture, staple, adhesive tape or glue, resulting in close approximation of the skin edges. Most surgical wounds are expected to heal without complications. However, some will go on to dehisce, which often makes them difficult and expensive to treat. This can lead to an increased risk of surgical site infection (SSI), delayed healing and poor scar formation, as well as harm to the patient's mental health, social life and physical functioning (Dowsett et al, 2018).
Surgical wounds with complications are the most commonly managed wound type in some clinical care settings and are one of the leading global causes of morbidity following surgery and account for a growing percentage of patients seen in outpatient wound clinics and in the home (Conway et al, 2022). A surgical wound complication is defined as a disruption to normal incisional wound healing following surgery. Surgical wound complications delay healing, and continue to pose a challenge to health professionals (Conway et al, 2020).
Surgical wound complications include SSIs, surgical wound dehiscence, hypergranulation, periwound maceration, scarring, medical adhesive-related skin injury (Sandy-Hodgetts et al, 2020), seroma, haematoma, delayed healing and incisional hernia (Downie et al, 2020).
A key element in preventing surgical wound complications is the postoperative/surgical dressing (Breisinger et al, 2022). The purpose of the surgical dressing is to cover and protect the wound from external contaminants, reduce the risk of infection and support wound healing (Downie et al, 2020).
An international meeting of surgeons to discuss incision care and dressing selection for surgical wounds identified that dressings should ideally not impede patients' movement, provide elasticity to avoid pulling or blistering, have good adherence, prevent exudate leakage from the dressing to the periwound skin, protect the surrounding skin to the reduce the risk of blistering or irritation, provide patient comfort with minimal discomfort or pain during removal, have a good seal/barrier function, eliminate ‘dead space’ between the wound bed and the dressing to avoid exudate pooling and possess transparent dressing borders to allow the surrounding skin to be observed (Sandy-Hodgetts et al, 2024).
The dressing evaluated in the present study is the Curapor surgical dressing (Lohmann & Rauscher), which is a newer version of an existing, CE-marked sterile surgical dressing. This newer version uses improved, more modern versions of the materials in the original product. It consists of a white, non-woven polyester base material, skin-friendly polyacrylate adhesive and a wound pad (an absorbent layer made of viscose and polyethylene/polypropylene and wound contact layer made from polyethylene).
The aim of this survey was to collect health professionals' assessments of the dressing's performance, quality, ease of application and usability and so validate the claims for Curapor and compare a few features with the existing version of the dressing.
Methods
The survey was designed to collect subjective observations by clinicians about the technical characteristics of the dressing, which is intended for postoperative, acute and superficial wound care as well as cuts and lacerations. All of these wound types were included in the study.
The observation was conducted through a prospective, cross-sectional quantitative survey of nurses and doctors in hospital inpatient and outpatient departments, GP practices and wound care specialist centres in Germany to collect feedback on their routine experiences of using Curapor surgical dressings and the number of patients they treated for each endpoint of the survey. The health professionals were experienced wound care practitioners accustomed to assessing wound dressings. They were approached by Lohmann & Rauscher sales representatives about taking part.
A convenience sampling method was adopted with the minimum sample size not having being determined statistically. The patients who required a post-surgical dressing were selected by the health professionals.
The study endpoints were derived from the design specifications of the dressings, in line with characteristics for ideal surgical dressings identified in a recent consensus paper (Sandy-Hodgetts et al (2024). The dressings were employed according to their certified intended use, under paragraph 23b of the German Medical Devices Act.
The study inclusion criterion was the presence of a wound requiring a surgical wound dressing. No other inclusion or exclusion criteria were set.
Approval by an ethics committee was not required as the study comes under the provisions of paragraph 23b of the German Medical Device Act. Gaining informed consent from patients was not deemed necessary as no personal data were obtained from them nor were they subjected to any procedure beyond routine dressing use. All the health professionals were required to sign a confidentiality agreement. This agreement included the nature of the activity and its results; mandatory reports to authorities etc were explicitly excluded.
Participants received a small compensation, depending on the number of patients they involved.
The survey was performed in compliance with the study protocol (not published) and the sponsor's standard operating procedures to ensure adherence to good clinical practice.
The survey ran between June 2015 and January 2017 with no follow-up period.
A clinical research associate, who was hired for the study, drove to every centre, gave out paper questionnaires by hand and trained the practitioners on the product and completing the survey.
The questionnaire collected assessments of the dressing's primary parameters of performance, quality, ease of application and usability. Assessments were scored using three questions, with higher scores given to the worst outcomes. These questions were: six-point Likert scales (very good=1, good=2, satisfactory=3, sufficient=4, deficient=5, insufficient=6); three-point Likert scales (light/better/very soft=1, medium/equal/soft=2, severe/worse/less soft=3); and dichotomous questions (yes/no). The characteristics or claims were considered passed in cases where mean value was <3.5 for a 6-point scale, <2 for a 3-point scale and >50% for a dichotomous question.
The performance and quality of the dressing were evaluated through parameters of gentleness on the skin of the adhesive, the non-woven material and wound pad, conformability, tear strength, adhesion to the wound, absorption capacity, formation of tape blisters on the skin, tendency to roll up, adhesion to the skin, prevention of maceration, softness and permeability.
Ease of application was assessed on whether the dressing was easy to apply and how well it compared to the previous version of the dressing. The usability of the dressing was assessed through questions on user-friendliness, pain experienced on dressing removal and change, dressing adhesive residue, patient acceptance and overall comfort levels.
The data from the survey were inputted manually into a database and verification was carried out by an independent reviewer. Explorative-descriptive statistical analysis was used for data evaluation. Statistical significance was determined using the Fisher's exact test where P<0.05 was considered statistically significant. All the study records were stored in a secure, password-protected location by the sponsor.
Results
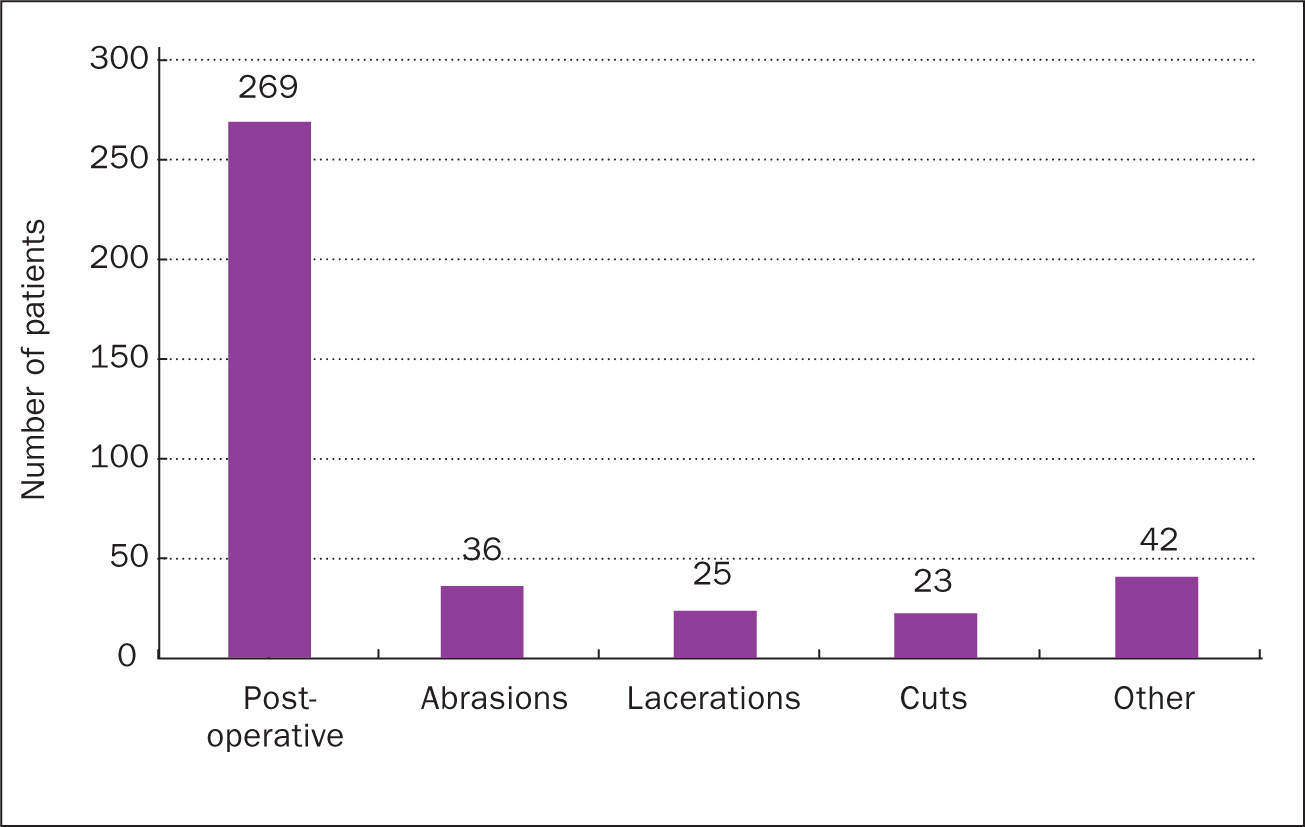
The survey was completed by 21 doctors and 24 nurses, who treated a total of 394 patients, a mean of 8.76 patients per health professional. The majority of the patients (90%) were treated for acute wounds such as postoperative wounds (68%; n=269), abrasions (9%; n=36), lacerations (6%; n=25) and cuts (6%; n=23), while 10% were treated for other superficial wounds (n=41) such as skin disorders, diabetic foot ulcers, abscesses, leg ulcers or puncture wounds (Figure 1). The abdomen, arm, hand, knee and foot were the most common sites for dressing use (Figure 2). The average time for which the dressings remained on the wound was 2.08±0.86 days.

When assessed for performance and quality on a scale of 1-6, the dressing was rated as good for its capacity to absorb light exudate (mean 1.64). The dressing was rated as satisfactory regarding absorption of medium exudate (mean 2.60). In the dichotomous questions (yes/no), the dressing edges were recorded not to have rolled up in 89% of the patients and 98.9% of patients had no tape blisters.
Only one practitioner reported X-rays being taken with Curapor in place, which happened with three patients. There was no impairment in the image quality.
No itching caused by the dressing was reported for 93.6% of patients. Maceration occurred in 14 (4%) of patients. Moisture vapour was transmitted successfully through the dressing, avoiding any moisture pooling, in 96% of patients. Impairment of skin appearance (maceration (n=10), skin irritation (n=2), pustules (n=3), reddening (n=1), risk of blisters and infection (n=2) were observed in 4% (n=16) of patients, which resulted from waterlogging caused by excessive moisture under the dressing. Infection was not seen during the survey assessments.
Concerning application and usability, the dressing was rated as very good regarding general comfort (mean=1.53 on the 6-point scale). The health professionals reported that all the patients found the non-woven material and wound pad of the dressing to be either soft (60%) or very soft (40%) on the 3-point scale. The adherence of the wound pad to the wound bed was either light (50%) or medium (50%) in the 5.08% (n=20) of patients whose wound pad adhered to the wound. The ease of positioning of the dressing to the wound location (mean=1.47), the speed (mean=1.58) and simplicity (n=1.51) of dressing application were rated as very good on the 6-point scale.
In 94% of patients, the dressing stayed securely in place and did not slip. Displacement occurred in 6% of the patients; these patients were treated by 20% of the practitioners – 80% had no patients where the dressing slipped.
The average wear time of dressings that did slip was 31.4 hours. No significant differences (P<0.05) were found between wound location and incidence of slippage.
During dressing removal, no severe or long-term redness was reported in 96.95% of patients; there was no dressing residue on the wound in 98.45%, no pain in 88.07% and no dressing tears in 98.99%. No wound lesions were recorded using the yes/no scale in 97.9% of patients.
The study endpoints and results are shown in Table 1.
| Parameter* | Mean value |
|---|---|
| Adhesion of dressing to the skin | 1.40 |
| Capacity to absorb light exudate | 1.64 |
| Capacity to absorb medium exudate | 2.60 |
| Ease of positioning of the dressing on the wound | 1.47 |
| Handling of the dressing with regards to simplicity | 1.51 |
| Handling of the dressing with regards to speed | 1.58 |
| Patients' overall comfort levels on wearing the dressing | 1.53 |
Discussion
Dressings with a gentle adhesive that avoid blisters and periwound injuries, that manage exudate well and allow the patient to freely move are recommended to facilitate undisturbed wound healing (Stryja et al, 2020).
Blistering and SSIs are common postoperative complications. To reduce SSI risk, it is now generally accepted that surgical dressings should be kept undisturbed for a minimum of 48 hours after surgery and up to 4 days if possible, unless leakage occurs or symptoms change (Stryja et al, 2020). Blistering has been identified as the most common type of skin damage caused by post-surgical dressings (Ousey et al, 2023) with the strength of the dressing's adhesive implicated in some cases of this.
A study of 416 patients with postoperative wounds (Arroyo et al, 2015) compared the performance of a transparent surgical dressing with polyurethane film and pad (Post-Op Visible, Smith and Nephew) versus a gauze and tape dressing regarding the incidence of SSIs, injury to the periwound skin and patient and clinician satisfaction. Blistering occurred in 8.7% of wounds under gauze and tape and in 2.3% under the film-plus-pad dressing. Studies on an earlier, opaque version of the Post-Op dressing reported incidences of blistering of 6% (Cosker et al, 2005) and 9% (Jester et al, 2000). The proportion of patients in whom tape blistering under Curapor was reported was 2% (n=7), with bleeding being reported in one patient.
Arroyo et al (2015) reported erythema rates of 12.2% in the gauze group and 2% in the film-and-pad group. On removal of Curapor, severe or long-term erythema was reported in 3% (n=12) of patients; five of these were deemed to have resulted from an allergic reaction.
The average number of dressing changes per week with Curapor was 3.36, which is comparable to previous studies of post-surgical dressings (Roberts and Ousey, 2013; Arroyo et al, 2015).
In common with other studies on clinicians' evaluation of the performance of post-surgical dressings (Bielby et al, 2011; Roberts and Ousey, 2013; Arroyo et al, 2015), the clinical users' assessments were subjective and collected via Likert scales. However, in this study, the data were supported by quantification of the patients in whom the endpoints were observed; the practitioners were able to indicate, for example, how many of the patients had a successful result and how many did not.
Limitations
Survey methodology is an established approach for obtaining insights from real-world situations and clinical outcomes but is subject to limitations that would be expected in any non-comparative or non-randomised clinical study.
The outcomes measured were the perceptions of the clinicians of the performance of the dressings and were not collected per individual patient. Analysis was therefore not possible per wound characteristic. Future surveys could report data according to wound types.
The opinions of the health professionals completing the survey may be subject to bias as the questionnaire was not pre-tested and the survey tool was not validated.
The assessment of dressing performance by the practitioners was subjective, and expressed on a numeric Likert scales with no intermediate scores.
As the study was carried out in a real-world context and minimising the reporting burden was a concern, no independent assessors were used to cross-check health professionals' reports on performance.
Including wounds' infection status and incidence of any SSIs would have facilitated a comparison of results with the literature.
Conclusions
As the first line of defence for a new wound, post-surgical dressings have to be designed to balance and combine competing performance characteristics. To remain in situ and avoid incidents of blistering, maceration and erythema, dressings must have an effective adhesive which, at the same time, ensures a high level of comfort, flexibility and gentleness on the skin and sufficient permeability to allow for the moisture and vapour transfer of excess exudate or passage of fluid into a secondary cover dressing.
In this study, the average dressing wear time of 2.08 days and the high scores for performance in the features critical to ease of use and patient comfort demonstrate that Curapor meets the multiple requirements for a post-surgical dressing.