

The first article in this two-part series focused on the clinical awareness of infiltration and extravasation (Barton, 2024), particularly associated with non-systemic anti-cancer therapies (non-SACT) and introduced ivWatch technology by sharing data from a clinical trial. ivWatch was trialled in an outpatient infusion unit in a large acute hospital in England between August 2023 and January 2024. The results of the trial were compelling: 2254 infusion sites were monitored with ivWatch, detecting 122 red alerts and a further 59 yellow alerts, averting a total of 181 infiltration and extravasation injuries. This follow-up article demonstrates the benefits of using ivWatch by examining the economic and public burden of infiltration and extravasation injuries in more detail.
Complications arising for intravenous (IV) therapy can be serious and sometimes life changing (Nickel et al, 2024). Historically, complications associated with IV therapy and vascular access devices (VADs) used to administer IV infusions have predominantly focused on infection, thrombosis and drug reactions, including anaphylaxis. Less well-known complications such as infiltration and extravasation are now being more widely discussed in the literature, most recently by the National Infusion and Vascular Access Society (NIVAS).
Historically, extravasation has been considered a concerning complication in oncology, associated with the administration of IV systemic anti-cancer therapies (SACTs), especially anthracycline cytotoxics. Extravasation awareness is an essential element of SACT training for nurses and is included in their annual updates (Casey et al, 2023). The same level of training and awareness is not placed on non-SACT IV therapy practice, yet this is where most extravasations occur.
It is important to note that the dangers of extravasation and infiltration are not as widely known as other patient harm risks and, as a result, are often not recognised in clinical practice. Because of this, the costs cited in this article are only a partial representation of potentially staggering liabilities affecting healthcare organisations due to continued misdiagnosis or failure to properly identify extravasation and infiltration events as they occur.
NHS Resolution (2022) has published a breakdown of the cost of claims for infiltration and extravasation against the NHS it received between 1 April 2010 until 1 December 2021. The figures show that over these 10 years NHS Resolution received 467 claims from patients who had suffered such injuries. Of this number, 214 were settled with damages and 112 closed with nil damages, with the cost to the NHS reaching £16 million. This sum includes payments for claimant legal costs, NHS legal costs and damages.
Publication of these figures coincided with the launch of the national campaign from NIVAS to raise awareness about infiltration and extravasation in the UK, which included the recently published national toolkit (NIVAS, 2024). This aims to improve the awareness, prevention, recognition, treatment, follow-up and reporting of infiltration and extravasation injuries, in particular those associated with non-IV SACTs, although SACT is an important element of the toolkit.
The true financial cost of infiltration and extravasation within the NHS is difficult to quantify. Poor awareness and recognition of extravasations when they occur has led to misdiagnosis of these injuries, leading to missed opportunities to incident report locally. This has resulted in a lack of local and national reporting data, making it impossible to know the true rate of infiltration and extravasation including the financial cost. A national change in awareness and prevention is leading the way, with the support of the NIVAS national infiltration and extravasation toolkit (NIVAS 2024). Despite the absence of national data, it is possible to approximate the economic burden of infiltration and extravasation by looking at local case studies from NHS organisations.
Awareness and recognition rely on health professionals knowing how to differentiate between infiltration and extravasation. Infiltration is the inadvertent administration of IV therapy or fluids into the tissue surrounding a VAD (Kim et al, 2020). Although infiltrations can cause harm to the patient, the severity of injury is usually not serious unless large volumes of fluid are involved, in which case compartment syndrome is a risk. Non-vesicant therapies such as IV iron preparations can also cause harm, leading to permanent staining of the subcutaneous tissue and skin, which can lead to psychological trauma and negative body-image issues.
Extravasation occurs when IV therapy infiltrates the surrounding tissue, particularly when the therapy or drug involved is a vesicant (David et al, 2020). A vesicant is a broad term describing a group of drugs and IV therapies that can cause irritation or damage to skin, tissues, veins and cells (Ong and Van Gerpen, 2020). Vesicants can lead to mild localised irritation, pain, limb swelling, blistering, deep-tissue damage, cell damage, tissue necrosis, limb loss and, in extreme cases, death (Giménez Poderós et al, 2024). Vesicants broadly fall into four categories (Barton, 2024; NIVAS, 2024), which are (NIVAS, 2024):
- SACTs
- Drugs with non-physiological pH
- Vasopressors
- Hyperosmolar solutions.
Systemic anti-cancer therapy
Previously called chemotherapy, SACT can be further classified as vesicant, irritant, exfoliant, inflammatant or neutral, DNA-binding or non-DNA binding (Tanay, 2020). DNA-binding SACT such as anthracyclines and alkylating agents are capable of causing the most severe tissue damage (Khanna and Khanna, 2023). Non-DNA binding compounds such as vinca alkaloids and taxanes cause irritation, but tend to cause less severe injuries, and exfoliants cause inflammation and shedding of skin without causing underlying tissue death (Alexander, 2020).
The incidence and prevalence of cancer are increasing worldwide, with the number of patients requiring first-line chemotherapy treatment estimated to increase by 53% between 2018 and 2040, from 9.8 million to 15 million (Wilson et al, 2023). The most recent available figures for 2016-2017 show that SACT is the single biggest spend within the NHS budget and accounts for an estimated £1.4 billion a year (NHS England, 2016). The cost of SACT is growing rapidly, with an annual increases of around 8% due to rising demand and higher charges from drug companies (Royal College of Radiologists, 2023).
The cost of IV SACT per patient regimen can be as high as £30000 (Cortes et al, 2020). To mitigate this, local and national initiatives to reduce SACT drug waste have been implemented through better prescribing and dispensing practices, although there are currently no mandatory systems in place within the NHS. Incidence rates of SACT extravasation in the UK vary due to the absence of a centralised register, but have been estimated at 0.5-6% of patients receiving chemotherapy (NHS England, 2018). The amount of drug wastage and missed or delayed doses of SACT due to extravasation have not been considered in the literature, nor is this recorded nationally for the UK. Consequently, it is impossible to know the true figures, and research is therefore required to determine this.
The physical cost to patients who suffer an extravasation is better understood through published case studies. A stage 3 or 4 anthracycline extravasation injury can be life changing and every effort should be made to reduce the risk of its occurrence (Nedomansky et al, 2021). More research is needed to understand the impact of missed doses of SACT on successful cancer outcomes (Pham and Tsunoyama, 2024).
The ivWatch trial data cited and described in the previous article (Barton, 2024) demonstrates that the device can identify an infiltration around the infusion site even before the patient notices that it has occurred. When a decision to administer a vesicant using a peripheral cannula has been made, the use of ivWatch can ensure the infusion is as safe as possible (Van Rens et al, 2023; Barton, 2024). ivWatch's advanced signal processing can detect infiltrations in as little as 0.2ml of IV fluid, with an average detection volume 2–3ml (ivWatch, 2014, ivWatch, 2019).
Drugs with non-physiological pH
The data reveal that most infiltration and extravasation injuries associated with IV therapy administration occur in non-SACT practice (NHS Resolution, 2022). It is essential to know the pH of IV drugs in order to administer them safely (Manrique-Rodríguez et al, 2021). It is generally considered that a drug pH of between 5 and 9 is safe to administer via a peripheral cannula (Ong andVan Gerpen, 2020; Manrique-Rodríguez et al, 2021).
However, any drug pH outside normal blood pH range (7.35–7.45) has the potential to cause a degree of injury or irritation to tissue if an extravasation occurs. For this reason, infusion-site surveillance using ivWatch technology should be considered for all peripheral IV infusions, alongside other evidence-based practices, such as using an infusion pump, and adhering to vessel health and preservation protocols to protect the patient, their vessels and the infusion site.
Vasopressors
Vasopressor IV therapy is fundamental in the treatment of septic shock-induced hypotension because it can correct vascular tone depression and improve organ perfusion pressure (Sanchez et al, 2023). However, vasopressors are known to be high-risk vesicants which can cause significant damage to the tissue; if extravasation occurs, there is a higher risk of limb loss. (David et al, 2020). It is recommended that vasopressors are administered via central venous access (Nickel et al, 2024).
Peripheral administration of vasopressors, however, can occur in emergency situations (Tian et al, 2020; Haimovich et al, 2021). Many NHS hospitals have local protocols to administer vasopressors such as noradrenaline via a peripheral cannula in pre-defined clinical situations. The use of peripheral vasopressors has been shown to be effective in stabilising patients in septic shock long enough to admit them to a critical care unit (CCU) and place an acute central venous catheter for further vasopressor support (Tian et al, 2020; Haimovich et al, 2021), although the risk of severe extravasation injuries remains high. ivWatch can easily be used in CCUs and emergency department (ED) resuscitation rooms for just this type of infusion scenario. ivWatch can be set up quickly to monitor infusions in emergency situations.
Sepsis and risk of extravasation
In the UK, there are at least 200000 episodes of sepsis in adults each year, with up to 52000 deaths occurring as a result (Flaherty, 2022). It claims more lives than breast, bowel and prostate cancers combined, with estimated costs to the NHS of £1.5–£2 billion each year (Aschroft and Oakeshott, 2022). The UK Sepsis Trust (Daniels and Nutbeam, 2022) developed the Sepsis 6, which is a set of six tasks (enlist senior help, administer oxygen, take bloods, give IV antibiotics, consider IV fluids, monitor lactates and urine output) - to be instituted within 1 hour of identifying sepsis (Evans et al, 2021). This short time frame for treatment undoubtedly saves lives; however, the increased pressure on healthcare staff to gain IV access, administer IV antibiotics and start IV fluids within that hour can increase the risk of infiltration and extravasation. Gaining IV access can be difficult in patients who are septic due to the peripheries being shut down, which can be exacerbated in individuals who already have difficult IV access. The percentage of patients with difficult IV access across all hospital settings is estimated to be between 35% and 40% (Paterson et al, 2022).
One of most common antibiotic regimens used for firstdose administration for sepsis with unknown source in NHS hospitals is currently a combination of IV gentamycin, amoxicillin and metronidazole, providing that the patient is not allergic to penicillin. Gentamycin is a vesicant with a pH of 3.8. An extravasation of gentamycin can cause significant tissue damage. Consequently, for patients who are already at risk of infiltration and extravasation due to poor peripheral vein availability, which makes it harder to gain IV access, the administration of a vesicant can increase the risk of injury significantly.
In the ED, when managing these patients, for whom gaining central IV access can take time, using a peripheral IV and monitoring the vesicant infusion with ivWatch can not only reduce the risk of extravasation, but can also ensure that the whole infusion/dose of antibiotic is given in that first hour of sepsis.
Hyperosmolar solutions
Hyperosmolar drugs and fluids have a high osmolarity, above 600 mOsm/L (David et al, 2020), and should be given via a central VAD. Osmolarity can influence the degree of tissue injury, and the extravasation of hypertonic fluids, such as 10% dextrose or parenteral nutrition solutions, can cause skin necrosis and serious tissue damage (Stefanos et al, 2023). Dextrose solutions are rarely administered alone; other products such as potassium are often added, which can increase osmolarity even more.
Extravasation of hypertonic solutions causes a shift of fluid from inside the cells into the interstitial space, which disrupts cell function (Ong and Van Gerpen, 2020). The shift from subcutaneous cells to interstitial tissues leads to swelling and increased local pressure, which can cause acute limb compartment syndrome (Borrelli and Donohue, 2022) (Figure 1). Hyperosmolar solutions can shrink cells and collapse the internal structures, whereas hypo-osmolar solutions can swell cells and lead to cell rupture (Giménez Poderós et al, 2024). IV fluids such as 5% dextrose with 40mmol potassium can cause a significant injury if infiltration and extravasation occur.

Intravenous iron infusions
Intravenous iron preparations are not vesicant in nature; however, infiltrations of IV iron can lead to significant mental anguish due to the permanent staining of skin. When iron infusions infiltrate tissue this causes a permanent orange stain that is visible under the skin (Crowley et al, 2020). Depending on the preparation of IV iron used, an infusion of 100ml can run over as short a time as 15minutes, so by the time an infiltration is noticed most, if not all, of the infusion will have been infused. This can lead to extensive skin staining (Figure 2). There is no effective treatment for the skin staining, which is permanent. This type of injury was among those reported to NHS Resolution (2022).

A secondary consequence of IV iron infiltration is that the patient will require an additional infusion to ensure they get the prescribed amount of drug into the circulatory system. This entails the additional cost of an infusion session as an outpatient, the cost of the drug and also the equipment required. The cost of a 1000 mg dose of IV iron is £154.23 (British National Formulary (BNF), 2024), and the additional outpatient infusion appointment would be on top of this. Aside from the extra clinical cost, the patient will be nervous about having a subsequent iron infusion, because the previous one infiltrated and caused a disfiguring injury.
There is also the possibility of litigation costs. For example, between 2019 and 2024, lawyers secured large compensation settlements against NHS trusts for harm suffered as a result of iron infiltrations. A client who had suffered a permanently discoloured arm was awarded £25000 in compensation (Angwin-Thornes, 2019). In other cases, five-figure sums were awarded to two other patients who had suffered an iron infiltration (Leahy, 2021; Demetriou, 2023). The main aspects of the claim described by Demetriou (2023) centred on the fact that the trust had failed to:
- Obtain proper consent from the patient for the IV iron infusion preparation
- Failed to use the correct technique in siting the cannula before commencing the procedure in both of the patient's arms
- Failed to exercise caution to avoid leakage of iron into the patient's arm
- Failed to suspect extravasation and/or subsequently stop the infusion immediately in both arms, once it had been realised the patient had suffered an extravasation.
The common themes in these other cases of successful litigation against NHS trusts due to negligent iron infusion infiltrations (NHS Resolution, 2022) were the lack of informed consent with regard to possible iron infiltration skin staining, lack of monitoring of the infusion site, and lack of awareness that an infiltration had occurred and how to treat it (Shi et al, 2023; Barton, 2024; NIVAS, 2024). The ivWatch trial data reported in the previous article (Barton, 2024) showed the success of the technology in preventing potential harm from IV iron infiltrations, and the infusion unit has since continued to use ivWatch to monitor all IV iron infusions. From the start of the trial in August 2023 up to the time of writing this article (August 2024) there have been zero cases of iron infiltrations causing skin staining in patients with whom ivWatch was used; over this period one patient had an infiltration of iron; however in this case ivWatch was not used.
Challenges facing health care
In 2023, the Health Foundation published a paper outlining nine challenges facing health care in the UK (Dunn et al, 2023). Among these were the fact that patients are living longer but in many cases with major long-term health conditions, many of which are likely to require the use of IV therapies.
Patients surviving conditions such as cancer often require long-term IV infusions such as zoledronic acid, which is a vesicant (Salbaş et al, 2018), long after they have had the all-clear from their oncologist. Individuals living longer due to having lifelong infusions of high-cost drugs such as monoclonal antibodies or IV immunoglobulin are at increased risk of infiltration and extravasation. This should be even more of a motivation to adopt and embed technology, such as ivWatch, for infusion site surveillance, to enable cost savings in the long term, helping avoid drug wastage and extravasation injuries. In 2022–2023, the highest spend was on high-cost drugs, categorised under Malignant Disease and Immunosuppression in the BNF: £3.26 billion was expended on items dispensed in the community. This was the net ingredient cost before any discounts, with £3.09 billion being spent on medicines issued and dispensed in hospitals (NHS Business Services Authority, 2023).
The financial cost
The NHS tariff for 2022–2023, for an inpatient ward bed day, was £320.00 (NHS England, 2023; 2024). This includes all the basic nursing care and clinical interventions, food and estate costs. Other costs such as specialist treatment, surgical interventions and high-cost drugs are calculated separately. When a patient has a serious infiltration or extravasation, an extended hospital stay is often indicated, and outpatient follow-up and community treatment are usually required after discharge. Even without additional interventions the cost is high, including increased pressure on inpatient beds.
Bed shortages alongside high occupancy rates are unsafe for patients and staff. It can increase delays in ED, delay transfer from intensive care units and between wards, and increase stress for staff and patients. Using ivWatch to monitor infusion sites can therefore help prevent infiltrations and extravasation injuries, and the ensuing costs.
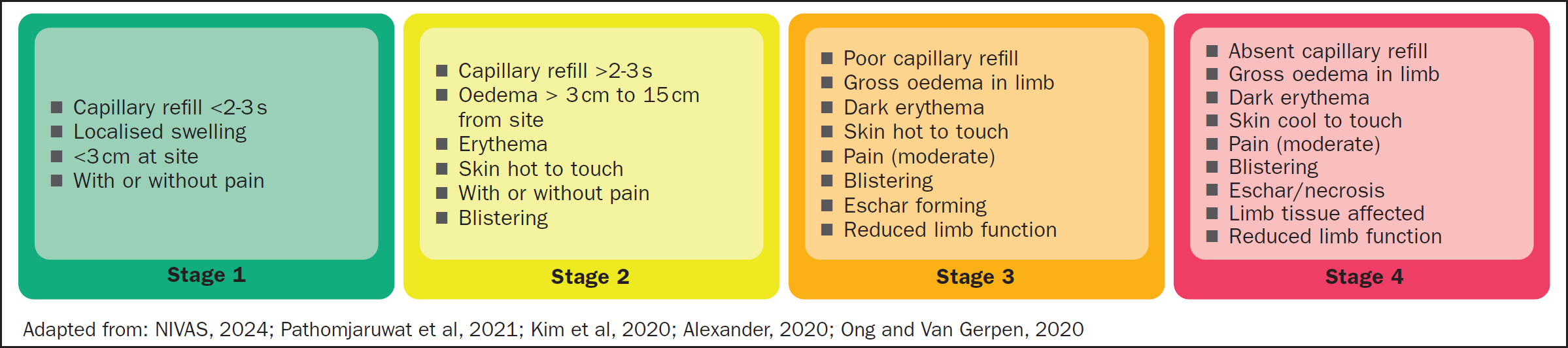
Stages of extravasation and associated costs
- Stage 1: assessment and close monitoring
- Stage 2: requires treatment action
- Stage 3 and 4: clinical emergencies requiring urgent action (Figure 3).
The cost of treating an infiltration or extravasation can vary, and depends on the stage of injury and what type of treatment is required. Other factors to consider are whether the patient is an inpatient or whether they have been discharged, with the injury developing in the community. For someone who attends an urgent care centre and receives the lowest level of investigation and treatment, the average cost in 2024–2025 is £91 (The Kings Fund). For an individual treated in ED who receives more complex investigations and treatment, the costs range from £137 to £445, depending on level of care required (King's Fund, 2024).
For an outpatient consultation with a consultant plastic surgeon the cost is £163 for a 30min consultation (NHS England, 2024). Using the 2023–2025 NHS Payment Scheme data (NHS England, 2024), which establish the amount payable for provision of NHS-funded secondary health care, it is possible to approximate the cost of an infiltration/extravasation.
The NHS uses individual healthcare resource groups (HRGs), which include clinically similar treatments using common levels of healthcare resources, to produce a tariffor payment for treatment provided by NHS trusts (Amies-Cull et al, 2023) (Table 1). HRGs for plastic surgery for skin conditions (or injuries) are categorised depending on patient age (under/over 18 years old) into minor skin procedures (£593–£1074) including excision of skin lesions; full-thickness grafts and local flaps; intermediate skin procedures (£1045–£1362) including abdominoplasty and tissue expanders; and major skin procedures (£2326–£11916) including skin debridement or split-skin grafting (Seaward et al, 2007).
| Healthcare resource groups are standard groupings of clinically similar treatments that use common levels of healthcare resource | Outpatient procedure | Combined day case/ordinary elective spend (£) | Ordinary elective long-stay trim point (days) | Non-elective spell (£) | Non-elective long stay trim point (days) | Per day long-stay payment for days exceeding trim point |
|---|---|---|---|---|---|---|
| Very major skin procedures | – | £2879 | 5 Days | £19200 | 61 Days | £308 |
| Major skin procedures | £175 | £2326 | 5 Days | £11916 | 45 Days | £308 |
| Intermediate skin procedures, 19 years and over | £283 | £1045 | 5 Days | £1105 | 5 Days | £308 |
| Intermediate skin procedures, 18 years and unde | £302 | £1116 | 5 Days | £1362 | 5 Days | £308 |
| Minor skin procedures, 19 years and over | £143 | £593 | 5 Days | £627 | 5 Days | £308 |
| Minor skin procedures, 18 years and under | £157 | £949 | 5 Days | £1,074 | 5 Days | £308 |
For patients who remain in hospital beyond an expected length of stay for clinical reasons, there is a reimbursement in addition to the unit price called a ‘long-stay payment’ (sometimes referred to as ‘excess bed day payment’). The long-stay payment applies at a daily rate where length of stay of the spell exceeds a ‘trim point’ specific to the healthcare resource groups (HRGs). A long-stay payment on a daily rate basis applies to all HRGs where length of stay of the spell exceeds a specified trim point specific to the HRG and point of delivery (NHS England, 2024)
Stages 3 or 4 extravasation injuries or infiltration related compartment syndromes are likely to require surgical skin procedures, which will depend on the degree of tissue damage, with associated high costs of repairing such injuries.
Case studies
The following case studies outline recent extravasation injuries sustained in one acute NHS foundation hospital in England. All these extravasations were investigated and changes in practice made to reduce the risk in future. Had ivWatch had been used to monitor these infusions, this may have prevented these injuries. In the case of the iron infusion used at the hospital, there have been no infiltrations while using ivWatch in the infusion unit in the hospital.
Case study 1: calcium chloride extravasation
A 78-year-old patient was seen in the ED. He was feeling unwell with a pyrexia and had shortness of breath; additionally, he had a chronic left leg ulcer that was infected. He lived independently alone, despite having had a previous below-right-knee amputation, and he used a wheelchair. When he was admitted to the ED, a 20-gauge peripheral cannula was placed into the right antecubital fossa and bloods were taken.
The bloods showed a potassium level of 8.8 mmol/L (normal range 3.4–4.5 mmol/L), blood pH was 7.166 (normal range 7.35–7.45), and lactate level 2.9 (normal range 0.5–2.2 mmol/L); he had a C-reactive protein level of 208 (normal range 0–5 mg/L) and was in renal failure, with an estimated glomerular filtration rate (eGFR) of 6 (normal range 60–120 ml/min). A hyperkalaemia, or elevated level of potassium in the blood, was diagnosed in addition to sepsis and acute renal failure. Left untreated, hyperkalaemia can cause life-threatening cardiac arrhythmias, muscle weakness or paralysis,(Palmer et al, 2021).
Intravenous antibiotics were prescribed and given, alongside IV calcium chloride to reduce the risk of ventricular fibrillation associated with hyperkalaemia. Due to its high osmolarity, 2040 mOsm/L, calcium chloride is considered a vesicant capable of causing severe vessel irritation, skin blistering and tissue destruction (Ong and Van Gerpen, 2020). The patient was given 10ml of calcium chloride 10% via a slow bolus injection; as soon as the drug was administered he complained of pain and the nurse noticed localised swelling around the cannula site. The nurse recognised an infiltration, reporting this to the doctor. The cannula was removed, a new one sited in the left arm and a repeat bolus of IV calcium chloride 10% administered with no complication to ensure the patient received the full-dose of calcium chloride.
Although the infiltration of the the first dose of calcium chloride was documented, it was unclear whether the staff involved understood the terminology used. It was not recorded that calcium chloride 10% was a vesicant or that an extravasation had occurred, and no action was taken directly at that time to minimise the risk of tissue damage.
The patient was admitted from the ED to a level 1 medical unit where the hyperkalaemia improved, as did the acute renal failure. However, after 48 hours the skin and tissue around the right antecubital fossa started to blister and non-blanching erythema developed (Figure 4 a–f). The patient reported severe pain in the right arm, which limited the range of movement. At this time, cellulitis was diagnosed at the site of the peripheral cannula and antibiotics were prescribed. A referral to the vascular access team was made for a peripherally inserted central catheter (PICC) to be placed for ongoing IV therapies.
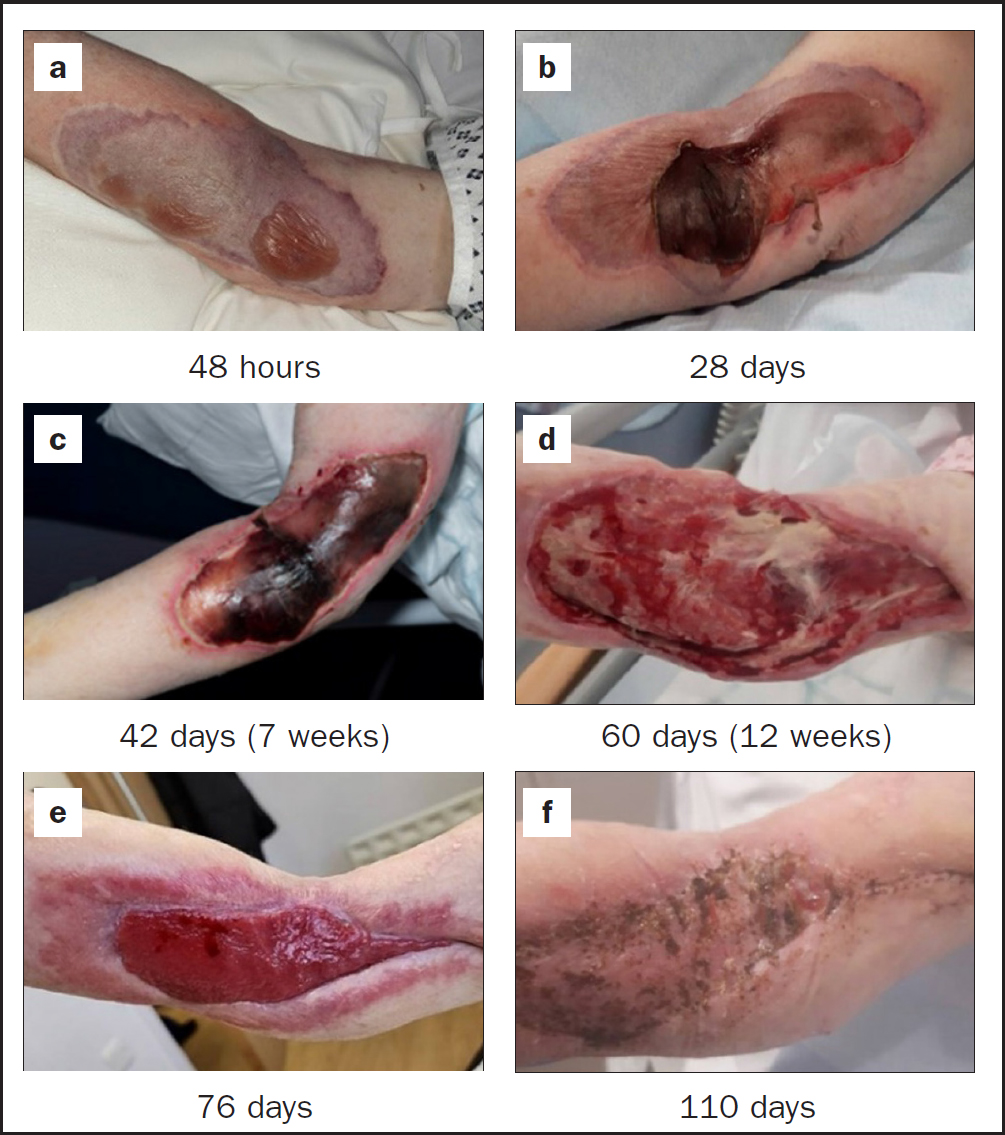
When the vascular access team reviewed the patient at 48 hours, a calcium chloride extravasation was suspected, and the patient was referred to the plastics team.
By the time of diagnosis after 48 hours post extravasation, it was too late to instigate a subcutaneous saline wash-out or to inject hyaluronidase as an antidote. The management plan from the plastics team was to allow the injury to develop and manage the patient's pain until such time as surgical debridement was indicated, with or without skin grafting. The injury continued to develop over the next 7 weeks, at which point the patient had a plastic surgical procedure to debride necrotic tissue from the injury. He remained an inpatient for a further 5 weeks until week 12, at which point a skin graft procedure was undertaken. The patient recovered from the skin grafting for a further 26 days in hospital, following which he was transferred to a community rehabilitation unit. Figure 4f shows progress of the wound after 110 days while he was in rehabilitation.
What went wrong?
The patient had three cannulas sited in the ED, which were all used appropriately;he remained stable, but had the potential to deteriorate rapidly. There was no acknowledgement that calcium chloride 10% was a vesicant or that an extravasation had even occurred. An extravasation was documented, but there was no understanding of what the term meant, so proper treatment did not begin in time.
The patient's extravasation was misdiagnosed as a cellulitis, and he was already having antibiotics for his infected leg ulcer.
What was learnt?
That this was not the first missed extravasation associated with IV calcium chloride 10%. Six significant extravasation injuries were discovered via the incident reporting system over the previous 8 months in other departments of the hospital through a review undertaken by the infusion unit, with the data showing a lack of awareness and recognition of infiltration and extravasation in the ED and the level 1 medical unit.
What was changed in practice?
Recommendations for first-line treatment for hyperkalaemia and hypocalcaemia are to administer calcium gluconate 10% where appropriate. Compared with the osmolality of around 2040 mOsm/kg for a calcium chloride ampoule, calcium gluconate is twice-hypertonic to body fluids, at 680 mOsm/kg. So, although calcium gluconate is still an irritant, it is considered to have less of a vesicant effect than calcium chloride 10% (Lindner et al, 2020). Intravenous 30ml calcium gluconate 10% is an alternative to 10ml calcium chloride 10%.
Calcium chloride is preferred in patients with cardiac arrest due to hyperkalaemia because it releases active calcium immediately upon infusion, unlike calcium gluconate, which requires hepatic metabolism to release calcium.
Education was provided to staff in the ED and in critical care, departments that are both high users of calcium chloride. Trustwide awareness-raising was also undertaken to ensure the correct dose of calcium gluconate is administered, as this has previously been an issue to ensure the correct dose of calcium gluconate 10% is given. An NHS National Patient Safety Alert (Medicines Healthcare products Regulatory Agency, 2023) has previously been issued on the potential risk of underdosing with calcium gluconate in severe hyperkalaemia – this was issued as the result of confusion in cases in which a calcium chloride 10% 10ml dose was given instead of the 30ml calcium gluconate dose.
If calcium chloride 10% is prescribed to treat hypercalcaemia, this should be given via central venous catheter due to its vesicant nature, except if the patient is in cardiac arrest, in which case any IV route is permissible (NIVAS, 2024).
What was the impact on the patient?
Despite using a wheelchair due to a previous amputation, the patient was independent prior to this episode of care. Following the extravasation the patient lost their ability to be independent with their activities of daily living. The pain and loss of function in the right arm was debilitating. After 110 days as an inpatient in the acute hospital the patient was transferred to a community rehabilitation unit. Sadly, they never returned home to live independently.
What was the estimated economic cost?
Based on available data on the cost of an NHS bed day and HRG tariffs (NHS England, 2023; 2024) the approximate cost to the NHS of this extravasation injury, without possible litigation costs was an estimated £38996. The costs break down as follows (see Table 1):
- Hospital stay of 7 weeks (49 days) at £320 per day (standard bed day cost), totalling £15680
- Plastic surgery to debride at week 7 (HRG minor skin procedure tariff, +5-day post-operative trim point, totalling £620.
- Followed by a 35-day hospital stay, at £308 per day, until skin graft procedure at week 12, totalling £10780
- Major skin procedure (HRG tariff, including 45 days post-operative trim point), totalling £11916.
Had the extravasation not occurred and the patient had not required an acute hospital stay, or had been treated promptly, the estimated treatment would have cost less than one-tenth of this amount. The patient would have remained in hospital for less than 10 days, with a total bed cost of less than £3200 (bed-day cost £320).
Case study 2: anthracycline extravasation
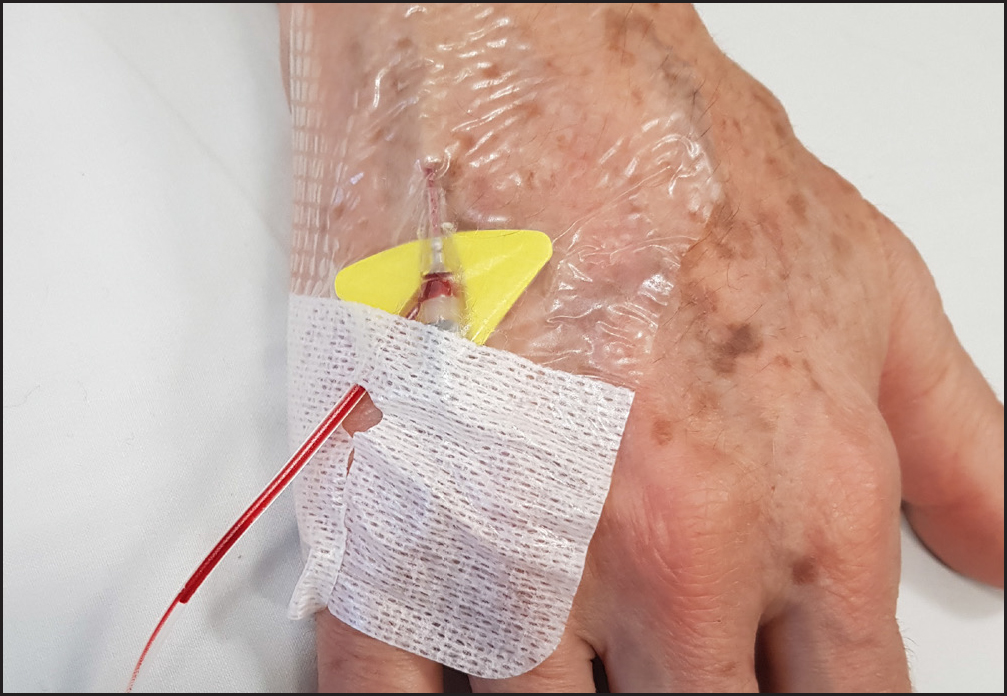
A 54-year old patient was admitted to the inpatient oncology unit to undergo SACT for treatment of diffuse large B-cell lymphoma (DLBCL). A 24-gauge cannula was placed in a vein in the back of the right hand (Figure 5) for intravenous R-Pola-CHP C2D1. This type of SACT is a combination of IV polatuzumab vedotin (irritant), rituximab (neutral), cyclophosphamide (neutral), doxorubicin (vesicant-anthracycline), and prednisone orally administered.
Prior to administration, consent was gained in line with local policy. The IV administration of the first three drugs was unremarkable; however, towards the end of the fourth and final infusion of doxorubicin, the patient reported a mild burning sensation. The SACT nurse documented that the cannula was still patent, so the remainder of the doxorubicin was administered. The next day he knocked the back of his right hand on the bedside table on the ward, causing trauma to the area where the 24-gauge peripheral cannula was sited. The cannula was removed and the patient was given analgesia.
Over the following week the back of the patient's right hand became more painful, an area of erythema developed around the peripheral cannulation site. Small fluid filled blisters formed on the skin in the area of erythema. The right hand was examined by the oncology team and the patient was referred to the plastic surgeons for review.
The plastics team examined the right hand, they took a brief history and were told that a peripheral cannula had been sited on the hand, and that the patient had experienced a contusion to the hand while the cannula was in situ. The plastics team were not told about the potential SACT extravasation because at that time an extravasation diagnosis had not been made, and they diagnosed a cannula-related trauma injury to the soft tissue caused by the contusion, recommending conservative management.
Four weeks later the patient was preparing for discharge from the acute oncology unit. A PICC had been placed for the administration of the SACT after the injury to the right hand. He was referred back to the vascular access team for review because the wound on the back of the right hand was not healing, and the tissue had become necrotic and more painful.
The vascular access team lead reviewed the patient notes and realised that this was an extravasation of R-Pola-CHP C2D1: the doxorubicin is an anthracycline known to cause extravasation injuries, which was consistent with the wound that had developed on the hand.
A referral was made back to the plastic surgeons, where the patient was reviewed in the plastics clinic after discharge home. The plastics plan was to watch and wait for the extravasation to fully evolve and consider surgical intervention at a later date, managing the patient's pain in the meantime. The SACT treatment continued, but the patient was readmitted 2 weeks later with further complications associated with the extravasation injury which had become infected. This was likely to have been due to the SACT therapy inducing neutropenia and increasing the risk of infection.
The patient remained an inpatient for 2 months, experiencing ongoing complications associated with the extravasation. He underwent skin debridement and continued to have repeated infections to the wound. Nine months after the extravasation had occurred the patient completed the SACT therapy, but has since continued to require weekly dressing changes for the extravasation wound.
What went wrong?
Because the SACT regimen contained an anthracycline, a PICC should have been placed prior to the administrant – this would have mitigated the risk of a peripheral extravasation.
There was no recognition that an extravasation had occurred by the SACT nurse, the oncology team or the plastics team, and the hand injury was treated as cannula trauma.
What was learnt?
Any patient having active SACT who presents with a similar injury needs to have extravasation ruled out fully and, until a SACT extravasating can be ruled out, this should be the primary suspect.
What was changed in practice?
For anthracycline-containing SACT the use of a centralVAD is advised and recommended due to the vesicant nature of the drug.
The patient was traumatised by the incident, losing confidence in the entire team, due to the misdiagnosis of the extravasation and conflicting clinical information provided by different staff. The hand extravasation was originally misdiagnosed as a cannula trauma injury, and there was disagreement between plastics, the SACT lead and the extravasation lead about the cause of the injury. It was as the injury developed that it became evident that this was a serious extravasation.
For any vesicant SACT administration the patient should be given the option to have a PICC.
Following this review, regular training was set up to ensure that oncology unit staff had an awareness of and were able to recognise the signs of extravasation for SACT, and this is now delivered as a mandatory annual update.
What was the impact on the patient?
The patient lost confidence in the oncology team because of the extravasation misdiagnosis at the time. Up until the second review by the plastics team he received inaccurate information from a number of different health professionals and, although this was not intentional, it was confusing.
He subsequently required multiple admissions, an operation on the right hand to debride the extravasation, and lost functionality in the hand; this has still not returned and he continues to experience pain. The 54-year-old has been left with extensive damage to the tendons and nerves of the hand.
Due to the severity of the injury, he has not been able to return to work, even 10 months after the extravasation, despite successful treatment for cancer. He is also unable to drive and has to pay for transport every week to attend the hospital for dressing changes. The injury has had major impact on his earnings potential and financial stability: on his estimation, he has lost in the region of £50000 a year after tax. Due to the injury, he is now relying on his life savings and having to plan for early retirement, but it will be more than 10 years before he can receive the state pension at 67 years of age.
What was the estimated economic cost?
Based on available data on the cost of an NHS bed day and HRG tariffs (NHS England, 2023; 2024), the approximate cost to the NHS of this extravasation injury, without litigation costs, was £6003). It is difficult to calculate the total financial costs for this case, but the additional plastic surgery procedure and the ED attendances and outpatient visits can be taken into account. Because the injury occurred when the patient was already an inpatient, there was no extra cost to treat the extravasation. The costs could be approximated as follows (see Table 1):
- HRG minor skin procedure tariff, plus 5-day post-operative trim point, totalling £620
- Plus 15 additional inpatient days after trim point (£308 per day), totalling £4620
- ED visits x2 (majors at £137), totalling £274
- Plastic surgeon consultant outpatient clinics x3 (£163 for a 30min), totalling £489.
Case study 3: peripheral vasopressor extravasation
A 30-year-old patient was admitted to the ED with a sore throat, tonsillitis, abdominal pain and chest pain. She deteriorated rapidly in the resuscitation room and was quickly intubated and taken for a CT scan. The CT of the abdomen and pelvis showed left lower-lobe pleural effusion, right-sided empyema with loculations, bilateral consolidation, thickening of the transverse colon, focal splenic lesions and moderate ascites, suspicious for an abdominal abscess. A bedside ultrasound indicated severe left ventricular (LV) dysfunction, and there was further evidence of acute liver and renal impairment.
The patient had multiple peripheral cannulas sited in ED for life-saving IV therapies. The patient was transferred to the CCU and had peripheral noradrenaline administered through a cannula in the left forearm.
The patient spent 28 days in the CCU, and 3 days into the stay developed blisters at the site of the left forearm canula. This was not recognised as an extravasation at the time. The patient had been intubated and placed on a ventilator almost immediately on admission, so had been unable to indicate if there was any pain in the left forearm. A dermatology referral was made and the patient was seen by a dermatologist who was unsure of the cause of the blisters and thought this might be a localised skin reaction, prescribing an emollient.
On the day the patient was stepped down from CCU to a surgical ward, the extravasation had not been diagnosed. However, a large area of skin, 5cm by 10cm, had become necrotic and an eschar had formed (Figure 6). The patient was referred to the vascular access team for a peripheral cannula placement with ultrasound. The vascular access nurse recognised the injury as an extravasation and initiated an investigation. At this point a referral was made to the plastics team, to surgically debride the wound.

The patient remained on the surgical unit a further 14 days recovering from the critical care admission, following which she underwent an intermediate surgical skin procedure involving a skin graft of the extravasation wound. She was finally discharged after a further 5 days. The total inpatient stay was 47 days, the extravasation injury contributed 5 additional days to this stay as the patient was critically unwell and required 42 inpatient days.
What went wrong?
The patient was critically unwell and required a critical care admission which happened very quickly after admission. Once on the CCU the patient was stabilised, and her life was saved despite being so unwell. As the patient was intubated before the noradrenaline was administered via the peripheral cannula in the left forearm, she was unable to indicate if there was any pain from the cannula site, something they undoubtedly would have been able to do had they been conscious.
There is always a risk of extravasation when vasopressors are administered peripherally. The blisters that formed a few days after the injury in this patient's case are a known sign of extravasation, but this was not recognised.
The cannula was removed while the patient was still ventilated, when it was noticed that it would not flush, and the skin and tissue around the cannula site had developed non-blanching erythema. This change was not recognised as an extravasation.
What was learnt?
When vasopressors are administered peripherally, surveillance of the cannula site is essential, especially when a patient is unable to indicate whether the cannula site is painful, for example, if they the are intubated and ventilated. Any signs of extravasation should be acted on immediately.
What was changed in practice?
Staff in the CCU have been provided with education on how to recognise an extravasation in all stages (see Figure 3) and about the risks of vasopressors administered peripherally.
What was the impact on the patient?
The patient did not lose function of the left hand and arm, recovering well from the extravasation. The skin grafting was successful. However, she had to remain in hospital for an additional 5 days and has been left with permanent scarring from the extravasation and skin grafting, both of which have caused emotional distress.
What was the estimated economic cost?
- HRG minor skin procedure tariff, plus 5-day post-op trim point, totalling £620
- Consultant plastic surgeon outpatient clinics x3 (£163 for a 30min), totalling £489
- Approximate additional cost of £1109, as the patient required additional procedures.
ivWatch monitoring versus no monitoring
This article has illustrated the cost of infiltration and extravasation to the NHS using different clinical scenarios, either through showing additional treatment costs, drug waste or additional bed days, outpatient appointments and litigation. The highest cost remains to the patient through physical and psychological harm.
It is difficult to quantify the degree of emotional and psychological harm that an extravasation injury can incur not only for the patient, but also for the nurses and doctors involved. If the patient requires future IV therapy, they may experience additional stress, as they will always be concerned that an extravasation might occur once again.
In the first article in this series on infiltration and extravasation the ivWatch clinical trial data were detailed. One aspect that all case studies have in common is that had ivWatch been used to monitor the infusion site, the extravasation injuries would not have occurred to the degree that they did, based on the finding reported in the first article.
The estimated financial savings from the case studies alone would easily justify the investment in ivWatch to prevent infiltration and extravasation from occurring: ivWatch technology helps both the patient, giving them confidence that an extravasation injury was not likely to occur during IV therapy administration, and clinical staff, who can rely on the technology to monitor patients and identify potential problems.
Added to the savings outlined in this article are the positive effects of early identification and risk mitigation that the ivWatch technology makes possible. These include decreased lengths of stays, reduced number of procedures, elimination of delays in care, reduction of drug dosing errors, decreased risk of hospitalacquired infections, reduced pressure on beds, minimal medical supply usage, less wastage, and lessening of the burdens on clinical resources. Of additional importance is reducing the revolving door of hospital care with patients returning to have the injuries incurred through extravasation subsequently managed and treated.
It is also evident from the case studies and data presented in the previous article that adopting this technology brings great benefits to both the organisation and the patient. It is worth the financial investment to the organisation, because it not only improves patient outcomes and wellbeing, but also improves its safety profile, and minimises litigation related to infiltration and extravasation injuries. Above all, however, the use of ivWatch results in a continued perception by the patient that they are being cared for by a healthcare organisation that places great emphasis on safety and prioritises protecting them from avoidable infiltration and extravasation injuries.
KEY POINTS
- ivWatch technology can reduce the number of injuries associated with intravenous infiltrations and extravasations
- The emotional and psychological toll associated to extravasation injuries for the patient and the nurse or doctor involved should be considered, and support should be provided to all those affected
- The use of calcium chloride 10% can be switched to calcium gluconate 10%. Care must be taken to give the correct dose, but the additional time and effort can make a huge difference to the outcome of an extravasation injury
- This article has limitations, due to the lack of published information to support quantification of the full extent of an extravasation injury and the lack of education on how to correctly diagnose an extravasation injury
CPD reflective questions
- Consider how ivWatch technology can be utilised in your infusion practice to eradicate infiltration and extravasation injuries
- Do you know the signs and symptoms of infiltration and extravasation?
- Who is your hospital extravasation lead, and are you aware of your local guidelines for infiltration and extravasation?
- What would you do if you noticed an infiltration or extravasation?