
Monoclonal antibodies (MAbs) have been used in oncology treatment since the 1990s (Carter et al, 1992) and work by binding to antigens on the surface of cancer cells to mimic the body's own immune response (Bayer, 2019). Many MAbs can be administered via subcutaneous injection, reducing treatment time by up to 97% compared with intravenous infusion alternatives (DuMond et al, 2021).
Since 2018, increasing numbers of MAbs have been licensed and introduced in the Chemotherapy Day Unit at the author's Trust, as well as nationally, which has coincided with year-on-year increases in patient numbers (Cancer Research UK, 2024). The regimens for MAbs often require patients to attend multiple cycles of treatment over several months or years, putting further pressure on treatment capacity. The onset of the COVID-19 pandemic and its impact on patient care further compounded these pressures, and consequentially triggered a comprehensive pathway review.
Since the COVID-19 pandemic, treatment scheduling has been optimised and appointments have been staggered to enable optimal capacity use throughout the day. Capacity was further increased in the Chemotherapy Day Unit by extending opening times to include Saturdays and Bank Holidays. Initially, this was only possible for patients receiving regimens containing drugs with long expiry dates, as at that time all drugs were made up by the Aseptic Pharmacy during standard operating hours. The resulting increased treatment capacity in the Chemotherapy Day Unit was met with concerns from the Aseptic Pharmacy that they would be unable to manage the corresponding increase in activity. Due to Aseptic Pharmacy capacity limitations, more pressure was exerted on cancer services, resulting in delays, and an increasing patient backlog.
To address the competing challenges of patient numbers and Aseptic Pharmacy capacity, the possibility of preparing some MAbs in the clinical area was considered. To the author's knowledge, this was the first NHS trust in the country to implement nurse-led MAbs preparation using the ChemfortTM closed system transfer device (CSTD).
Although MAb preparation in the clinical area would allow staff to increase capacity, it was imperative that the safety of the nurses undertaking this new task was ensured and the risk of needlestick injuries and exposure to spillage, vapours and aerosols of systemic anti-cancer therapy (SACT) minimised. Another concern was around the potential variation between staff in their preparation technique, and the risk of contaminating the preparation.
Doxorubicin administration via bolus injection had previously been a concern for SACT exposure for staff, and CSTDs had been implemented to minimise this exposure (Marler-Hausen et al, 2020). Therefore, following the success of CSTD evaluation for doxorubicin administration, the same devices were considered for ward-based preparation of MAbs.
Methods
A risk assessment was developed considering the increased demand for MAbs, the complexity of the preparation (powder formulations, multiple dilutions, and so on), the potential toxicity of the drug and exposure risk for the staff. To mitigate the risks, patient pathways were reviewed, and a standard operating procedure (SOP) was developed, including:
- A procedure for the risk assessment of each drug, accounting for its individual toxicity risk and the complexity risk (for example, powder formulations, multiple dilutions)
- A procedure for safe handling of MAbs in the clinical area, including personal protective equipment (PPE), CSTD, appropriate preparation room, sterilisation of the equipment tray (Figure 1a), the volume of patients, and new roles for nurses
- A direct observational procedure assessment to standardise practice
- Education sessions for each individual drug, including its storage temperature, side effects, and the need for filters
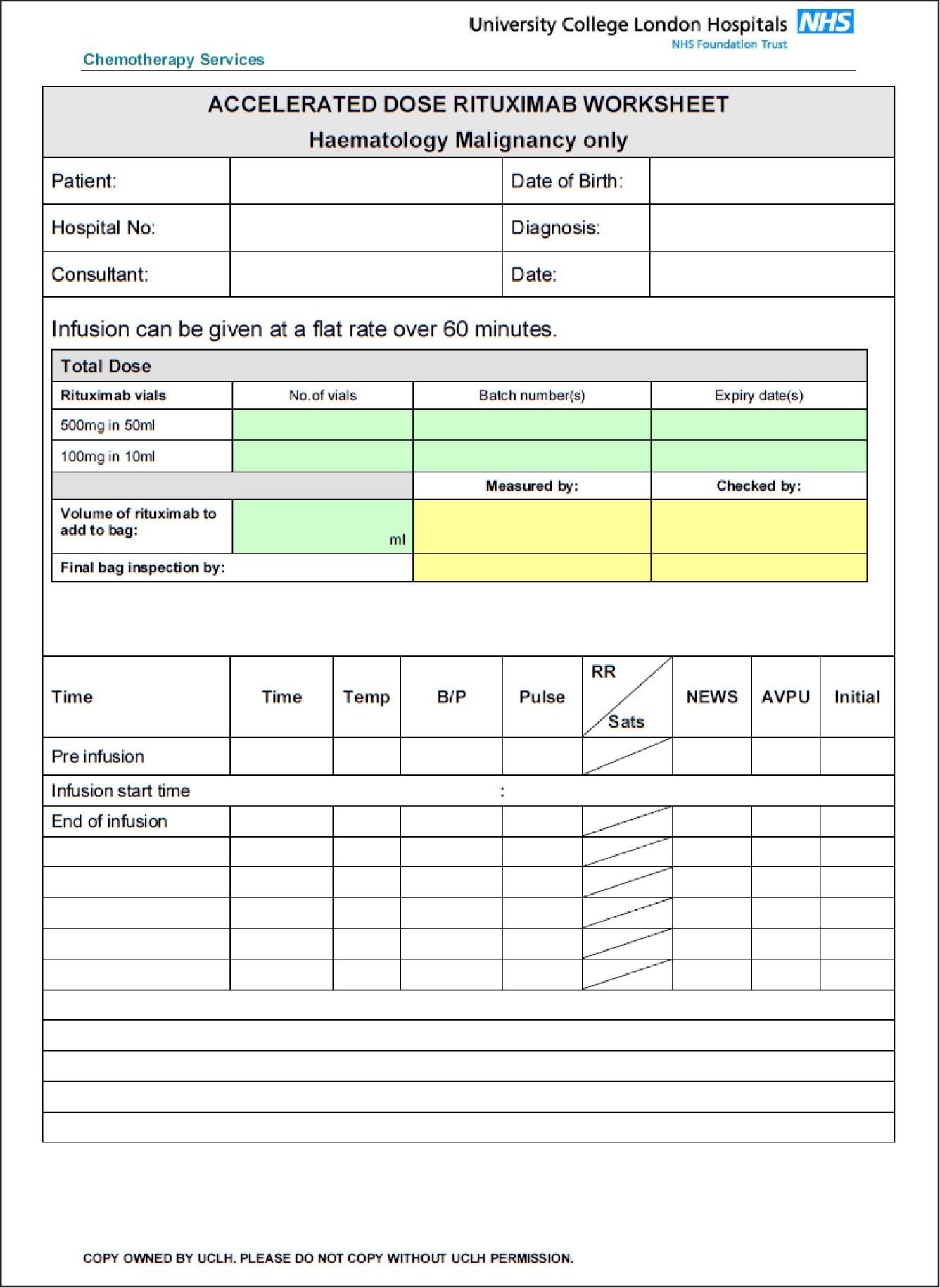
- A worksheet produced for each nurse-prepared MAb (Figure 2), including drug and diluent volumes required.

Once the new SOP was in place and nurses had familiarised themselves with the MAbs preparation process, staff were sent an anonymous survey asking for their feedback on their experience of the new process.
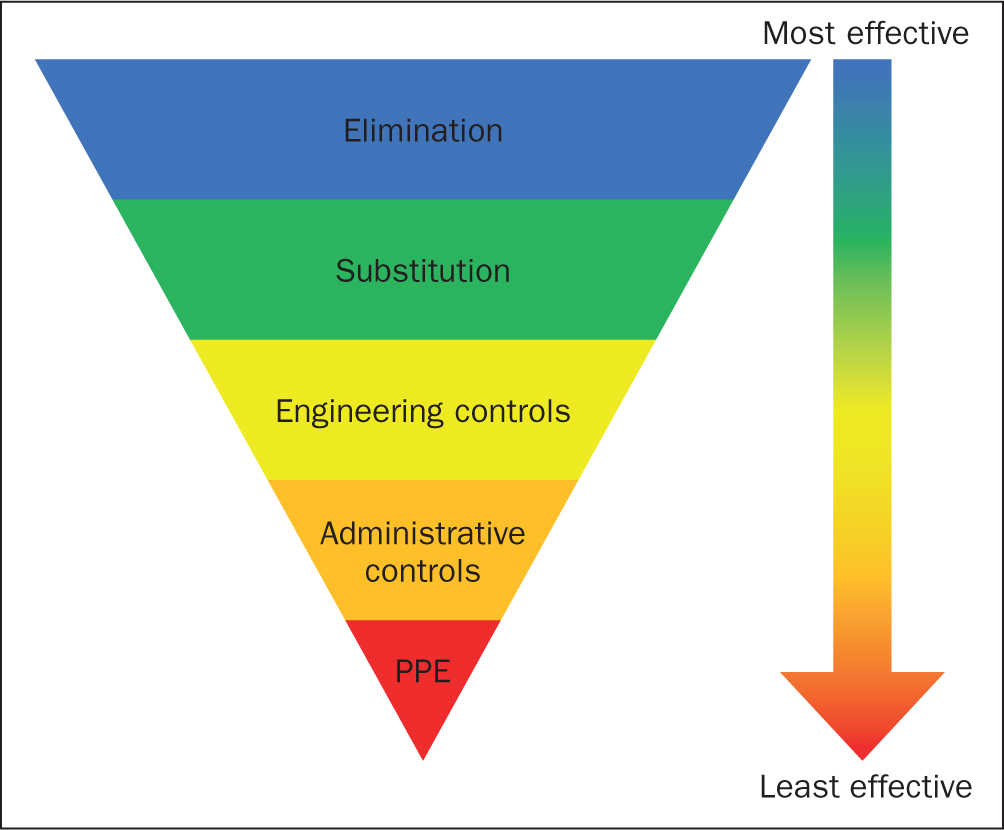
Based on the hierarchy of control (Health and Safety Executive, 2022; Figure 3), CSTDs, a form of engineering control, were implemented to minimise the risk of staff exposure.
An evaluation of CSTD for MAb intravenous (IV) bags and subcutaneous MAb preparation and administration was performed from containment performance, usability, and a cost point of view. Bolus administration of doxorubicin was additionally carried out using the CSTD. From the available CSTDs, the chosen option was the Chemfort CSTD (distributed by B. Braun Medical UK) (Figure 1b, 1c, 1d).
A pilot on the effectiveness of the Chemfort was also performed, looking into the length of time it took a nurse to make up the drugs in the clinical area compared with the waiting time for MAbs to be manufactured by the Aseptic Pharmacy.
Results
By adopting this approach, it was possible to safely move from Aseptic Pharmacy-led to nurse-led preparation of IV MAbs in clinical areas. The drugs prepared were rituximab, nivolumab, pembrolizumab, bevacizumab, daratumumab, alemtuzumab, and subcutaneous PHESGO (trastuzumab and pertuzumab), trastuzumab, daratumumab.
Three nurses each prepared pembrolizumab (the MAb taking the shortest time to prepare) and isatuximab (the longest time to prepare) under timed observation. A mean time for each MAb was calculated (Table 1). These results showed that the total time to prepare MAbs, including preparation of the work area, is between 15 minutes 23 seconds and 25 minutes 5 seconds, representing a 72-83% reduction in the patient waiting time for MAbs to be ready to administer.
Table 1. Timings for the preparation of two monoclonal antibodies, pembrolizumab and isatuximab)
| Step | Timing test 1: Pembrolizumab | Timing test 2: Isatuximab |
|---|---|---|
| Washing hands and donning PPE* | 00:49 | 01:00 |
| Cleaning the tray and collecting all materials ready to begin preparation | 03:10 | 06:58 |
| Checking the drugs and patient's identity | 04:14 | 03:20 |
| Preparation time | 07:10 | 13:47 |
| Total time | 15:23 | 25:05 |
Eighteen nurses completed the anonymous survey, which asked staff to rate their experience of nurse-led MAb preparation compared with pharmacy-led preparation.
Nurses were asked the following questions (see Figure 4)
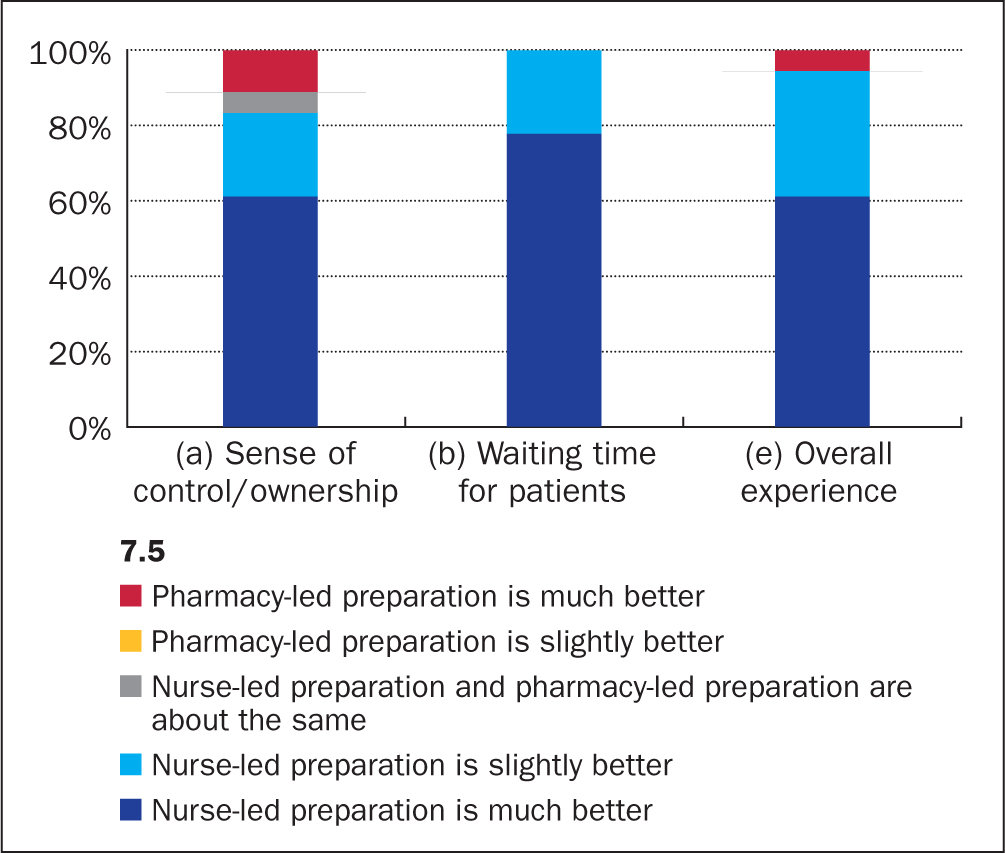
- How would you rate your sense of control/ownership over the MAb preparation process now compared with when Pharmacy used to prepare MAbs?
- How would you rate the waiting time for patients now compared with when Pharmacy used to prepare MAbs?
- How would you rate your overall experience of nurse-led MAb preparation compared with when Pharmacy used to prepare MAbs?
The majority responded that they had an improved sense of control or ownership and that they found preparing MAbs easy (both 83%); that they felt safe preparing MAbs and that their overall experience of nurse-led MAb preparation was better than pharmacy-led preparation (both 94%). All nurses agreed that the waiting time for patients was either slightly better (22%) or much better (78%) than pharmacy-led preparation (Figure 4).
Nurses also provided written feedback about their experiences:
‘It saves time as patients don't have to wait for MAbs to be made, which can cause a backlog. This is both better for patient experience and staff stress levels.’
Nurse 1
‘Advantages are it increases capacity in terms of appointment time and day cases can be treated, and we can treat more patients on nurse prepped drugs as we're not waiting for 1.5 hour [pharmacy] production time. Disadvantages are that space is needed to draw up drugs, and time is needed – it is quite quick but if we're very busy it can add to workload.
Nurse 2
‘It frees up space in production [pharmacy], reduces waiting time for patients, gives nurses control over when to administer, reduces wastage, and reduces time chasing if drugs are ready.’
Nurse 3
Since the new pathway was implemented, an average of 512 doses of MAbs have been prepared by nurses per month in the author's Trust. This equates to more than 6000 doses per year released from strained Aseptic Pharmacy capacity, and 7168 hours of waiting time eliminated for patients per year.
Discussion
The introduction of nurse-led MAb preparation was not without disadvantages, such as increased workload for nurses, the need to monitor each new drug being rolled out, and the need to review pharmacy technician roles to support nurses with their new responsibilities. With the introduction of each new drug, vial sizes must be checked to ensure compatibility with the CSTD, and storage space at the Chemotherapy Day Unit needs to be effectively used.
However, nurse-led preparation of IV and SC MAbs in clinical areas using Chemfort has had a net positive effect, as it has helped the team to accommodate increased demand for MAb treatments and improve the level of services alongside patient satisfaction. Without the nurse-led MAb preparation, this increased capacity demand could not have been met. Patients' treatments are available more quickly and are also made possible on Saturdays and Bank Holidays, increasing flexibility for patients, as the service is not restricted by pharmacy capacity or opening hours.
Staff experience is also improved by the elimination of production delays for the included MAbs, and they have increased ownership and sense of control of the patients' treatment journey. The anonymous survey sent to nurses revealed that all nurses recognised the improvements in waiting time for MAbs, and a large majority of nurses rated their overall experience of the new nurse-led pathway as better than the pharmacy-led pathway. Moreover, senior staff have a legal and moral duty of care to nurses to ensure their workplace safety, and nurse exposure to harmful spillages, vapours and aerosols of SACT drugs is minimised by the CSTD. CSTDs have also been found to substantially reduce environmental contamination of other drugs, such as doxorubicin; previous studies have shown that CSTDs are an effective method of preventing spills of the cytotoxic drug (Marler-Hausen et al, 2020).
Although the waiting time for MAbs to be made up by Aseptic Pharmacy was previously 90 minutes, when checking and transport is removed the actual production time is 30 minutes. This means that the 512 doses made up by nurses per month relieves 3072 hours of production capacity per year, which will increase as more MAbs are added to the nurse-led preparation pathway. Already, from June to December 2023, there has been a 29% increase in the number of MAb doses dispensed from pharmacy to be prepared by nurses, due mostly to the introduction of isatuximab to the nurse-led preparation pathway in October 2023. This released production capacity can be refocused on drugs that are income-generating for the Trust such as those for clinical trials. Additionally, capacity is now released for the production of drugs for compassionate use, which are drugs to be administered only to a named patient, where all previous lines of therapy have been exhausted (Medicines and Healthcare products Regulatory Agency (MHRA), 2023). These must be produced on the day of treatment to be administered to the specific named patient.
Conclusion
Nurse-led MAbs preparation on the wards has decreased the time patients wait for their drugs to be available, improving patient experience. The use of a CSTD has minimised the risk of nursing staff exposure to SACT, and enabled the successful roll-out of the nurse-led MAbs preparation pathway. Consequentially, increased Chemotherapy Day Unit capacity is no longer being met with a corresponding increased pressure on the Aseptic Pharmacy at the author's Trust. Due to the success of this project, isatuximab has been added to the list of MAbs to be prepared by nurses on the unit, with durvalumab and atezolizimab to follow. Senior nurses will continuously review other drugs to be added to this policy.
KEY POINTS
- Nurse-led preparation of monoclonal antibodies (MAbs) was found to be a solution to both increased oncology treatment demand and strained Aseptic Pharmacy production limitations
- To minimise the risk of nurse exposure to systemic anti-cancer therapy (SACT), a closed system transfer device was implemented as an engineering control against spillages and vapours
- This resulted in around 80 minutes' reduced waiting time per MAb dose, improving patient experience, increasing nurse ownership, and reducing demand on Aseptic Pharmacy
CPD reflective questions
- What is your current process for producing MAbs at your hospital?
- What operational changes could be made at your hospital to reduce demand on Aseptic Pharmacy production?
- What benefits could closed system transfer devices bring to your staff and services?