

Of the £8.3 billion the NHS spent on 3.8 million patients with a wound in 2020, £5.6 billion was spent on the 30% of wounds that can be classed as hard-to-heal (Guest et al, 2020), referring to those that have not closed in the expected timeframe (Atkin et al, 2019). With demographic forecasts predicting people to live longer (Office for National Statistics, 2022), the incidence of hard-to-heal wounds is likely to increase, and those patients will have increasingly complex needs. Dealing with this increasing burden of hard-to-heal wounds requires a growing understanding of how to manage the factors impacting on a wound's ability to heal.
Wound exudate
Understanding exudate
One of the main symptoms associated with hard-to-heal wounds is the production of excess exudate (Atkin et al, 2019). Exudate, often referred to as ‘wound fluid’ or ‘wound drainage’, can be defined as ‘material composed of serum, fibrin, and white blood cells that escapes into a superficial lesion or area of inflammation’ (World Union of Wound Healing Societies, 2019). This increase in exudate production may be due to a prolonged chronic inflammatory response stimulated by a physiological cause, such as in malignant fungating wounds and inflammatory ulcers e.g., rheumatoid ulcers and pyoderma gangrenosum (Bernardes et al, 2021). Excess fluid of any composition on the skin for any prolonged period, which can be as little as a few minutes, will impair the protective nature of the stratum corneum, the outer layer of the skin, increasing the risk of skin injury and infection, whatever the cause of the fluid accumulation (Collier et al, 2014).
The (non-excessive) presence of exudate creates a moist environment that is beneficial for the wound-healing process. A moist wound-healing environment has been shown to promote re-epithelialisation, modulate the inflammatory reaction and reduce scar formation (Junker et al, 2013). The main function of exudate is to facilitate the diffusion of vital healing factors (e.g., growth and immune factors) and the migration of cells across the wound bed during wound healing (Gushiken et al, 2021). Each main constituent of exudate has a different role (Table 1) (World Union of Wound Healing Societies, 2019). A moist wound environment promotes granulation tissue formation and epithelial migration (Liang et al, 2023), with benefits including improved healing rates, reduced pain and decreased risk of infection (Wounds UK, 2021). In superficial wounds, an optimal environment helps stimulate a regenerative process where dead cells are replaced by living cells. In deep wounds characterised by tissue loss, an optimal environment helps the multi-stage repair process involving synthesis of several tissue types (Collier, 2023).
| Constituent | Role |
|---|---|
| Water | Prevention of the wound from drying out |
| Nutrients | Promotion of cell health, such as glucose as a cellular energy source |
| White blood cells | Growth factor production, immune defence and reduction of bioburden within wound margins |
| Proteases | Degradation of proteins and assistance in autolysis and cellular migration |
| Protease inhibitors | Inhibition of proteases |
| Cytokines and growth factors | Stimulation of cellular growth |
Insufficient or excessive exudate
Insufficient exudate can cause excessively dry conditions that adversely affect healing (Box 1). It promotes the formation of dry, necrotic tissue (eschar) within the wound margins (Hurlow and Bowler, 2012). It also inhibits cellular activities, delaying autolytic debridement and healing (World Union of Wound Healing Societies, 2007; Sibbald et al, 2015). Moreover, it increases the risk of dressings adhering to the wound bed, damaging the wound bed and causing pain during dressing removal (Collier, 2023).
Potential consequences of insufficient exudate
On the other hand, uncontrolled excessive exudate has several negative consequences (Box 2) (Sibbald et al, 2015). It can damage the surrounding skin (maceration) with proteolytic proteases (enzymes that break down protein), as well as promote biofilm formation by acting as a potential nutrient source for bacteria (Hurlow and Bowler, 2012). Highly exuding wounds require more frequent dressing changes, which is inconvenient for patients and increases the cost of their care (Edwards, 2013; Wounds UK, 2013). Wounds with high levels of exudate can leak through dressings and clothing, which can lead to malodour and embarrassment, resulting in stress, loss of dignity and attempts to hide wounds with oversized clothes and footwear (Persoon et al, 2004; Beldon, 2016). This can restrict activities of daily living, such as work, socialising and domestic activities. Therefore, unmanaged excess exudate can have significant negative effects on a patient's psychological wellbeing and overall health-related quality of life (HRQoL). Excessive exudate may also indicate the presence of infection (Romanelli et al, 2010).
Potential consequences of excessive exudate
Assessment and management
Consequently, wound care should prioritise effectively managing excess exudate and maintaining an optimal wound-healing environment. This can improve clinical outcomes and patient HRQoL, as well as free up nursing time and healthcare resources. Exudate management should be part of a holistic and systematic model of wound care, such as TIMERS (Atkin et al, 2019). Exudate levels should be an essential part of all wound assessments, conducted and fully documented at baseline and each subsequent reassessment to track progress or deterioration (Flanagan, 2013). Only then can exudate and the wound environment be managed with interventions based on assessment results and an understanding of the principles of wound healing. The keystone of managing hard-to-heal wounds is evidence-based best practice of the underlying aetiology. This standard care can be supported with appropriate use of wound dressings, following the manufacturers' instructions. Selection of an appropriate dressing for controlling exudate will depend on the type, viscosity and amount of exudate (Vowden et al, 2015).
Superabsorbent wound dressings
Mode of action
Superabsorbents are a type of modern interactive wound dressing used to manage exudate and promote moist wound healing. Superabsorbents are designed to retain large volumes of liquid, which differentiates them from non-occlusive, permeable absorbent dressings that facilitate evaporation of absorbed moisture into the atmosphere (Folestad et al, 2008). Superabsorbents have a greater absorption capacity than traditional dressings, whose fluid-handling capacity can be suboptimal (Hughes and Jones, 2017), particularly under compression, allowing leakage of exudate and resulting in periwound maceration (Schulze et al, 2001). Consequently, superabsorbents play an important role in the management of moderately-to-highly exuding wounds (Jones and Hampton, 2021).
Superabsorbents are designed to absorb and lock away exudate, along with the bacteria and matrix metalloproteinases (MMPs) contained within it (Caley et al, 2015). Although MMPs help regulate the phases of normal wound healing, excess prolonged MMP expression can destroy growth factors and delay the wound's healing process, contributing to hard-to-heal status (Caley et al, 2015). Superabsorbents absorb and lock away fluid with a multi-layered structure, designed to work in sequence (Tickle and Fletcher, 2012):
Differences between superabsorbents
Although superabsorbents share the principles of this common structure (Gefen, 2021), different superabsorbents vary significantly in material selection, construction methods and manufacturing processes. For example, simpler superabsorbents have three-layer cores (SAP sheets), where the SAP grains are sandwiched between thin superior and inferior layers of paper (cheaper) or textile (better quality). Meanwhile, more advanced superabsorbents have three-dimensional cores (absorption pads), where the polyacrylate SAP grains are embedded within a structure of cellulose (cotton), fibres (cellulose fluff) and bonding fibres (Gefen, 2021).
These compositional variations often account for how separate superabsorbents perform differently in terms of clinical efficacy and cost-effectiveness (Gefen, 2020). For example, a study on the microbial and MMP sequestration of different superabsorbents found that, while all dressings could sequester bacteria, some dressings did so more effectively. There were considerable variations in bacterial viability in the dressings' core, as well as the extent and duration of bacterial retention (Singh et al, 2022).
Performance in the clinical setting does not always match laboratory results. For example, the results of absorbency tests depend on the chemical characteristics of a test fluid, and test fluids cannot always mimic clinical fluids. Standard laboratory absorbency scores for superabsorbents are highest with distilled water, noticeably lower with saline and still lower with fluids containing calcium or other ions, despite some superabsorbents actually needing calcium ions present to create cross-links and thus absorb into a gel (Browning et al, 2016). It should be noted that superabsorbent is a comparative not an absolute term (Wakefield, 2024).
C-Sorb superabsorbent dressing
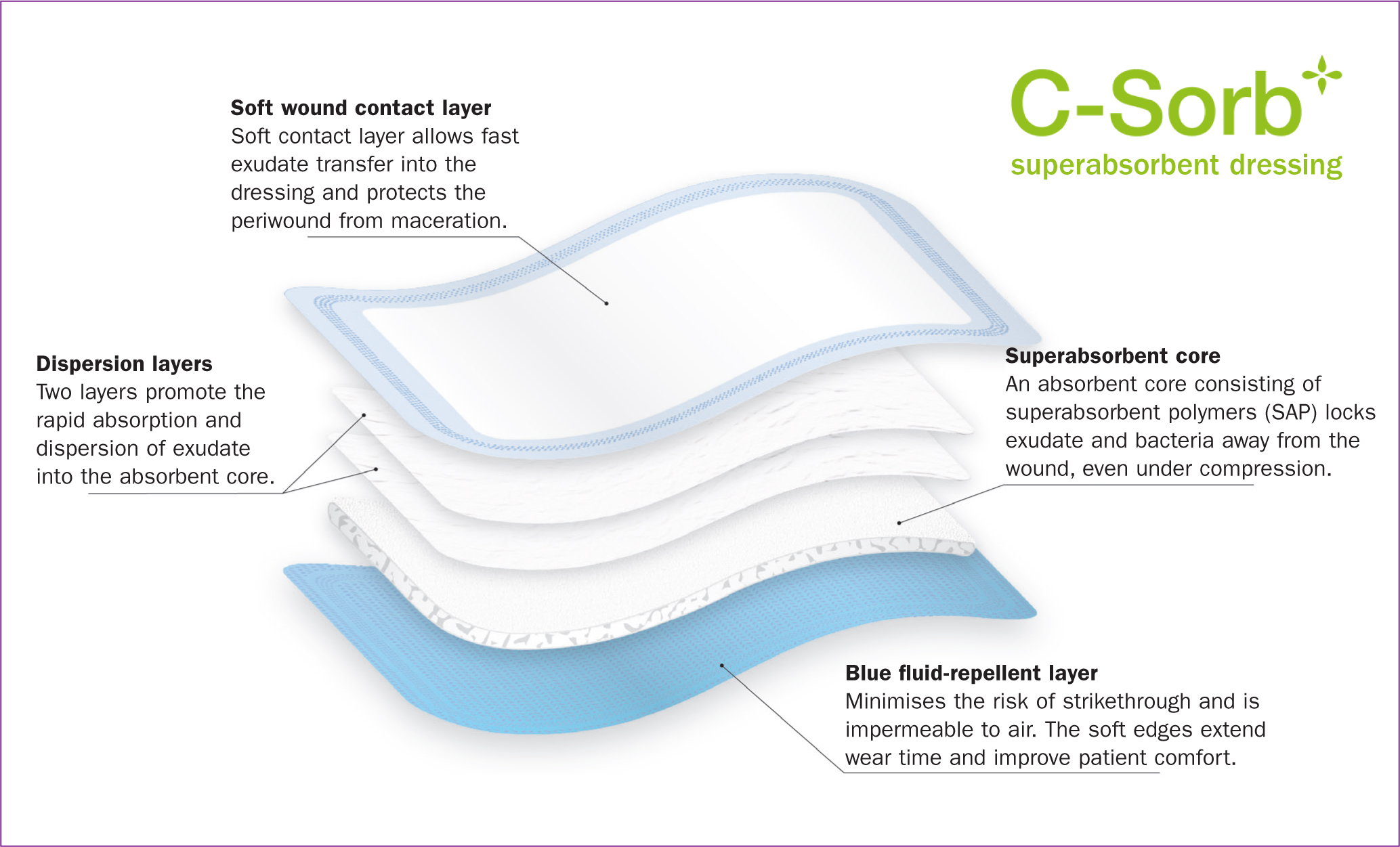
C-Sorb (Richardson Healthcare) is a superabsorbent designed to be a solution for managing moderate-to-high wound exudate levels and lymphorrhoea as a complication of lymphoedema (Box 3). Managing excess exudate should help minimise the incidence of maceration and reduce the number of dressing changes, thus achieving good patient outcomes at the same time as saving costs and nursing time. Their multi-layered design comprises a soft wound contact layer that allows free flow of fluids into the dressing; two fast-wicking dispersion layers that offer even absorption; an SAP core that locks away exudate, bacteria and MMPs; and a hydrophobic backing that prevents strikethrough for patient comfort (Figure 1). C-Sorb is generally used in conjunction with compression, and the fluid-repellent layer is designed to prevent the compression garments from becoming soiled by strikethrough.
Indications and contraindications for C-Sorb
Indications
C-Sorb is indicated for moderately-to-highly exuding superficial and partial-thickness acute and hard-to-heal wounds (including pressure ulcers, leg ulcers and foot ulcers and traumatic wounds). C-Sorb is suitable for use under compression.
Contraindications
C-Sorb should not be used on dry or heavily bleeding wounds. C-Sorb should not be used on infected wounds without professional advice.
Note
Before using a chosen wound-management product, health professionals should familiarise themselves with its properties and the manufacturer's instructions for use.
A study undertaken at the Surgical Materials Testing Laboratory, Bridgend in 2019 compared four superabsorbent dressings: C-Sorb (Richardson Healthcare), Eclypse (Advancis Medical), KerraMax care (Solventum) and Zetuvit Plus (Paul Hartmann). Compared with the other test dressings, C-Sorb had the highest absorbency (1.98 g/cm2), retention capacity (1.61 g/cm2) and absorbency under compression (1.15 g/cm2).
Patient and professional feedback on the experience of pain and malodour also led to the development of C-Sorb Silicone and C-Sorb Carbon. C-Sorb Silicone has a gentle silicone wound contact layer that allows for pain-free removal while maintaining stable fixation. C-Sorb Carbon has an integrated carbon layer designed to absorb and lock away malodorous molecules to minimise patient distress, embarrassment and social isolation (Caley et al, 2015). C-Sorb dressings and their packaging are designed to be low-cost and environmentally sustainable.
Case studies
Five patients with highly exuding, hard-to-heal wounds were trialled on C-Sorb for 3 weeks. All five patients reported improvements in their wounds over the 3-week period, and the treatment was found to be cost-effective.
Patient 1
Presentation and history
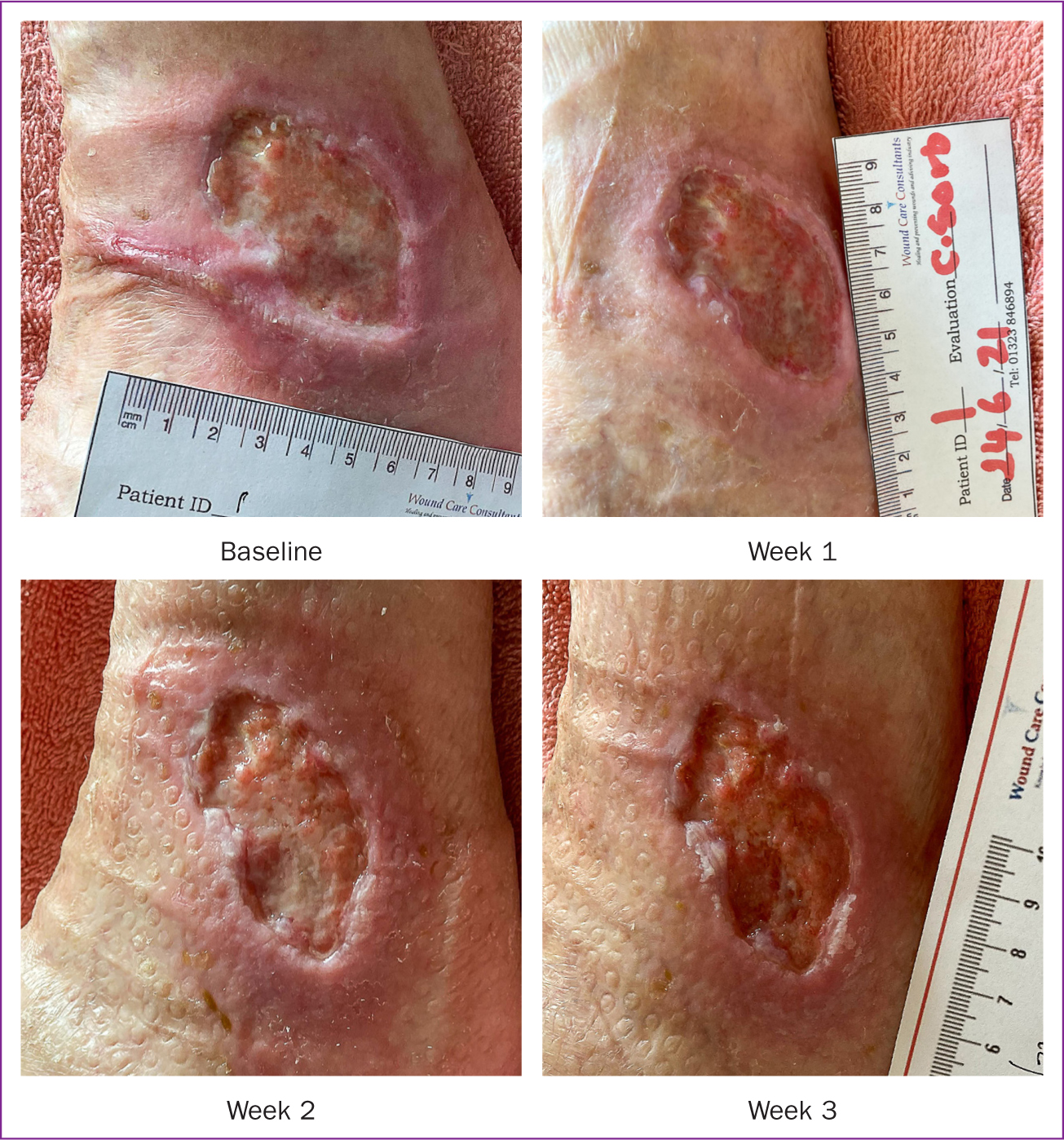
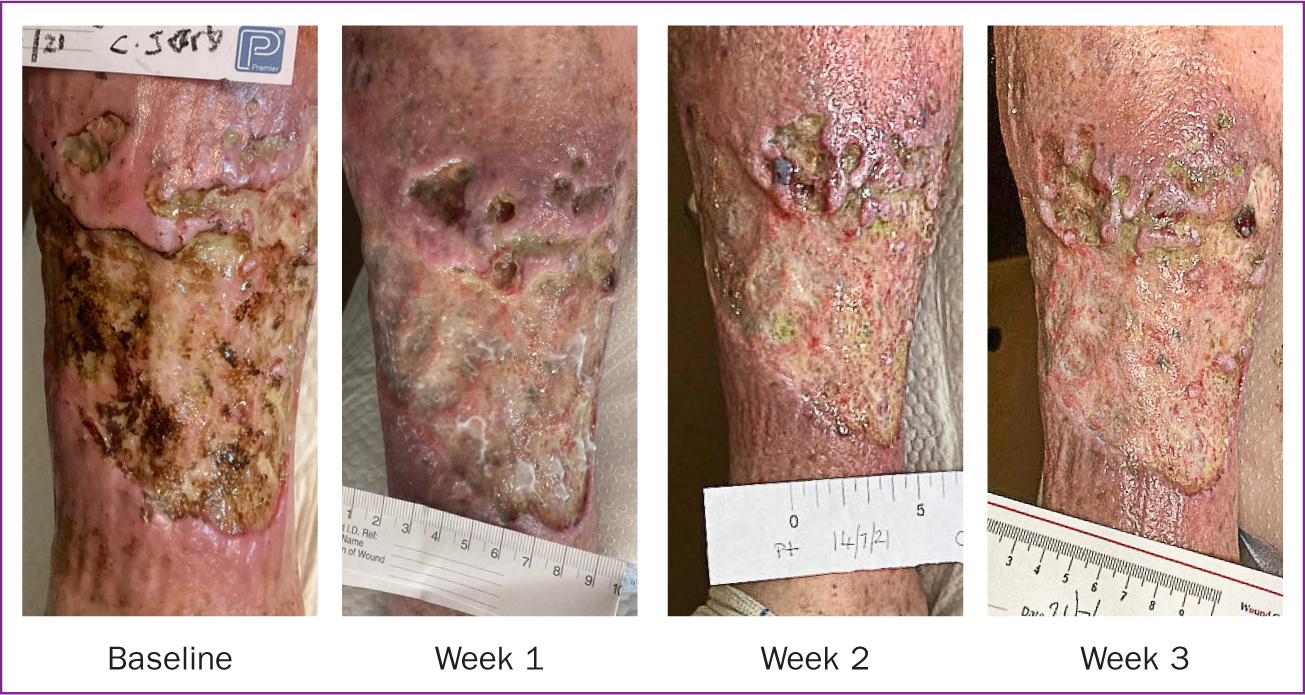
An 84-year-old female patient presented with a venous leg ulcer on the left lateral malleolus that had been present for 21 months (Figure 2). The patient had raised blood pressure, slight ankle fixation and osteoarthritis in the knees, which limited socialisation and may have contributed to the periwound erythema. The wound bed was covered in an even mixture of slough and granulation tissue. She was worried about the strong odour of her wound, and there were signs of increased bioburden. She was experiencing pain rated 4/10 (where 1 is no pain and 10 is the worst pain imaginable). The periwound skin was red, inflamed and in a poor condition.
The patient had twice-weekly visits from the practice nurse, who was a specialist in wound care running a dedicated clinic. The patient was undertaking ankle exercises, undergoing reduced compression therapy and taking amlodipine and paracetamol. Her wound had previously been treated with absorbent, foam and iodine dressings.
Intervention
The patient was trialled on C-Sorb to absorb exudate and reduce the risk of periwound soreness from proteolytic enzymes. The leg was soaked in water and had moisturiser applied, before the wound was dressed with C-Sorb and reduced compression therapy was applied. Compression was applied at reduced strength because the patient refused full strength, and healthcare staff felt any compression was better than none.
Outcomes
Overall, the signs of wound healing (including the wound bed, odour and periwound skin) improved at week 1, somewhat worsened at week 2 and improved again at week 3. However, pain reduced to just 1/10 from week 2. By the end of the trial, the wound bed showed considerably more granulation tissue than slough, and the surrounding skin showed considerably less erythema.
Discussion
The improvements seen are likely attributable to the combination of C-Sorb and compression therapy. The patient had an excellent overall view of the wound changes noted, especially because the reductions in pain, fluid loss and odour meant less embarrassment when visitors came. The treating nurse noted the reduction in odour and improvement in the patient's wellbeing.
Patient 2
Presentation and history
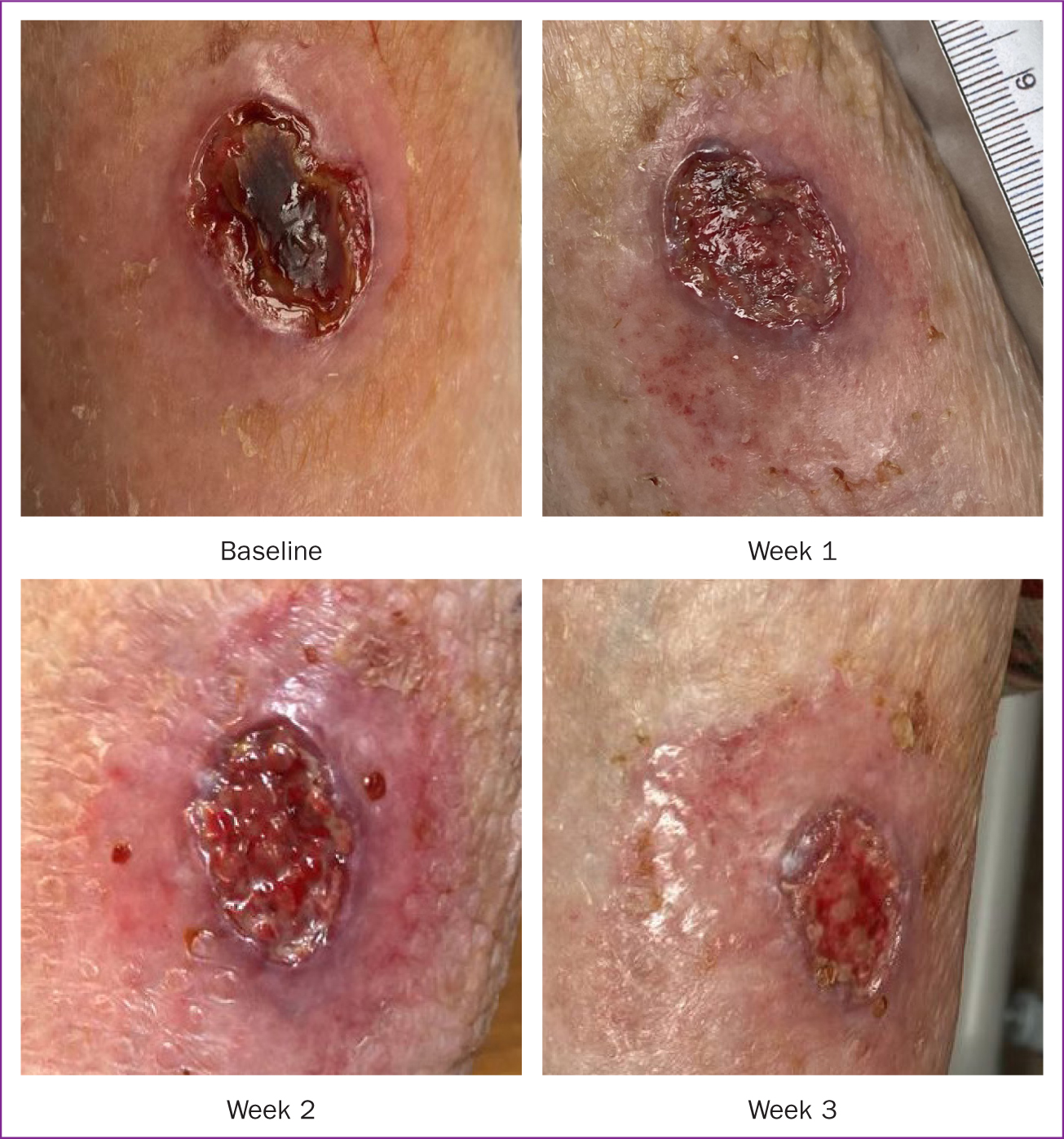
An 88-year-old female patient presented with a wound high on her right lateral calf, which had been present for 6 months (Figure 3). She had rheumatoid arthritis. The wound was entirely covered in necrotic tissue and surrounded by inflammation, suggesting high bioburden and possible pyoderma gangrenosum, despite little pain (2/10) or odour. The periwound skin was highly irritated, with minor erythema and swelling. The wound was being dressed with an adhesive foam, which was changed twice-weekly by the practice nurse.
Intervention
Activated carbon cloth was used for the first week to control bioburden. The inflamed periwound skin was treated with clobetasol propionate, and the wound was dressed with C-Sorb to absorb the increased exudate expected once the necrotic tissue lifted through autolytic debridement. The dressings were changed weekly.
Outcomes
The wound bed started off entirely covered in necrotic tissue, but by week 1 it was almost entirely slough and at week 2 it had fully granulated. The odour resolved by week 1, while periwound swelling, irritation and erythema fully resolved by week 2. Pain first increased to 4/10 at week 1 but then was completely gone from week 2.
Discussion
The wound bed had considerably improved by week 2, with no odour or pain and considerable improvement in the surrounding skin. In that time, the exudate had been effectively absorbed.
Patient 3
Presentation and history
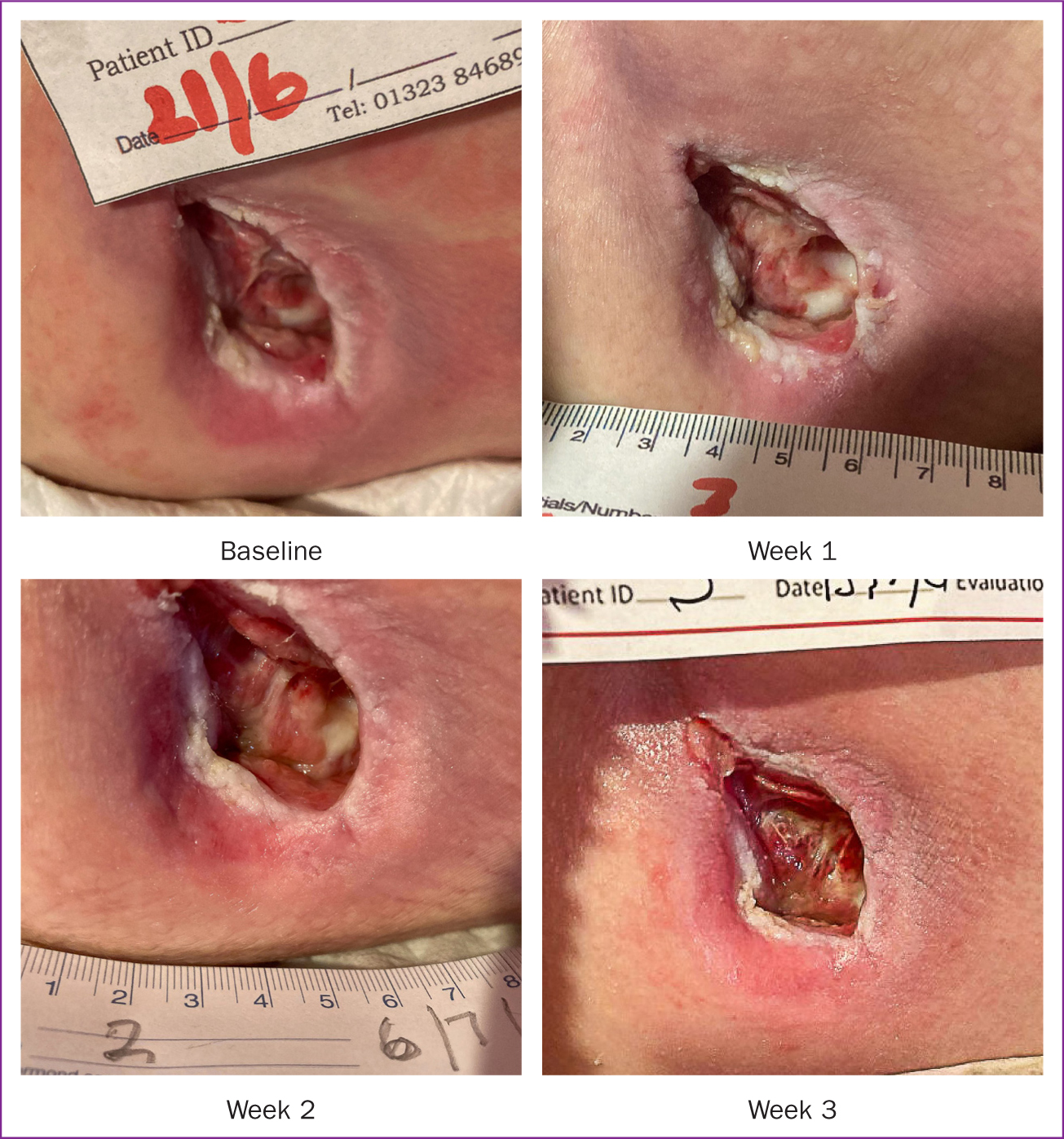
A 62-year-old male patient had had a pelvic wound on the left ischial tuberosity for an unknown duration (Figure 4). Pyoderma gangrenosum was suspected but not diagnosed. The wound showed 10% necrotic tissue, 65% slough and 25% granulation tissue. The patient was experiencing moderate odour, minor pain (2/10) and some periwound erythema.
Intervention
The wound was cleansed with a wound irrigation solution over gauze for 10 minutes, and then was dressed with C-Sorb.
Outcomes
The following 3 weeks saw a gradual decrease in devitalised tissue on the wound bed and a steady improvement in the condition of the periwound skin. By the end of the 3-week trial, the wound was smaller, with only minor odour and minimal pain (1/10).
Discussion
The wound showed positive progress over 3 weeks, with improvements in tissue types, skin condition, malodour and pain.
Patient 4
Presentation and history
An 87-year-old male patient presented with broken skin and a large haematoma on the upper calf due to a traumatic wound from a fall 6 months previously (Figure 5). The surrounding tissue was red and inflamed, and the patient was experiencing severe odour and very high pain (9/10).
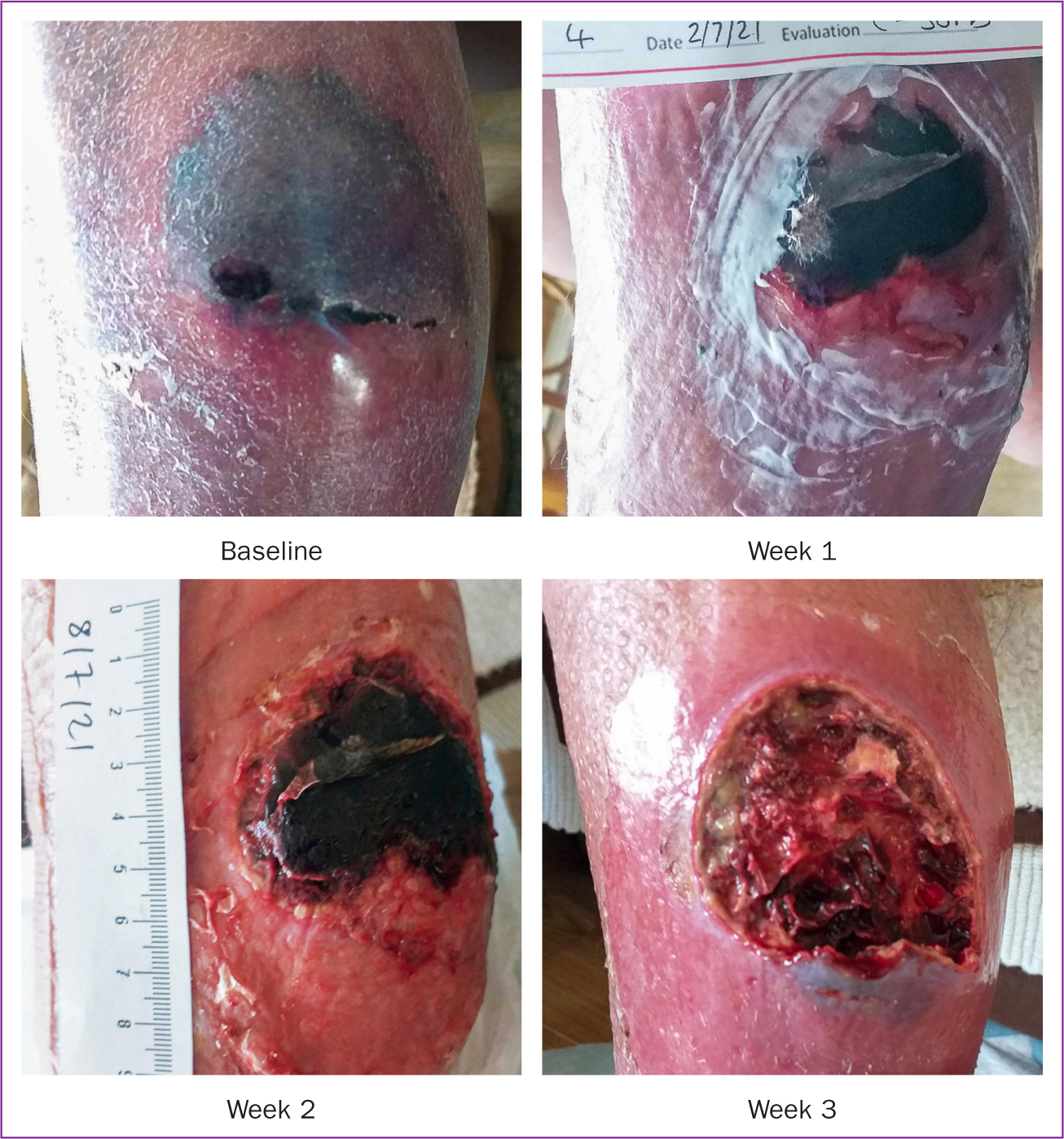
Cellulitis was suspected but then ruled out by two tissue viability nurse consultants. The wound was first treated with a pressure pack, ice and arnica. Adjuvant treatments were attempted but discontinued, including systemic antibiotics and compression bandages.
Intervention
The haematoma was sharp debrided with a curette over the following weeks. This was done gently and in stages to minimise pain. After debridement, the wound was dressed with a hydro-responsive dressing and C-Sorb, which was applied to control the expected increase in exudate once the haematoma and devitalised tissue came away. A compression bandage was also applied with the patient's agreement. The dressings and bandages were changed weekly by a tissue viability nurse (TVN). At week 2, the hydro-responsive dressing was stopped.
Outcomes
By week 1, the haematoma had been mostly debrided, and the wound was beginning to heal. By week 2, the haematoma had been fully removed, and the wound bed was consequently covered in a hard necrotic tissue (eschar) formed from dried blood. The eschar also underwent sharp debridement, and it was mostly cleared by week 3, allowing the wound bed to begin to granulate. The odour significantly reduced from week 1 onwards and was mild by the end of the trial. Pain also dramatically declined to 5/10 at week and 3/10 at week 3. The condition of the periwound skin gradually improved along with that of the wound.
Discussion
By the end of the trial, the haematoma and eschar had been debrided, and the wound was beginning to progress towards healing.
Patient 5
Presentation and history
A 78-year-old female patient presented with a venous ulcer on the right calf, present for many years (Figure 6). The patient used intravenous recreational drugs and would inject into or around the wound at least daily, which was the likely cause of the wound's chronicity. The wound bed was entirely devitalised, covered in half necrotic tissue and half slough. The periwound skin condition was also very poor due to injection of drugs into the tissue. The wound was very painful (9/10) and produced a severe odour. The wound was evidently deteriorating.
Intervention
The wound was dressed with a hydro-responsive dressing and C-Sorb, and a compression bandage was applied. The patient chose to change her own dressings daily, and she was reviewed weekly by the TVN. The hydro-responsive dressing was discontinued at week 2, but otherwise the treatment remained the same throughout. The patient was fully self-caring, having been taught how to change her own compression bandages and proving very good at doing so.
Outcomes
Over the first 2 weeks, the dark necrotic tissue cleared up to be replaced by slough, and in weeks 2 and 3 this slough began to thin, with some minor granulation. By week 3, pain had reduced to 3/10, and there was only minor odour. The periwound skin had slightly improved.
Discussion
The compression bandage and dressing were having an additional positive effect by stopping the patient from injecting into the wound. The patient reported an improvement in her quality of life due to a reduction in wound malodour. This may have been facilitated by C-Sorb's high absorbency and the containment of bacteria within the dressing. The patient remained on C-Sorb and compression. However, the wound and periwound remained unlikely to fully heal while the patient continued to inject drugs into the area.
Conclusion
Excess exudate remains one of the major challenges in wound care, often leaving patients with a hard-to-heal wound that is wet, malodorous and painful, adversely affecting their quality of life. Together with appropriate management of the aetiology, wound dressings remain the mainstay of exudate management, and so healthcare professionals and patients need to have confidence in the capability of the dressings selected. Superabsorbents are well-suited to absorbing and retaining exudate, and so they play an important role in the management of moderately-to-highly exuding wounds.
Further research would be valuable to demonstrate how superabsorbents have evolved, as well as identify their appropriate place in a wider clinical wound-management pathways. This could examine the key role of superabsorbents in preventing maceration. Ideally, further research would assess and compare all superabsorbents on the market across a wider variety of wound types. Future studies should consider extending the evaluation period up to when a healing response may be identified (6–12 weeks). Also, if the chosen materials allowed, the study superabsorbents could be left in place for extended periods of time (as clinically dictated). This might help assess if savings in staff and resource costs could be achieved without detriment to the patient.
The cases above demonstrate the impact of the superabsorbent C-Sorb in hard-to-heal wounds characterised by excessive exudate, as well as symptoms such as devitalised tissue (slough or necrotic tissue) on the wound bed, maceration of the periwound skin and presence of pain and malodour. The patients reported reductions in pain and malodour, and there were evident improvements in the appearance of the wound bed and periwound skin. These results support published evidence on the absorptive and retaining capacity of superabsorbents in general and C-Sorb in particular, with resulting clinical and economic benefits.