

Ahard-to-heal wound has been defined as one that fails to heal in an orderly and timely manner with standard therapy, due to a disruption in the body's natural healing process (Troxler et al, 2006; Fletcher et al, 2022), caused by intrinsic and/or extrinsic factors (Werdin et al, 2009). Hard-to-heal wounds represent a significant clinical problem and a financial burden to healthcare systems (Guest et al, 2020), as well as significantly impacting patient quality of life (Arshad et al, 2020). Hard-to-heal wounds are often stuck in a chronic inflammatory state, which prevents healing (Fletcher et al, 2017). A major feature of chronic inflammation is the overproduction of matrix metalloproteinases (MMPs) (Atkin et al, 2019), which may present clinically as increased exudate. This exudate can be corrosive in nature, causing periwound maceration, wound expansion and an increased risk of infection (Bianchi et al, 2013; Harding et al, 2019).
Early assessment and identification of the barriers to healing can enable fast adoption of care interventions to prevent wounds from becoming hard to heal. This can be achieved with a framework tool such as the ‘Wound Balance’ concept (Garten et al, 2023).
This article discusses the use of Wound Balance and a superabsorbent dressing containing polyacrylate polymers (RespoSorb® Silicone Border, Hartmann) to lock away wound inhibitors, such as MMPs and microorganisms (Eming et al, 2008; Wiegand et al, 2013; Wiegand and Hipler, 2013), prevent tissue damage, reduce bioburden and move the wound into a healing trajectory. This is illustrated in three case studies.
Hard-to-heal wounds
Hard-to-heal wounds continue to pose challenges for patients, healthcare professionals and healthcare systems, with the prevalence of wounds increasing, causing a significant financial burden (Atkin et al, 2019; Guest et al, 2020). Negative effects on quality of life have been widely reported (González-Consuegra and Verdú, 2011; Upton et al, 2012), with patients and their families often describing a loss of hope of the wounds ever improving. Patients with hard-to-heal wounds are at increased risk of morbidity, including infection, sepsis and limb amputation, as well as mortality (International Wound Infection Institute (IWII), 2022). Thus, ensuring optimum assessment and management to prevent deterioration are key to preventing these adverse outcomes.
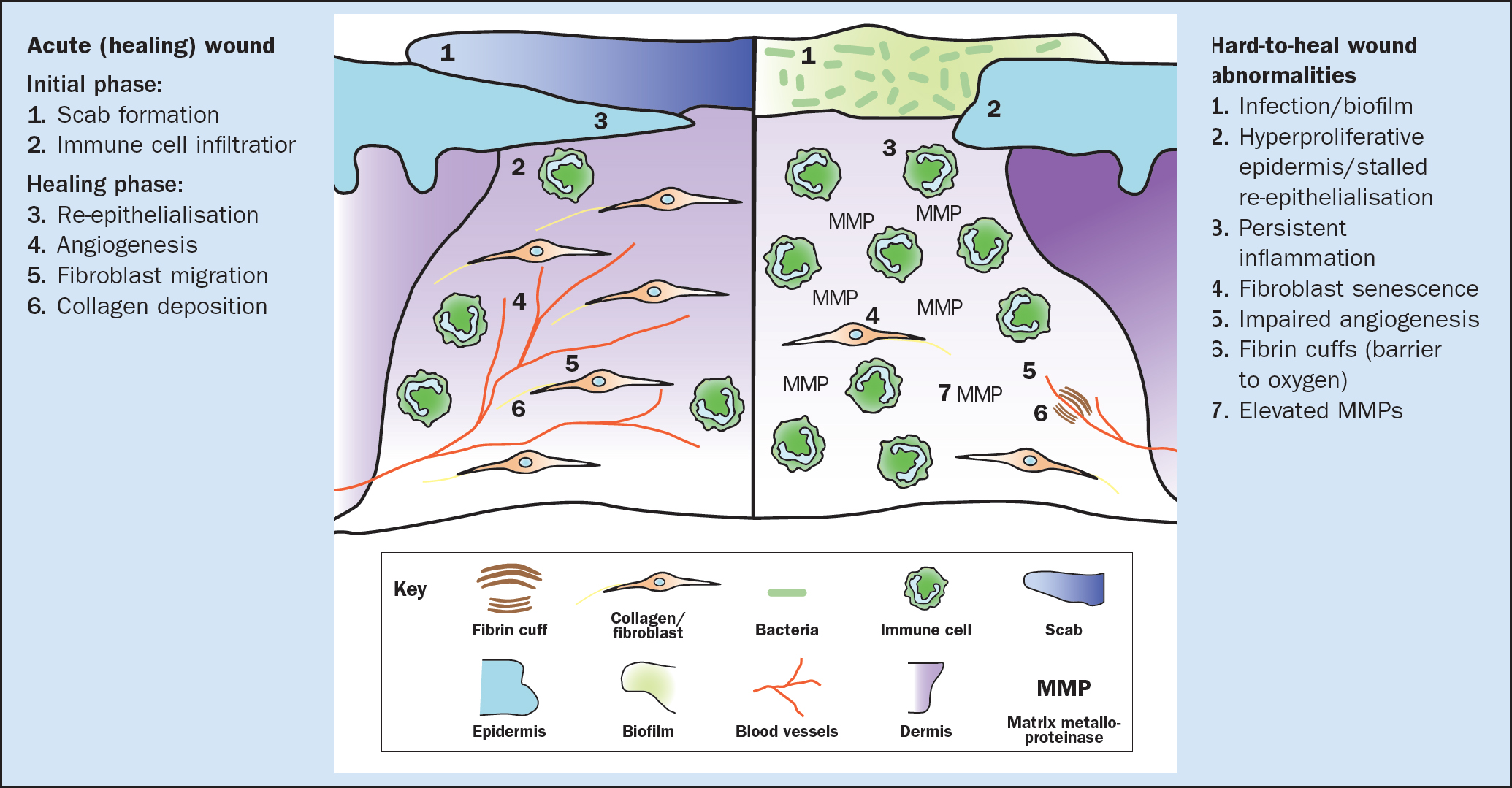
Evidence suggests that hard-to-heal wounds become stuck in a chronic inflammatory state (Figure 1), preventing the deposition of granulation and epithelial tissue (Nunan et al, 2014). There are often abnormally high exudate levels, which contribute to delayed healing (Atkin et al, 2019) and can result in quality-of-life issues for the patient, including malodour, wet dressings/bandages, embarrassment, social isolation and depression (Harding et al, 2019; Wounds UK, 2021).
Hard-to-heal wounds have three main components: the presence of tissue-destructive enzymes, predominantly MMPs; an oxidative environment caused by reactive oxygen species (ROS); and impaired endogenous control mechanisms that regulate enzyme activities (Atkin et al, 2019). MMPs are a vital part of the normal wound healing process (Figure 1); however, an increase in the MMPs and downregulation of the tissue inhibitor of metalloproteinases (TIMPs) in the hard-to-heal wound environment are part of the pathophysiology of the stalled wound (Atkin et al, 2019). Diminished growth factor activity, fibroblast/cell senescence and impaired proliferation are also key features (Garten et al, 2023). This can lead to the following clinical presentations:
- Increased bioburden, including biofilm formation and reformation, likely to present with increased, often corrosive, exudate, malodour and pain, increasing the risk of wound infection (IWII, 2022) and wound deterioration
- Increased exudate, which causes periwound maceration, wound expansion and strikethrough to dressings, further increasing the risk of wound infection (Harding et al, 2019)
- Egress of malodour, facilitated by strikethrough of exudate and soiling, is particularly distressing for patients, often causing social isolation and reducing quality of life (Harding et al, 2019)
- Presence of devitalised tissue, including slough and necrotic tissue (Percival and Suleman, 2015), provides an area of attachment for additional biofilm formation, encouraging the biofilm cycle further (Metcalf and Bowler, 2013; IWII, 2022)
- The wound fails to advance towards healing (Atkin et al, 2019)
- Wound pain is a common feature of hard-to-heal wounds (Newbern, 2018), and it is often cited as being the worst symptom of living with a leg ulcer (Leren et al, 2020). Together with underlying pathophysiological factors, the chronic inflammatory state of hard-to-heal wounds is likely to be the trigger to various types of wound pain (Holloway et al, 2024). Pain affects health-related quality of life, including sleep, mental health, social interaction and activities of daily living (Holloway et al, 2024).
Assessment of hard-to-heal wounds
The first step in managing hard-to-heal wounds is to undertake a full holistic assessment of the patient and wound. This incorporates identification of the physical, psychological and social issues to determine the underlying pathophysiology and determine any significant barriers to healing (Fletcher et al 2018a; 2018b; 2022) (Box 1).
Box 1.
Holistic wound assessment factors
Wound factors
- Anatomical site
- Exudate level
- Exudate type
- Wound-bed composition
- Wound dimensions
- Wound edges
- Periwound skin
Patient factors
- Age
- Co-morbidities
- Lifestyle and behaviour
- Medication
- Mental health and psychological wellbeing
- Mobility
- Nutrition
- Overall physical health
- Pain
- Sleeping pattern
Social factors
- Demographics
- Economic status
- Environment
- Social support
- Religious and cultural beliefs
Source: Fletcher et al 2018a; 2018b; 2022; Atkin et al, 2019
The initial management of hard-to-heal wounds is to undertake a full holistic assessment of the patient and wound, to determine the following (Fletcher et al, 2016; 2018; 2022):
- The underlying wound aetiology
- Patient co-morbidities
- Risk factors which may impede healing/cause further wound development (such as medication, lifestyle factors, wound aetiology)
- Patient symptoms (such as pain, sleeplessness and psychological issues) and factors affecting quality of life
- Social issues and environment; wound and periwound assessment including anatomical site, descriptions and measurements.
Early assessment, identification and management of the barriers to healing can improve the patient's healing potential and reduce the risks of the wound failing to progress (Garten et al, 2023). Identification of factors that may prevent a wound from progressing, including systemic inhibitors (Table 1) and local inhibitors of healing, such as elevated MMPs and inactivated growth factors (Figure 1). Treatment decisions and care planning should be implemented as early as possible to facilitate the normal phases of wound healing, such as angiogenesis and epithelial migration (Garten et al, 2023).
| Wound aetiology | Intervention strategy |
|---|---|
| Venous leg ulcer |
|
| Lympho-venous ulcer |
|
| Mixed aetiology leg ulcer |
|
| Arterial leg ulcer |
|
| Diabetic foot ulcer |
|
| Pressure ulcer |
|
| Surgical site wound |
|
| Malignant wound |
|
ABPI=ankle brachial pressure index; aSSKINg=Assess risk, Skin assessment and skin care, Surface, Keep moving, Incontinence or increased moisture, Nutrition, Give information; NICE=National Institute for Health and Care Excellence; NWCSP=National Wound Care Strategy Programme
Following an assessment, intervention strategies should be discussed with the patient, providing them with comprehensive information and education regarding their condition and to ensure that treatment is tailored to each individual (Garten et al, 2023). Aims and objectives can be agreed, as part of developing a clear care plan and to ensure delivery of evidence-based care (Fletcher et al, 2018a; 2022), with a focus on healing their wound, rather than just managing it (Table 1 and Box 2) (Trouth, 2023). However, it is important to set realistic goals with the patient, based on their needs; this is because symptom management may be more important to them than healing in the short-term. Assessment should be holistic and ongoing, following the care plan and adapted to the treatment (National Wound Care Strategy Programme (NWCSP), 2023a; 2023b).
Box 2.
Wound Balance concept
Clinical practice balance
- Addressing of all challenges (eg access to resources)
- Continuity of care in clinical decisions and practice
- Realistic time balance in daily practice
Patient care balance
- Patient-centred assessment and diagnosis
- Patient concordance
- Balance of a patient's quality of life (QoL)
- Outcome measurement (Wound-QoL)
Wound Balance
- Biomarker shift
- Normalisation and maintenance of healing trajectory
- Exudate management
- Early identification and intervention
Source: Garten et al, 2023
There are several widely adopted established wound assessment and management framework/tools available (Schultz et al, 2003; Dowsett et al, 2015; Atkin et al, 2019; Murphy et al, 2020).
Wound Balance
Wound Balance is a framework that takes a holistic approach rather than focusing simply on the wound itself concept (Garten et al, 2023). Wound Balance aims to integrate several critical parameters to enable continuity of care, individualise patient care and support clinical decision-making to shift the focus, where possible, from managing the wound to healing it as early as possible (Garten et al, 2023).
Wound Balance aims to help clinicians to (Garten et al, 2023) (Box 2):
- Understand the science of wound healing
- Understand the intrinsic and extrinsic factors preventing healing
- Recognise the risks factors that impede wound healing, to prevent chronicity
- Understand the importance of delivering a patient-centred approach to identify individual needs for assessment, diagnosis and treatment
- Consider and measure the impact on patients' quality of life and the impact of living with a wound
- Use and apply the increased knowledge to improve outcomes for patients.
Focusing on healing and improving the quality of life for patients should be embedded in everyday clinical practice. Optimising the wound healing potential for patients can be achieved with a proactive approach to incorporate wound bed preparation, exudate management, debridement and dressing selection (Garten et al, 2023).
Dressing selection and RespoSorb Silicone Border
Dressings should provide a safe, temporary physical protective barrier over a wound and encourage the optimum conditions for healing (Fletcher et al, 2023). Dressings can also help with other important aspect of wound care, such as managing increased MMPs.
Dressings containing superabsorbent polyacrylate polymers (SAPs) present a cost-effective and viable approach to MMP management (Velickovic et al, 2022). These dressings are not only able to absorb a high level of fluid (up to 100 times their own weight) (Garten et al, 2023), but they also have the ability to bind wound inhibitors, such as proteases and microorganisms (Eming et al, 2008; Wiegand et al, 2013; Wiegand and Hipler 2013). Locking wound inhibitors within the core of the dressing can prevent tissue damage and reduce bioburden, effectively impeding the factors associated with hard-to-heal wounds, to create a healing environment similar to that of an acute wound (Garten et al, 2023; Mikosinski et al, 2022).
The mechanism of action consists of four steps (World Union of Wound Healing Societies, 2020):
- Absorption of wound inhibitors and microorganisms
- Sequestration (locking away) of proteases and microorganisms
- Retention of proteases and micro-organisms
- Removal of wound inhibitors and microorganisms within the dressing.
RespoSorb Silicone Border is a sterile adhesive bordered SAP-containing dressing; it has silicone interface and is designed to remove excess MMPs from the wound to promote progression towards wound healing. It is available in a variety of sizes, including sacral, heel and oval shapes. It can be used as a primary or secondary dressing for acute and chronic exuding wounds in all phases if healing (Probst, 2019). The dressing is composed of five layers:
- Green water-repellent and breathable backing for strikethrough protection
- Soft polymer core with SAP for fluid distribution and retention
- Hydrophilic layer for fast exudate transfer
- Atraumatic silicone wound contact layer
- Atraumatic silicone border.
After 24 hours of contact, RespoSorb Silicone Border can significantly reduce the amount of MMP-2 and MMP-9 that are present in excessive levels in hard-to-heal wounds (Davies et al, 2017). Excessive MMP levels result in degradation of growth factors and the extracellular matrix (ECM), halting or slowing the healing process (Caley et al, 2015; Harding et al, 2019). Elevated protease activity in a wound can result in a 90% chance that the wound will not heal (Moore and Strapp 2015). Therefore, inhibition of MMPs using SAP dressings can provide a conducive environment to promote tissue repair (Eming, 2008).
In clinical practice, RespoSorb Silicone Border has demonstrated the ability to manage wound exudate, improve the wound edge and periwound skin, and have a positive effect on wound-bed preparation, all of which improve healing and quality of life for patients (Barrett et al, 2020; Velickovic et al, 2020; 2023; Trouth, 2023).
RespoSorb Silicone Border is very easy to use, comfortable and maintains its fluid retention capacity under compression therapy (Harding et al, 2019; Barrett et al, 2020; Trouth 2023). The silicone wound contact layer enables atraumatic dressing changes, reducing associated pain, and leads to increased health benefits compared with the use of standard care (Barrett et al, 2020; Velickovic et al, 2020). The silicone adhesive of the dressings helps prevent medical adhesive-related injury (MARSI), which is key to preventing harm to patients during dressing changes (Wounds UK, 2023). The conformability, high absorbency and silicone adhesive of the dressing ensures that it remains in situ, resulting in longer wear time compared with some foam dressings (Barrett et al, 2020), and brings associated economic benefits (Velickovic et al, 2020; 2023).
A recent predictive early-stage analysis demonstrated that using RespoSorb Silicone Border, compared to various foam dressings, improved healing, quality of life and cost savings for patients with moderate-to-highly exuding leg ulcers using (Velickovic et al, 2023).
Case studies
A case series of three patients was undertaken to demonstrate the benefits of using RespoSorb Silicone Border to facilitate Wound Balance and promote wound healing. In each case study, the patient received early assessment and intervention.
Case study 1
A 34-year-old female patient presented with a surgical wound on the right mid back created by an open incision and drainage of an infected sebaceous cyst and had been present for 48 hours prior to the first visit (Figure 2). The patient also had hypertension, which can affect wound healing. The wound measured 3cm×1cm, and it was covered in 20% slough and 80% granulation tissue. There were no signs of infection, nor odour or pain, and the periwound skin was healthy and the exudate level low. The clinician completed a quality-of-life tool: Wound-QoL-14 (www.wound-qol.com), reporting that the patient noted a little unhappiness and burden of the wound. The wound was being dressed with a hydrofiber dressing and a foam silicone border, changed once or twice weekly.

The patient was commenced on RespoSorb Silicone Border as a primary dressing.
By day 7, the wound had improved greatly, it had reduced size (2 cm×0.5 cm), there was good granulation (100%) and no exudate. By day 21, the wound had fully healed and the patient reported no quality-of-life impact.
The clinician remarked on the speed with which the wound had healed and characterised the performance of the dressing as ‘excellent’ in all areas. All aspects of the Wound Balance concept were considered in the selection of a dressing. RespoSorb Silicone Border proved an appropriate holistic choice for a patient who was only able to come to clinic once a week due to work commitments. The absorbency of the dressing meant that it could manage any increase in exudate, although in this case the exudate level was mostly low. Likewise, the patient was able to shower without the dressing coming off.
Case study 2
A 68-year-old male patient, who has chronic heart disease, presented with a surgical wound on the lower left leg (Figure 3). The wound had been created following resection of a basal cell carcinoma (BCC) 24 days prior to presentation, and it had subsequently dehisced. The wound measured 3 cm×1 cm, and it was covered in 10% slough and 90% granulation tissue. There were no signs of infection, and no odour or pain at presentation (although a little pain was reported on a quality-of-life tool), but the periwound skin was dry and there was moderate exudate. According to the Wound-QoL-14 assessment tool, the wound was having a negative impact on most aspects of quality of life assessed. The wound was being dressed with a sterile adhesive dressing, changed once or twice weekly.

The patient was commenced on RespoSorb Silicone Border as a primary dressing. On day 5, there was a slight odour and slight pain (2/10), but there was less exudate, the wound had reduced in size (3 cm×0.8 cm) and more granulation tissue (99%) was present. By day 10, the pain and odour were gone, and the wound continued to shrink and had fully granulated. By day 24, the wound had fully healed, and the patient reported no quality-of-life impact.
The clinician characterised the performance of the dressing as ‘good’ in re-epithelialisation and odour reduction and ‘excellent’ in all other areas, singling out exudate reduction and size reduction for positive feedback.
The use of RespoSorb Silicone Border was guided by the holistic elements of the Wound Balance concept. The wound was the result of a BCC resection and, through the study period, the patient was still waiting for a histology report to confirm whether BCC was still present. This was important for the healing trajectory of the wound, as the patient may have required wider excision. It also made the wound unsuitable for compression, which is contraindicated in skin cancer according to the National Wound Care Strategy Programme (2024). No other interventions were needed or used. There had been a plan in place to carry out a Doppler ultrasound in anticipation of the need for vascular referral, but the wound healed effectively, negating the need for more complex diagnostics and treatment interventions.
Case study 3
An 82-year-old male patient presented with a pemphigoid wound on the front right lower leg (Figure 4). The patient had had reoccurring pemphigoid wounds for the past 11 months and had been receiving treatment for these for the past 6 months. All but this one remaining pemphigoid wound had healed.

The wound was diagnosed and treated as venous in aetiology. His medical history included anaemia, asthma, atrial fibrillation, lung metastases, chronic kidney failure, heart failure and rectal adenocarcinoma. The wound measured 1.5cm×1.0cm, and it was covered in 90% granulation tissue and 10% epithelial tissue. There were no signs of infection or pain, the periwound skin was healthy and the exudate level low. The wound was having a negative impact on most aspects of quality of life assessed. The wound was being dressed with a simple film dressing, changed once or twice weekly. The underlying venous aetiology was being treated with compression hosiery, following initial use of compression bandages.
The patient was commenced on RespoSorb Silicone Border as a primary dressing, alongside compression hosiery. No other dressings or topical treatments were used.
By day 7 the wound had fully healed. However, the patient remained a little worried and afraid of new wounds appearing.
The clinician characterised the performance of the dressing as ‘good’ in ease of removal and ability to stay in place and ‘excellent’ in all other areas, commenting on the patient having healed, with good skin integrity.
Conclusion
The burden of hard-to-heal wounds has been well documented over the past few years. Therefore, it is more important than ever to shift the focus from managing a wound to healing a wound to minimise the risk of hard-to-heal status, focusing on a holistic approach to achieve Wound Balance (Garten et al, 2023).
RespoSorb Silicone Border is an SAP dressing that can reduce the high abnormal levels of MMPs and bacteria that are often found in hard-to-heal wounds and that inhibit wound healing (Davies, 2017). RespoSorb Silicone Border is easy to use, conformable and comfortable for the patient, and it enables a non-traumatic dressing change and has a long wear time. The dressing provides a cost-effective (Velickovic et al, 2020; 2022) alternative to foam dressings for patients with exuding acute and hard-to-heal wounds.
The case studies demonstrate how early assessment of wound risk factors and early appropriate intervention can improve patient outcomes. Case studies play an important role in developing an evidence base, but further well-designed studies are required to expand on this.
KEY POINTS
- Early assessment and identification of the barriers to healing can enable fast adoption of care interventions to prevent wounds from becoming hard to heal
- ‘Wound Balance’ is a holistic approach to assessment and care planning that can be adopted to optimise the healing potential for patients
- Wound Balance is achieved by shifting/regulating biomarkers such as elevated matrix metalloproteinases (MMPs) and improving growth factor activity and angiogenesis
- Superabsorbent dressings containing polyacrylate polymers (SAPs), such as RespoSorb® Silicone Border, can facilitate Wound Balance, reversing the factors associated with hard-to-heal wounds to enable a healing environment similar to that of an acute wound
CPD reflective questions
- What are the advantages of early assessment and identification of the barriers to healing?
- What characterses ‘Wound Balance’ as an approach to assessment and care planning?
- In what circumstances might it be advantageous to use superabsorbent dressings containing polyacrylate polymers?