

Medical adhesive-related skin injury (MARSI) has been overlooked and underestimated for a considerable time (McNichol et al, 2013; McNichol and Bianchi, 2016; Ousey and Wasek, 2016). McNichol et al (2013) first described it in a guidance document developed by a consensus panel. They reported that, when the correct techniques for the application and removal of adhesive products were not used, tissue trauma could occur, impacting patients' safety and quality of life, and increasing healthcare costs. Their document includes consensus statements on the assessment, prevention and treatment of MARSI. Fumarola et al (2020), in the international consensus document Overlooked and underestimated: Medical Adhesive-related Skin Injuries, have extended this pivotal guidance, expanding on the work done nationally and internationally in this area, and adding to the evidence.
The effects of MARSI are broad; it is not a simple area of skin damage but has potential to be widespread, with loss of skin integrity. It may lead to soft tissue infection, a delay in wound healing and increased pain, negatively affecting a patient's quality of life (McNichol and Bianchi, 2016; Ousey and Wasek, 2016).
This article outlines and discusses how optimal skin integrity can be achieved, drawing on the recent consensus document (Fumarola et al, 2020). In particular, it looks at how certain products can assist in preventing MARSI as opposed to treating it after it occurs, as MARSI is considered preventable harm (McNichol and Bianchi, 2016; Hadfield et al, 2019).
The skin
The skin is the largest organ of the body and performs many critical functions. It is a physical barrier to microorganisms and irritants. The pH of the skin has an antimicrobial function, so assists in preventing infection. Excretion and absorption, which play a crucial role in thermoregulation, helps protect against impending injury (Thayer, 2012).
The skin has two main layers. The first, the epidermis, is a thin layer with thicker layers over areas of friction and pressure, such as the palms and plantar surfaces of the feet (Thayer, 2012). The second layer is the dermis, which provides skin structure and resilience through the proteins collagen and elastin. In the dermal layer, there are blood vessels, sweat glands, hair follicles and sebaceous glands. Beneath the dermis is the subcutaneous fat layer (Thayer, 2012).
MARSI
Fumarola et al (2020) defines MARSI as skin damage related to the use of medical adhesive products or devices such as tapes, wound dressings, stoma products, electrodes, medication patches and wound closure strips. This is a much simpler definition than that given by McNichol et al (2013), in that it does not specify the type of skin damage that has to occur for it to be defined as MARSI nor the time frame in which MARSI can occur. McNichol et al (2013) suggested that skin changes should persist for 30 minutes or more after removal of an adhesive product, and this 30 minutes time period has been removed from the later consensus document (Fumarola et al, 2020). This is important as damage to the epidermal layer can occur as soon as the dressing is removed; on removal of any medical adhesive it is not uncommon to see a small amount of redness that may spontaneously disappear. If a subsequent dressing is applied to the same area, there is potential for further skin damage and the health professional will be unable to see it if a non-transparent dressing is used to cover the wound.
According to Fumarola et al (2020): ‘MARSI occurs when the attachment between the skin and the medical adhesive is stronger than the individual cells, causing the epidermal layers to separate or the epidermis to detach from the dermis.’
MARSI can be categorised into three types: mechanical, dermatitis, and other (eg maceration)(Box 1). The mechanisms for these are all different and therefore the presentation of the skin damage is equally different; however, all skin damage requires treatment in the main.
Box 1.Types of medical adhesive-related injuriesMechanical
- Skin stripping
- Tension injury or blister
- Skin tear
Dermatitis
- Irritant contact dermatitis
Other
- Maceration
- Folliculitis
To prevent MARSI, one of the most import measures is a full assessment of the skin. Skin assessment should occur in a well-lit environment for accuracy (Thayer, 2012; McNichol et al, 2013). It is important that the health professional obtains a history of known or suspected allergies, (McNichol et al, 2013) as part of this process, including risk factors for acquiring a MARSI. A full assessment of the skin as suggested by Fumarola et al (2020) would include:
- Visual inspection, including local signs of irritation or damage
- Palpation
- Temperature
- Colour
- Moisture level
- Turgor
- Fragility
- Integrity.
Fumarola et al (2020) describe the risk factors for MARSI in the consensus document; these are classified broadly as two categories of intrinsic and extrinsic (Table 1). These risk factors are very similar to those described by McNichol et al (2013).
Table 1. Risk factors for medical adhesive-related injuries
| Intrinsic risk factors | Extrinsic risk factors |
|---|---|
| Extremes of age: neonates and elderly people are at high risk | Dry skin (can be caused by low humidity) and harsh (non pH balanced) cleansers |
| Dehydration | Prolonged exposure to moisture |
| Malnutrition | Long-term use of certain medications, such as corticosteroids, anti-inflammatory agents, chemotherapeutic agents and anticoagulants |
| Dermatological conditions | Radiation therapy |
Underlying medical conditions:
|
Photo damage or exposure to ultraviolet light |
| Oedema | Tape, device removal and repeated taping Itching |
Source: Fumarola et al, 2020
The notable exception is the removal of race and ethnicity. This was unexpected as, in the authors' experience, those with darker skin pigmentation have a higher incidence of MARSI, particularly those receiving chemotherapy.
The risk factors are multifactorial, with individual patients potentially having more than one risk factor. An example of this is an elderly patient with comorbidities that puts them at risk combined with being dehydrated and/or malnourished; in this case, extra care would be required when using a medical adhesive and depend on the full skin assessment.
Medical adhesive products come in a variety of forms. Some are obvious, such as adhesive dressings, but others, such as surgical drapes, are less so. Regardless, they all pose a risk to all patients in all care settings (McNichol et al, 2013). The common types of medical adhesives used in healthcare are broadly categorised by purpose, which includes adhesion and securement (Fumarola et al, 2020):
- General adhesion, such as for dressing wounds and secure non-critical tubing
- Flexible adhesion in situations where swelling or movement is anticipated
- Securement of critical medical devices such as central vascular access devices, nasogastric and percutaneous endoscopic gastrostomy (PEG) products and stoma pouches.
In critical medical devices, the need for high adhesion may supersede all other considerations (Barton, 2020; Fumarola et al, 2020) but MARSI prevention should always be an important consideration.
Examples of medical devices with adhesion are:
- Electrodes for electrocardiography
- Vascular access device securement dressings
- Wound closure strips
- Surgical/procedural drapes
- Adhesive stoma products
- Adhesive wound dressings, such as hydrocolloids, foams and film dressings
- Tapes such as silicone, zinc oxide and acrylate tapes
- Plasters and first aid dressings
- Urinary catheter and sheath securement devices.
Injury from any medical adhesive devices will require treatment. Superficial skin stripping or a skin tear, for example, can be treated in a clinical environment provided there are clear guideline and protocols in place. However, persistent irritant contact dermatitis (ICD) that is not improving in a patient with a critical medical device in situ which cannot be resited would need specialist input; typically by a tissue viability nurse specialist.
Hitchcock and Savine (2017) describe a collaborative approach to preventing MARSI including ICD in critical medical devices (namely peripherally inserted central catheters) and developing algorithms to support best practice.
MARSI can have a profound effect on patients. An injury can range from being uncomfortable (Hadfield et al, 2019) to causing significant pain and distress (Fumarola et al, 2020). Minimising pain should be at the forefront of health professionals' minds (Collier, 2019) and products used to prevent pain, such as silicone medical adhesive removers, should be considered as standard (Collier, 2019; Barton, 2020).
A MARSI resulting from any medical adhesive can delay wound healing, cause scarring and increase the risk of infection because of skin breakdown, which is the first line of defence in preventing infection. Morbidity may increase as a result of significant skin injuries that become infected in at-risk patients.
Moreover, because of MARSI, organisations are impacted in different ways such as:
- Increased length of stay, impacting on bed capacity
- Potentially longer community treatment times
- Increased health professional time
- Increased use of resources and dressings and associated consumables (Collier, 2019; Hadfield et al, 2019).
Prevention
Prevention is better than cure and this should be the focus of practitioners in preventing MARSI.
Skin care is one of the single most important things that can be done to prevent any skin damage. Patients and health professions each play a role in maintaining healthy skin. Fumarola et al (2020) highlight the need for good skin care. Examples of good skin care are shown in the Table 2.
Table 2. Examples of good skin care that will help maintain skin integrity
Incorporate good skin care into daily routine:
|
Hydrate the skin and body (moisturise the skin daily and ensure the patient drinks enough water to prevent dehydration):
|
Avoid using alcohol-based products, perfumes, dyes or harsh soaps:
|
Use emollients as a moisture barrier:
|
Handle skin with care:
|
| Avoid clothing that scratches the skin, causes itching or puts pressure on the skin |
Encourage patients to adhere to the following sun care recommendations:
|
Source: Fumarola et al, 2020
Adhering to the principles of good skin care will help maintain skin integrity so it is optimal when an adhesive is required.
If a skin decontamination product has been used, the skin must be allowed to dry completely before any medical adhesive is applied, for example to secure a wound dressing or vascular access device. This is for two reasons. First, the medical adhesive will not adhere to the skin if the skin is wet and, second, there may be an iatrogenic relationship between the properties of the medical adhesive and the skin decontamination product that increases the risk of skin damage, predisposing a patient to developing MARSI (Hitchcock and Savine, 2017).
Three main types of adhesives are used in medical devices: silicone; acrylate; and hydrocolloid (Table 3). Adhesion to the skin can vary between medical adhesives, and their modes of action are different. Acrylate adhesives fill the gaps between the adhesive backing/device and the skin's irregular surface, and the strength of the bond increases over time, while silicone-based adhesives are softer and gentler, and maintain a constant level of adherence over time (Fumarola et al 2020). It is important to apply the medical adhesive correctly according to the manufacturer's instructions to ensure it remains in situ for the intended duration.
Table 3. Type of adhesive used in medical devices
| Type | Advantage | Disadvantage |
|---|---|---|
| Silicone |
|
|
| Acrylate |
|
|
| Hydrocolloids |
|
|
Source: Fumarola et al, 2020
Appeel Sterile Medical Adhesive Remover
Medical adhesive removers are important and have been shown to be effective (Collier, 2019; Evans, 2019; Hadfield et al, 2019; Barton, 2020). Appeel Sterile Medical Adhesive Remover is a silicone-based, no-sting remover that can assist in the removal of any medical adhesive, preventing pain and discomfort for the patient (Collier, 2019; Barton, 2020). Appeel Sterile Medical Adhesive Remover dries quickly and, once the medical adhesive is removed, it does not prevent reapplication of a medical adhesive at the same site (case study by Hitchcock in Collier, 2019).
Appeel Sterile Medical Adhesive Remover comes in a variety of forms: foam applicator; wipe; liquid sachet; and in a 100ml spray can. This allows the health professional to choose the right application for the intended purpose depending on the site and area of medical adhesive that requires removal.
The consensus document recommends the use of sterile medical adhesive removers to prevent injury to the skin from medical adhesive removal. It says they should be used in clinical areas where high-risk patients are treated, and that the decision to use a sterile medical adhesive remover is a clinical not a procurement decision. In addition, where there is no difference in cost between sterile and non-sterile medical adhesive removers, sterile medical adhesive removers should be considered as part of the risk management process (Fumarola et al, 2020).
Patients at a high risk of infection should have a sterile medical adhesive remover used to prevent MARSI. These patients include those with open wounds, vascular access devices (in particular central vascular access devices), immunocompromised patients and the very young (neonates, including very low birthweight babies) and the elderly (Table 1) (Fumarola et al, 2020).
An example of a flowchart that allows healthcare practitioners to follow a simple process to ensure dressings are removed correctly, using a medical adhesive remover and a skin barrier protectant before applying the dressing, is illustrated in Figure 1.
Figure 1. Dressing removal process
The correct application and removal of any dressing is vital in preventing MARSI and is detailed in Table 4.
Table 4. Application and removal of dressing to prevent MARSI
| Application | Removal |
|---|---|
|
|
Source: Fumarola et al, 2020
Case study 1. Treatment of sacral wound for 8 months
Ms Smith (not her real name) is a 28-year-old woman who was admitted into the intensive care unit (ICU) of Guy's and St Thomas' NHS Foundation Trust, with sepsis of unknown origin. She has a medical history of congenital nephrotic syndrome, kidney transplants in 1998 and 2007, new-onset diabetes after transplantation and a sacral nerve stimulation implant.
Ten months before admission, Ms Smith had developed lesions to her hands, arms and legs and was being reviewed by the dermatology department. She had a diagnostic punch biopsy taken from one of the lesions on her hand and, while this was histopathologically inconclusive, a provisional diagnosis of ecthyma (a deep form of impetigo) was given.
Shortly after admission into ICU, Ms Smith developed two lesions over her sacrum, which were reviewed by the tissue viability team. The lesions were atypical of pressure damage including deep tissue injury, so the dermatology department was asked to review.
Over a period of 2 weeks, the lesions became necrotic and coalesced. A microbiological swab of the wound identified Pseudomonas aeruginosa bacteraemia, which is commonly found in ecthyma gangrenosum wounds. Further lesions developed on her left lower leg, which led to an above-knee amputation under the care of vascular surgeons.
The tissue viability team, with the support from the plastic surgery team, managed the sacral wound. Wound management was further complicated by the implanted sacral nerve stimulator. This might have acted as a foreign body within the wound and may have caused the wound to become worse or delayed healing.
Because of the severity of Ms Smith's illness, a multidisciplinary team meeting decided that the wound would be conservatively managed via autolytic rather than surgical debridement. The plastic surgery team did, however, undertake some conservative bedside sharp debridement and the sacral nerve stimulator was removed in theatre with some limited debridement of the wound.
 Figure 1. Devitalised sacral wound
Figure 1. Devitalised sacral wound
The tissue viability team decided that, because the first wave of Covid pandemic was causing a continual disruption of supplies, the dressing regimen would use dressings that were readily obtainable and widely used om the trust and with which the large number of surge nurses rotating through ICU would be familiar.
This meant that dressings reputed to have gentler adhesives were not used, which increased the possibility of medical adhesive-related skin injury (MARSI) to the periwound area. The periwound area was treated with a barrier film spray to protect against maceration induced by wound exudate. The wound was cleaned with an antimicrobial soak to reduce bacterial colonisation and contamination of the wound bed. The primary dressing was medical-grade honey and hydrofibre to encourage autolytic debridement. A simple absorbent pad was applied as the secondary dressing and retained with an adhesive semi-occlusive film dressing to prevent contamination.
The dressing regimen was reviewed following the second wave of Covid, when supplies had stabilised. Ms Smith was transferred to a medical ward. The dressing regimen now incorporated an adhesive silicone foam dressing with a gentle border instead of the absorbent pad and semi-occlusive film.
Because of the frequency of honey application requested by TVN and the exudate produced, the dressing was changed three times weekly or more often if there was strikethrough or if the dressing became faecally soiled.
The film dressing had a firm adhesive. This meant that, while the dressing remained intact and prevented faecal contamination, the skin was at risk from MARSI during changes. This would be further compounded if the periwound skin developed any degree of exudate-related skin damage.
The tissue viability team had used Appeel Sterile Medical Adhesive Remover for a number of years and the bedside staff were instructed to use it at all dressing changes. The liquid sachets of Appeel Sterile, which incorporate a flow restrictor, were considered easier to use and more efficacious than wipes in releasing the adhesive bond of the film dressing.
 Figure 2. Granulating sacral wound post 8 months following alternate day dressings
Figure 2. Granulating sacral wound post 8 months following alternate day dressings
Ms Smith, when asked, reported that the dressing changes were mainly atraumatic and that the discomfort came from the lateral positioning she had to be in for the dressings to be changed.
The effectiveness of Appeel Sterile Medical Adhesive Remover can be viewed in that Ms Smith had alternate daily dressing changes (which included removal of a firm adhesive film dressing) for 8 months. Not only was the integrity of the periwound area maintained but also the friable new epithelium was not degraded, indicating in the author's opinion that MARSI was greatly prevented with the use of Appeel Sterile Medical Adhesive Remover.
Case study 2. Wound with a fistula after multiple surgery
Mrs Brown (not her real name) is a 66-year-old inpatient on an acute colorectal ward who has undergone complex abdominal surgery, including abdominal wall reconstruction and enterocutaneous fistula (ECF) repair. She has multiple comorbidities, including diabetes and chronic obstructive pulmonary disease. In addition, she is a heavy smoker, which is a significant risk factor for delayed healing and wound infection.
Mrs Brown has had multiple ECF surgery repairs in the last few years. After surgery she had an abdominal wound dehiscence (25 cm length x 27 cm width x 2 cm depth) and an ECF, which developed two weeks postoperatively, exposing two loops of small bowel within the wound.
The wound and ECF were managed with negative pressure wound therapy (NPWT) using a silicone isolator for the fistula. This is a complex scenario with a fistula within a wound, where leaks are likely to happen, as well as contamination of the wound with bowel output.
Multiple comorbidities and the nature of the wound made this patient vulnerable to skin infection from contamination and to medical adhesive-related skin injury (MARSI) as a result of already fragile skin and multiple previous surgeries to the same part of the abdomen and skin. Mrs Brown also has a stoma and the wound was very close to it (Figure 1). The pain from the wound and surrounding skin was rated at 8 out of 10 on the visual analogue scale (VAS).
 Figure 1. Large abdominal wound dehiscence and enterocutaneous fistula, with stoma in close proximity
Figure 1. Large abdominal wound dehiscence and enterocutaneous fistula, with stoma in close proximity
A hydrocolloid dressing was needed for the surrounding skin as skin stripping was caused by dressing removal and leaks from the fistula and stoma into the wound. Dressing removal took a long time, sometimes up to 20 minutes, and the pain was unbearable (10 out of 10) and caused anxiety to the patient before and after the process. The patient was reluctant to have dressing changes because of past MARSI and pain, and had to be given nitrous oxide during every dressing change.
No medical adhesive remover had previously been used. Appeel Sterile Medical Adhesive Remover Spray was considered as an option to avoid trauma, skin stripping and pain on dressing removal.
Appeel Sterile Medical Adhesive Remover is alcohol free, has a non-sting formulation and can be used on injured skin. Using Appeel Sterile Medical Adhesive Remover Spray at the next dressing change allowed the dressing to be unpeeled easily, without skin stripping. Appeel Sterile Medical Adhesive Remover Spray can be sprayed at any angle, allowing access to hard-to-reach areas.
The patient described the removal of the dressing as ‘tender and cold’ but not painful, and it took only 5 minutes. The wound was cleansed and a protective barrier film spray was applied to the surrounding skin to protect it through creating a skin barrier.
Mrs Brown reflected that the Appeel Sterile Medical Adhesive Remover Spray made a difference to her mood and reduced her anxiety. The dressing regimen continued with NPWT and the isolator. Appeel Sterile Medical Adhesive Remover continued to be used three times a week over the following 6 weeks to reduce pain at dressing removal and protect surrounding skin. Appeel Sterile Medical Adhesive Remover did not affect the adhesion of the replacement dressing. The wound improved and there was no skin stripping or redness to the surrounding skin (Figure 2).
 Figure 2. Negative Pressure Wound Therapy in place using silicone isolator for enterocutaneous fistula
Figure 2. Negative Pressure Wound Therapy in place using silicone isolator for enterocutaneous fistula
Pain during and between dressing changes reduced to 3 on the VAS, so nitrous oxide was not needed after 1 week of using the Appeel Sterile Medical Adhesive Remover Spray. Appeel Sterile Medical Adhesive Remover was easy to use and has assisted in achieving atraumatic dressing removal.
Case study 3. Moisture damage
Mrs Davis (not her real name) is an 83-year-old lady with mild moisture damage to her sacrum and bilateral ischial tuberosity area. Skin to this area is usually unbroken. It was classified as mild as it affected less than 50% of the surface area. She is incontinent of urine due to poor mobility and wears incontinence pads. She has rheumatoid arthritis, but chose not to take any medication to manage it. Her advancing age and incontinence put her skin at greater risk of skin damage.
Her skin care regime is managed by the district nursing team and carers. It includes the use of an emollient ointment as a soap substitute to the areas affected by moisture damage as per local trust guidelines, plus the use of a barrier cream daily. Usually, the skin is well maintained, but a recent episode of diarrhoea had caused a break in the skin, which had become infected and was causing a great deal of discomfort. This break in the skin was due to the excoriation caused by the diarrhoea and not pressure. When urine and faeces come into contact with the skin it causes a change in the skin's pH balance, which causes the skin to become red and irritated.
The district nurse decided to apply a soft silicone adhesive dressing to stop faeces coming into contact with the wound and to prevent further damage to the broken skin. Other methods of protecting the wound, such as film dressings and skin protectant spray had previously been used, but were ineffective. The rest of the sacrum and ischial tuberosity areas were treated with a barrier film spray again as per local trust guidelines. The affected areas were regularly washed with warm water and the emollient ointment and she was encouraged to try and use the toilet more often.
There was concern that using an adhesive dressing on skin damaged by moisture could cause skin stripping. Therefore, Appeel Sterile Medical Adhesive Remover Wipes were used when removing the dressings with the aim of preventing a medical adhesive related skin injury (MARSI) and to provide comfort during dressing removal.
Figure 1 shows the affected area before the use of Appeel Sterile Medical Adhesive Remover Wipes. The redness is from the moisture damage and there is a small break in the skin (1cm x 1cm) due to diarrhoea affecting the skin's integrity. The district nurse intended to leave the dressing on for up to 7 days as indicated for its use, but due to the faecal soiling it had to be changed daily. Prior to using the Appeel Sterile Medical Adhesive Remover Wipes, removal of the dressing was not only painful and distressing for the patient, but also caused trauma on removal. The skin where the adhesive had come into contact had started to bleed due to the skin stripping at dressing removal.
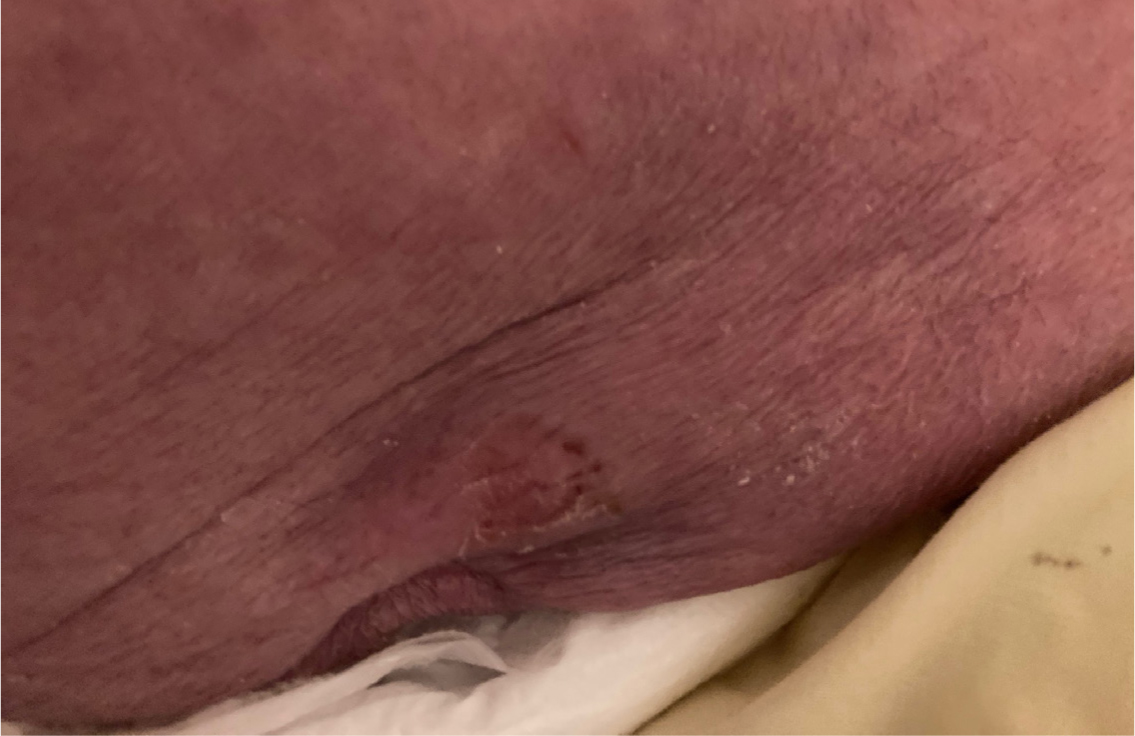 Figure 1. Sacrum before use of Appeel Sterile Medical Adhesive Remover Wipes
Figure 1. Sacrum before use of Appeel Sterile Medical Adhesive Remover Wipes
The nurse chose Appeel Sterile Medical Adhesive Remover Wipes to facilitate removal of the adhesive dressing and to reduce pain levels. The wipes, in particular were chosen as they could be used directly on the area where the adhesive part of the dressing attached to the patient's skin. Appeel Sterile Medical Adhesive Remover Wipes are alcohol free, and therefore should not cause any stinging to the surrounding skin.
The patient commented that she found the Appeel Sterile Medical Adhesive Remover Wipes had reduced the pain during dressing removal. The nurse found that Appeel Sterile Medical Adhesive Remover Wipes did not cause any trauma to the skin where the dressing had been. This permitted the areas which had previously shown signs of skin stripping to improve, and prevented any further skin damage occurring. This in turn allowed the dressing to be used over the area of broken skin to prevent contamination from the faecal soiling.
Figure 2 shows the affected area following a week of Appeel Sterile Medical Adhesive Remover Wipes usage. The area of broken skin is still present; however, being able to cover this area with a dressing to prevent contamination from the diarrhoea was essential to the patient's health and wellbeing. Infected wounds can cause distress, pain and discomfort to the patient and can be very challenging for health professionals in terms of management, cost and time.
 Figure 2. Sacrum after use of Appeel Sterile Medical Adhesive Remover Wipes
Figure 2. Sacrum after use of Appeel Sterile Medical Adhesive Remover Wipes
Conclusion
Prevention of MARSI is essential in maintaining skin integrity to prevent complications associated with the breakdown in the skin's normal function, which can result in pain, infection and delays in healing. Accurate skin assessment for all patients before the correct application of a medical adhesive device with a skin barrier film and the correct removal technique of a medical adhesive device (which includes the use of a medical adhesive remover) as recommended by the consensus panel on prevention of MARSI should be adopted in healthcare whenever a medical adhesive is used.
KEY POINTS
- Adhering to the principles of good skin care will optimise the skin preventing skin damage
- The use of a medical adhesive remover can assist in removing dressing thus protecting the skin
- Sterile medical adhesive removers are recommended for high-risk patients
- Use evidenced based information to develop an algorithm for applying and removing dressings, using the most appropriate products to prevent medical adhesive-related skin injury
CPD reflective questions
- In your clinical setting do you think dressings are applied and removed correctly?
- How can you prevent medical adhesive-related skin injury (MARSI) in your patients?
- What changes can you make in your clinical setting to ensure preventing MARSI can be adopted in practice?
- Consider writing a reflective piece on a patient where you have seen them get MARSI with a dressing.