
Following the introduction of a range of silicone-based stoma care accessories, Trio Healthcare is further developing its range of novel silicone-based adhesive stoma products. This includes stoma appliances made from a unique patented formulation, known as Sil2™ technology, that has been designed to maintain skin health by allowing the skin to breathe. As the use of silicone technology in stoma care is new, it has raised a number of questions among stoma care nurses. This Q&A draws on clinical evidence and the author's experience as a specialist stoma care nurse to answer these questions and help nurses select and use the most appropriate appliance for their patients.
What makes silicone an appropriate material for use in stoma appliances?
Silicone is widely used in wound care, continence and stoma care accessories, due to its inert, waterproof, non-toxic, non-odorous and hypoallergenic qualities. These properties also make it a safe and effective material for stoma appliances.
Many ostomates have an abdomen with an uneven surface for the flange to adhere to, which can cause problems with leaks and subsequent sore skin. Silicone polymers are extremely malleable and so can be easily moulded into creases and crevices around the stoma. This flexibility provides an excellent fit to the contours of the body and an effective seal against urine or faecal output (Meuleneire and Rücknagel, 2013).
Some silicones have been developed with adhesive properties, which allow a device to attach securely to the skin, preventing peeling or separation. Unlike other adhesive materials, soft silicones are less likely to deteriorate, and they do not leave a sticky residue (Burch, 2011). Sil2 has been especially modified to allow it to sustain a persistent level of adherence over time, as well as making it softer and gentler on the skin (Fumarola et al, 2020). These properties make silicone an effective material for products designed to meet the needs of ostomates and stoma care nurses.
Why should nurses consider changing from a familiar material that they already know to be effective?
Experienced stoma care nurses will understand that no two patients are the same. An appliance that has had fantastic results on one patient may not be as effective on another, and so stoma care nurses and ostomates may need to try products from several companies before finding the right one (Sica, 2018). Stoma care nurses need to be aware of the full variety of stoma appliances available, including one-piece and two-piece systems, each designed to accommodate different body shapes and types of stomal output. Finding the correct appliance can make a significant difference to a patient's quality of life.
To achieve this, the manufacturers of stoma appliances need to be innovative, creating new technologies to develop more effective products for ostomates and stoma care nurses to use. Furthermore, innovation also requires practitioners and users to be open-minded and willing to compare all available options. Part of this is the recognition that established technologies may not be perfect and often have drawbacks that can be improved on.
One such example is moisture management in stoma appliances. Normally, moisture on the skin is lost via evaporation, and this is known as trans-epidermal water loss (TEWL). This presents a challenge for occlusive devices that cover the skin for prolonged periods, because this will prevent TEWL and trap moisture in the skin, unless the technology has an effective method of moisture management. This is vital in stoma care, because peristomal skin, the area of skin around the stoma that is covered by the flange, is exposed to biochemical and mechanical stresses on a daily basis, and these can damage the skin's defensive, sensatory and regulatory functions (Nichols, 2018). Peristomal skin damage is a common, painful and debilitating issue that significantly impacts 70% of ostomates (Gray et al, 2013).
What specific drawbacks are there to established hydrocolloid stoma appliances that could be improved on?
Traditional hydrocolloid stoma appliances manage the issue of TEWL by absorbing moisture from the peristomal skin directly into the flange (also known as the baseplate). However, the hydrocolloid flange retains this moisture against the skin, where, over time, it has the potential to cause moisture-associated skin damage (MASD). MASD refers to skin damage caused by excessive or prolonged contact with moisture. This may be secondary to contact with stomal output, wound exudate, faeces, urine, sweat, mucus or saliva. MASD can be divided into four categories (Box 1). Some degree of peristomal skin damage has been reported by 62% of all ostomates (Nichols, 2018), and peristomal MASD was three times more common in ileostomates than in colostomates (Nagano, 2019).
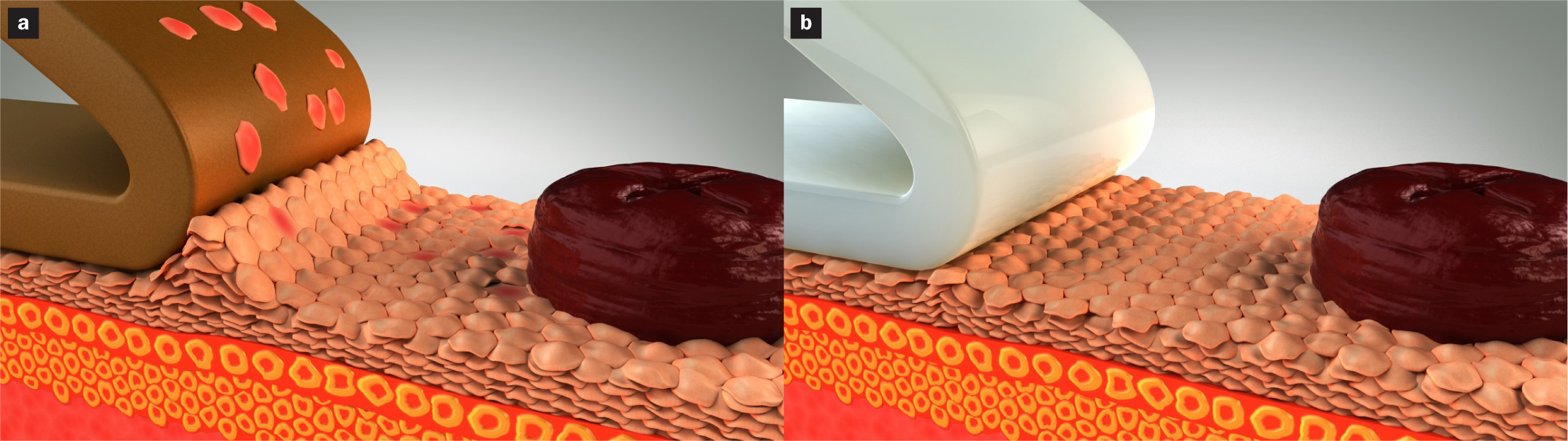
Additionally, this absorption of moisture into the hydrocolloid increases its adhesive strength. This makes the flange harder to remove, which, over time, may cause peristomal medical adhesive-related skin injury (MARSI) (Figure 1). MARSI is characterised by erythema, blisters, erosion and/or skin tears that continue for 30 minutes or more following removal of an adhesive device (Le Blanc et al, 2019). Peristomal MARSI is caused by excessively frequent or traumatic removal of a stoma appliance flange. Therefore, the more often an ostomate removes their appliance, and the stronger its adhesive properties at the time of change, the more likely they are to develop a peristomal MARSI. Studies have suggested that the prevalence of MARSI among ostomates could be as high as 54% (Fumarola et al, 2020).
‘The prevalence of MARSI among ostomates could be as high as 54%’
These issues present the need for a more effective stoma appliance that can prevent the build-up of moisture on the peristomal skin, increase wear time and decrease the incidence of peristomal complications, including MASD and MARSI.
If silicone does not absorb water, how can a silicone stoma appliance prevent the skin becoming damp and excoriated?
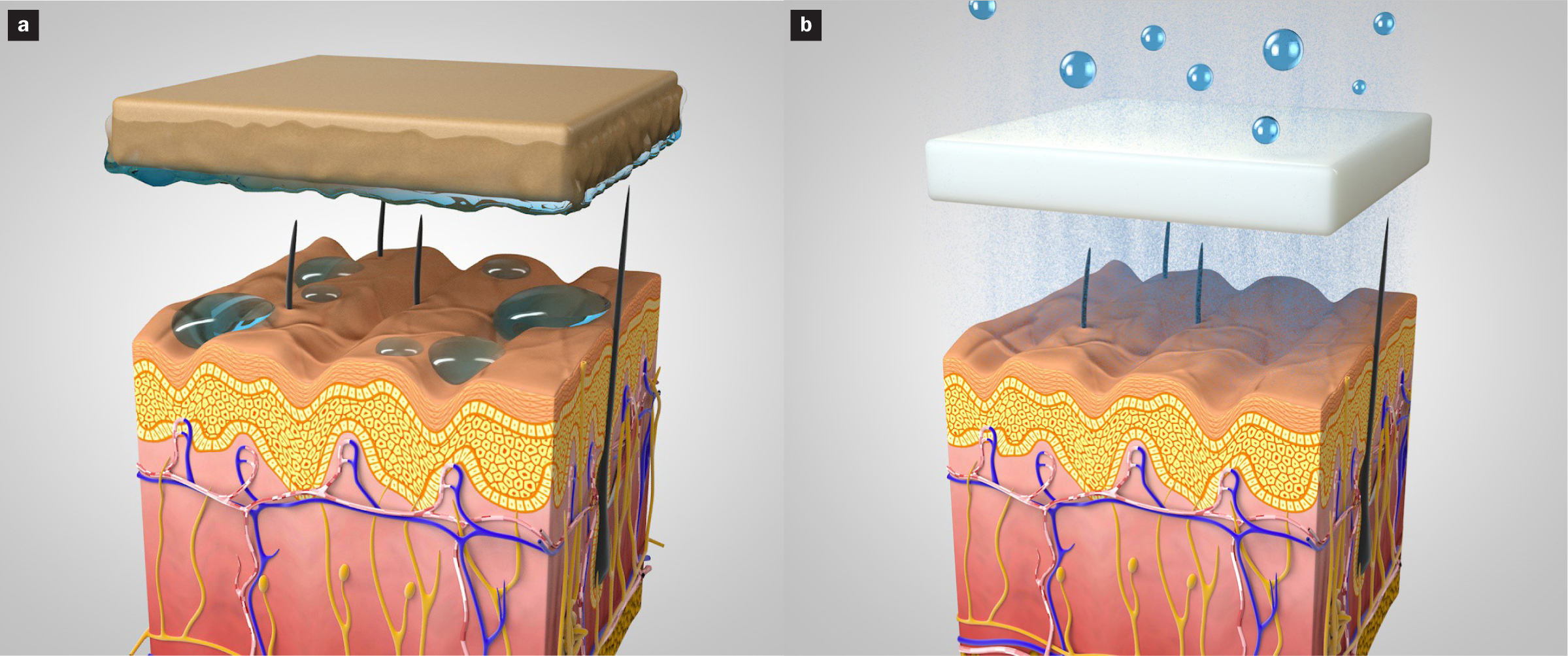
The appliances developed by Trio Healthcare and the University of Bradford Centre for Skin Sciences have a distinct evaporation-based mechanism of moisture management. They are made from a unique silicone compound, Sil2, which is different to the silicone used in other silicone devices (for example, in wound dressings). This novel formulation has been modified with the introduction of compounds that aid colloidal separation, which allows water vapour to find a path through the material (Figure 2). This has been used to create breathable stoma appliances that allow moisture to escape from the surface of the skin, through the flange and into the air. Because the water vapour passes through the silicone and into the air, the moisture is not held in the device, and, therefore, there is none of the permeation, engorgement or increased adhesion typical of hydrocolloids. Unlike the absorption process in a hydrocolloid flange, Sil2 also adapts to differences in moisture levels, allowing moisture vapour through, thus maintaining the skin under the flange at a normal healthy moisture level (Swift et al, 2020).
What unique benefits does a silicone appliance have for the patient that give it an advantage over existing options?
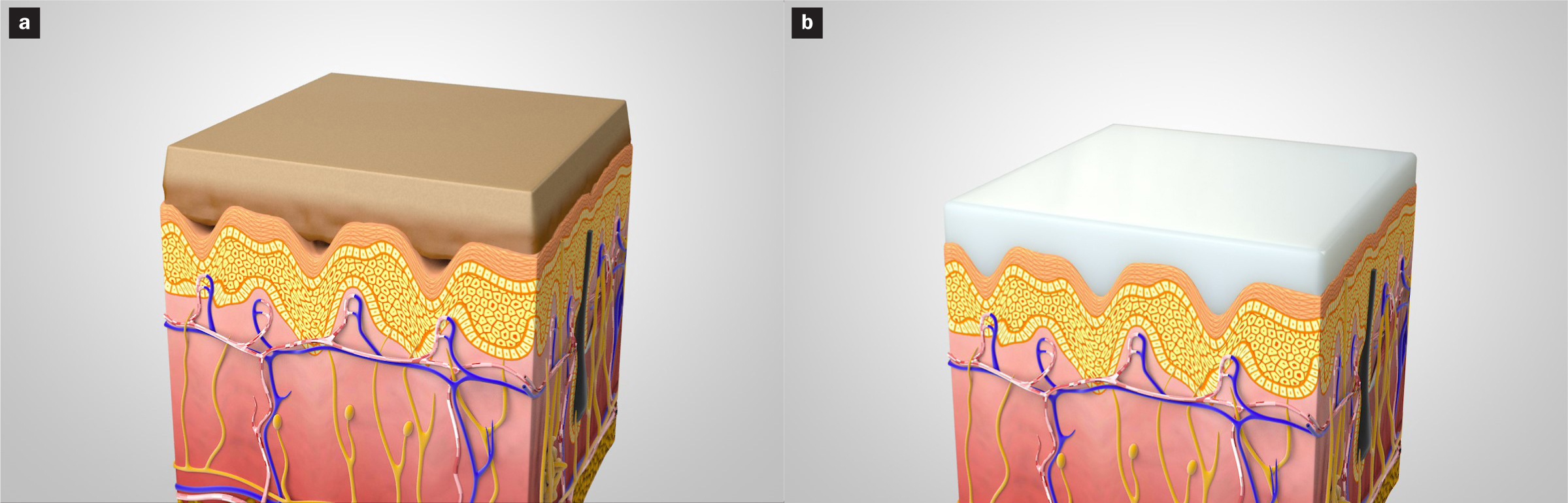
The effective and novel moisture management system of silicone appliances can provide a more natural moisture level for the peristomal skin, reducing the risk of MASD. The naturally hydrophobic material means that the appliance keeps a constant shape and does not swell, deform or break down. Likewise, its adhesive properties remain stable over time, providing an appliance that can be removed safely with no increased risk of MARSI (Figure 3). All of these properties can provide an extended wear time, adding up to an appliance that is comfortable and dependable for the patient, as well as cost-effective for the health service. The Sil2 products would be an especially appropriate choice for ostomates who are experiencing sore skin due to contact dermatitis resulting from effluent that has been absorbed in the hydrocolloid flange, as they would provide protection and respite for the skin. They have been developed to not absorb moisture, such as sweat and stomal output, throughout the day, which helps maintain skin integrity and prevent peristomal skin damage.
Because silicone is more flexible than hydrocolloid, a Sil2 appliance is better able to mould into the dips and creases of an uneven skin surface. This increases the overall contact area between the adhesive appliance and peristomal skin, distributing the necessary adhesion across a greater number of skin cells and thus reducing the likelihood of traumatic removal and MARSI (Figure 4).
Which patients are suitable for silicone appliances, and do they have any specific limitations?
Silicone appliances are suitable for most ostomates, including those with challenging stomas. This includes people whose stomas have sunk deeper into the skin, as the softness and flexibility of the flange allows it to be moulded around the recessed stomas, which provides a snugly fitting barrier that offers added security and confidence. In older patients, the gentleness of silicone, compared with hydrocolloid, makes it an effective covering for thin and fragile skin, which is at high risk of skin tears (Hadfield, 2019).
Sil2 should not be used in the rare cases of patients who have an allergic reaction to the silicone or any of its other ingredients. A patch test can be carried out for patients who are known to have sensitive skin. Silicone is hypoallergenic by nature, and allergy is very rare, making it a comprehensively suitable material for adhesive and protective therapeutic devices. However, as will be familiar to experienced stoma care nurses, there will be some challenges where finding the most effective solution requires trial and error.
Can silicone appliances be used on moist and/or excoriated peristomal skin?
As with all existing appliances, getting it right can be particularly challenging if the peristomal skin is excessively moist. A flange of any material (silicone or hydrocolloid) will not effectively adhere to moist skin without the skin being dried first.
Before using any kind of appliance, stoma care nurses and ostomates must be able to identify wet and sore peristomal skin, which may show signs of redness, inflammation and swelling, as well as, in severe cases, development of blisters (Voegeli, 2019).
There are several comprehensive assessment tools that stoma care nurses can use at each assessment to monitor deterioration or improvement in peristomal skin health and objectively evaluate the efficacy of interventions (Table 1). It is also worth assessing the social and emotional impact of peristomal complications. Stoma care nurses often hear patients saying that they are scared to go out, as they are frightened that their appliance will leak. This often seems to concern ostomates more than the peristomal skin soreness, although these issues usually go hand-in-hand. Ostomates can also be encouraged to monitor their own peristomal skin health, using a variety of online resources and visual aids available for self-assessment (Coloplast, 2020).
| Tool | Areas of assessment | Source |
|---|---|---|
| Ostomy Skin Tool | Clinical observation of discoloration, erosion/ulceration and tissue overgrowth (0–15) | Martins (2010) |
| Peristomal Skin Soreness Tool | Severity and contributing factors of moisture-associated skin damage | Association of Stoma Care Nurses UK (2017) |
| Stoma Care Ostomy Research Tool | Stoma size, shape and output and changes in body weight, skin elasticity and muscle tone | Williams (2010) |
| Ostomy Leak Impact Tool | Burden of leakage (emotional impact; usual and social activities; coping and control) | Nafees et al (2018) |
In order to optimise adhesion on sore, wet, macerated peristomal skin, the surface must be gently cleaned with plain water and then dried, bearing in mind that this maybe very painful for the ostomate. A common treatment for MASD involves applying calamine lotion or a hydrocolloid powder (Metcalf, 2018). The hydrocolloid powder adheres to the broken skin, forming a tacky layer that soaks up moisture and creates a dry surface for adhesion (Evans and Burch, 2017). However, ostomates should be made aware that overenthusiastic application of this powder could have the opposite effect, weakening rather than improving adhesion on the skin. Appliance adhesion can also be increased by using one of an array of barrier sprays and wipes to create a protective film over the skin. There are silicone-based skin barrier films available, which have the advantages of not stinging on application and drying quickly. When peristomal skin is too sore to touch, the use of a barrier spray rather than a wipe avoids adding to the pain levels, as there is no need to touch the skin during application (Bibi, 2019). These interventions should suffice to apply a flange to excoriated peristomal skin; however, in extreme cases of highly excoriated, wound-like skin, another approach may be required. It is worth noting that application of silicone skin barrier films can increase the adhesion of the appliances, and, therefore, adhesive remover may be required to avoid further injury.
How can stoma nurses know whether silicone appliances are a safe, appropriate and effective choice?
Any new product must be based on robust evidence that is fully transparent to users. Moreover, companies must afford proof of the efficacy of a new product, be able to define the difference between products and offer samples so that stoma care nurses are able to assess the product independently (Bibi, 2019). Ostomy products are regulated by the Medicines and Healthcare products Regulatory Agency (MHRA) and the Drug Tariff, and so their safety and efficacy must be demonstrated before they are approved and brought to market. Manufacturers are also legally obliged to undertake post-marketing surveillance to ensure their products are being used safely and effectively. Engaging with the emerging evidence on new technologies is a key part of the duty of care that stoma care nurses have to their patients, as it is essential for finding the most appropriate appliance for each individual.
The safety, efficacy and relevance of silicone are indicated by transferable evidence from wound care, continence and stoma accessories. In wound care, silicone's adhesive properties have made it a popular material for dressings, compared with other substances that can cause pain and further damage to the wound (Meuleneire and Rücknagel, 2013). Silicone wound dressings are used extensively by a variety of manufacturers, including Molnlycke (2020), which reports that 4 billion silicone dressings have been used on over 100 million patients over the past 30 years. In continence care, the biocompatibility of silicone catheters has proven to be gentle on the urethral mucosa (Nazarko, 2019).
In stoma care, there are many effective silicone-based accessories available, including stoma paste, adhesive removers, barrier films and barrier rings/seals. In my own experience, I have had excellent results using silicone-based adhesive removers and barrier films to treat painful, excoriated peristomal skin. Patients reported healed skin and no pain after just two or three applications of a sting-free skin barrier (Elisse, Trio Healthcare). I have also found silicone-based barrier rings (Siltac and Silvex, Trio Healthcare) to be effective on sore peristomal skin, providing a non-absorbent barrier for stomal effluent.
This transferable evidence and user experience have gone into devising innovative silicone-based stoma appliances, which will provide nurses and ostomates a more comprehensive choice to suit their needs. All this suggests that it will increase appliance wear time, reduce costs and improve patient quality of life and, most importantly, considerably reduce the occurrence of peristomal MARSI and MASD (Swift et al, 2020).
How can nurses determine which patients are most suitable for trying silicone?
At present, there is limited understanding of the application of silicone in stoma care practice. Therefore, in order to familiarise themselves with this new technology, nurses should try silicone appliances on ostomates with peristomal skin problems of mild-to-medium severity. Familiarisation, proficiency and confidence with silicone appliances will result in better patient outcomes.
Not only is it important for stoma care nurses to be informed of innovations in stoma appliances, it is also important for ostomates themselves to be kept updated on developments that could have a significant impact on their quality of life. In the author's own experience as the community stoma care nurse on an island off mainland UK, ostomates on the island find it difficult to attend stoma open days and participate in national stoma-specific support groups. However, there is a local support group, and together we hold a biennial stoma exhibition to give everyone on the island the opportunity to see, feel and try samples of new appliances and accessories. The hypoallergenic qualities of silicone make these products a suitable option for all ostomates to try, to see if they result in better outcomes and are preferable to established alternatives. We find that some ostomates are keen to try new things, while others are more reluctant and feel safer sticking with what they know, even if they are having problems. However, encouraging these patients to step outside their comfort zone and try new things can often resolve long-term challenges and improve their quality of life, particularly if they are experiencing problems with leaks and sore skin. Local ostomates have responded positively to silicone-based accessories in the past, and a similar response can be anticipated to silicone-based appliances. The best way to determine the suitability and efficacy of a device is to allow a patient to try it.