
Boyles and Hunt (2016) suggested that while:
‘Many patients will have to deal with problematic skin at some point, it should not be considered the acceptable norm as it can have profound impact on an individual's optimal physical, psychological and social functioning.’
Improving the quality and safety of healthcare is a system-wide priority. In times when the NHS is under substantial financial pressures to deliver efficiency savings, Getting It Right First Time (GIRFT) has never been more important. According to the website, GIRFT is:
‘…A national programme, led by frontline clinicians, created to help improve the quality of medical and clinical care within the NHS by identifying and reducing unwarranted variations in service and practice.’
The NHS is expected to deliver efficiencies of 2-3% per year, effectively setting a 10-15% real-terms cost-reduction target for achievement by April 2021, with the aim to make the NHS the safest and most efficient healthcare system in the world (Carter, 2016).
Considerations and patient safety
Fundamental to any patient intervention or project that has a clinical focus is the role and involvement of clinical governance. The systematic approach to embedding safety, effectiveness and experience into any intervention–be it face to face, written literature or product development–should be a conscious inclusion from the outset. If clinical governance is to truly function effectively, it requires collaboration and people to be in place to advocate and develop it further.
Many may view clinical governance as an abstract concept, however, once it is understood and accepted the advantages often become clear. Those who engage at an early stage benefit from thorough scrutiny and input that may have otherwise been overlooked. Clinical governance itself does not specifically mandate any particular structure for improvement in quality of care, except that the responsibility must exist, and it should be reviewed regularly to ensure that the structure remains robust and fit for purpose in meeting the needs of an organisation.
Risk management and patient safety is pivotal to the ethos of any clinician or clinical interaction and involves conscious consideration of the following:
Patient safety is defined as ‘the avoidance of unintended or unexpected harm to people during the provision of healthcare’ (NHS Improvement, 2019). Patient safety is an essential element of nursing care that aims to prevent avoidable errors and patient harm. It is a feature of a healthcare system and a set of tested ways for improving care. The Nursing and Midwifery Code (NMC) Code (2018) and the RCN Principles of Nursing Practice (RCN, 2019) promote patient safety. A change in culture is not a necessary precursor for changes in outcomes but it can determine the success and sustainability of patient safety initiatives.
The Care Quality Commission (CQC) has highlighted the need for a change in culture within the NHS to reduce the number of patients who experience avoidable harm. Everyone—including patients—can play a part in making patient safety a top priority. A change in approach is essential if we are to create a culture where learning is shared and where solutions are created proactively to manage risk (CQC, 2018).
Several reporting systems and schemes exist around the UK for reporting adverse incidents and near misses. Adverse incidents involving medical devices must be reported to the Medicines and Healthcare products Regulatory Agency (MHRA) reporting system. The MHRA is an executive agency of the Department of Health and Social Care in the UK that is responsible for ensuring that medicines and medical devices work and are acceptably safe.
A ‘CE’ mark is a logo that is placed on medical devices to show they conform to the requirements in the regulatory directives. It shows that the device is fit for intended purpose and meets legislation relating to safety. It shows the product can be freely marketed anywhere in the European Union (MHRA, 2016). The Yellow Card System is vital in helping the MHRA monitor the safety of all healthcare products in the UK to ensure they are acceptably safe for patients and those that use them (MHRA, 2019).
Clinical considerations for the ostomate population
In preparing and adjusting to life with a stoma, patients can often be anxious and will require support in adjusting to and living with a body-altering presence (Lim et al, 2015). Each person with a stoma is an individual and may react differently when faced with similar situations and as such needs to be considered individually to address their needs, support acceptance and encourage rehabilitation. Illness and stressful situations may impact upon a person's ability to engage fully at any given time and articulate problems or concerns (Poland et al, 2017).
There are 120 000 people in the UK with a stoma (Boyles and Hunt, 2016) and for each one maintaining an intact peristomal skin throughout their entire pathway and life with a stoma can be challenging.
The function of the skin
Boyles and Hunt (2016) concisely reported that the skin is:
Peristomal skin should have the same appearance as the rest of the abdominal area and should ideally remain intact and free from soreness. However, there are many factors both intrinsic and extrinsic that can damage peristomal skin; the contact of effluent and output from the stoma for prolonged periods can impact greatly on skin integrity.
The incidence of peristomal skin problems is widely reported in literature. However, many instances may be unreported, as often people living with a stoma—especially when well established and adjusted—will self-manage issues and only seek professional help when all other options have been unsuccessful. Studies suggest that a positive quality of life can be achieved when living with a stoma (Hubbard et al, 2017). However, if there is a loss of skin integrity, this can lead to possible issues which will impact on the adhesion of the stoma appliance, giving rise to leakage. This in turn will further impact on the skin integrity and influence the overall quality of that person's life (Erwin-Toth et al, 2012; Maydick-Youngberg, 2017).
Peristomal skin exposed to and in contact with urine and faecal matter can alter the balance of the skin's natural pH or acid mantle. In altering this balance, the skin will have a higher pH, making it more alkaline, which can increase the risks of skin irritation, breakdown and infection.
Another relevant skin function is that of transepidermal water loss (TEWL), which controls the amount of water transferred via the epidermis to the external environment. Gray et al (2011) discussed the impact that ‘skin-stripping trauma, infection, eczema and psoriasis’ has on the integrity of the skin, which causes an increase in TEWL action.
Peristomal moisture-associated skin damage (MASD) may be caused either by perspiration or the leakage of effluent underneath the flange. Over-hydrated skin, caused by prolonged exposure to moisture, may precipitate inflammation, which together with erosion to the skin occurs initially at the junction between stoma and skin, but can extend for up to 10cm from the stoma (Woodward, 2019).
Grey et al (2011) introduced the concept that MASD requires moisture and the addition of one or more attributable factors, which may include chemical irritants within the moisture source, its pH, mechanical factors such as friction and associated microorganisms.
A study undertaken to review the consequences of PSCs by Meisner et al (2012) concluded that a major focus was needed to minimise the risk, detect PSCs at an early stage and implement treatment to prevent the complications from worsening into a chronic, patient-impacting and expensive complication.
Sica (2018) suggested regularly reviewing whether a patient's pouching system can be improved, as the right appliance makes a vast difference to a patient's health, self-esteem and general wellbeing.
The aim of the study
Previous retrospective peristomal skin studies have been undertaken by the authors and presented to both World Council of Enterostomal Therapists (WCET) and European Council of Enterostomal Therapists (ECET) conferences. As with many studies, the evidence gathered and presented as a conclusion often raises more questions than answers and requires additional investigation.
The aim of this study was to collate outcomes from a real-life study collating evidence as to how SCNs:
Study design/methodology
The SCNs were introduced to the aims of the study and informed that the patient selection criteria focused solely upon the presence of PSC as identified during the physical review of the patient's stoma and discussions with the patient. No additional assessment tools or treatment pathways were introduced by the study.
The study used a questionnaire to capture details of the patient's PSC observed by the SCN, if the patient was deemed suitable to participate by the SCN and the patient gave consent to the SCN. The patient was shown the most suitable Manuka honey pouch (flat, convex or Profile), as clinically determined by the SCN.
The SCN and patient agreed a product evaluation period and also arranged to review the outcomes together. Following the outcome review, the second part of the questionnaire was completed by the SCN.
The end point of the study was to identify whether the introduction of a clinically appropriate pouch following ongoing assessment had a positive outcome in PSC.
The study outcomes focused on:
Once completed by the SCN, the questionnaire was forwarded by post to the authors.
Current practice baseline
The study consisted of 58 patients from across the UK, supported by 32 SCNs from 26 independent centres.
The study questionnaire captured a baseline recording of the extent of the PSC issues faced by the 32 SCNs within their nursing caseloads.
The most common attributes to PSC from their overall current caseload were:
Study findings
An overview of the study findings can be found in Figures 3 to 7.


The cohort demographics were:
Within the study cohort, the following accessory products were routinely used in conjunction with their stoma pouch:
The London Procurement Partnership (2018) recommended that prescriptions for accessory products including adhesive removers, skin protectors and adhesive discs/rings should be reviewed to ensure they remain effective.
The study results identify that the largest group of patients presenting with PSC had their stoma formed less than 18 months at the time of the review. Salvadalena (2013) stated
‘The most frequent time that the skin becomes sore is between 21 and 40 days after stoma formation’.
Lindholm et al (2013) stated that:
‘45% of patients experience problems with their stoma within the first 6 weeks after stoma formation.’
The peristomal skin complications described by the SCNs are shown in Figure 1.
Boyles (2018) described the complexity of describing PSC and suggests the descriptive approach of word choice like ‘sore’, ‘excoriated’, ‘red and broken’, ‘on the left or the right’, are highly subjective. She suggested that before descriptive word tools are used in practice, they need to benchmarked, audited and compared with those of others to improve care standards and outcomes.
One such tool that has been widely used within the specialty of managing the impact of incontinence upon the skin and one of the earliest scoring tools was developed by the National Association of Tissue Viability Nurse Specialists, Scotland (2009). The descriptor groups are listed in Table 1.
| Group | Inclusion |
|---|---|
| Healthy skin | Healthy, intact skin. No erythema (redness) |
| Mild excoriation | Excoriation erythema (redness) of skin only. No broken skin areas present |
| Moderate excoriation | Erythema (redness) with less than 50% broken skin. |
| Severed excoriation | Erythema (redness) with more than 50% broken skin. |
Adapted from NATVNS (Scotland) 2009
Current variations in descriptive terms are apparent across the 26 independent centres who participated within the study, as shown in Figure 2, which are the peristomal skin descriptors recorded by SCNs in this study. The skin descriptors were allocated into sub-groups; the terms and titles used have already been validated by a groups of SCNs and consensus gained as part of a previous study undertaken by the authors. Using the sub-groups defined, the SCNs’ peristomal skin descriptors were grouped into peristomal skin classifications as shown in Table 2.
Further analysis of the SCN's initial PSC assessment, identified that 47% of the cohort had severe peristomal skin damage (Table 3).
Bird (2017) said that the most effective way of reducing the cost of stoma care is to find the right appliance while acknowledging that if the ostomate is having persistent leaks or problems with sore skin something needs to change. Black (2018) further discussed the adverse impact that PSC can have on the patient's quality of life (QoL) citing Agarwal and Erlich (2010) who suggested that inadequate treatment of stoma-related problems may impact QoL while also increasing long-term treatment costs.
Product selection
The study methodology supported SCNs to independently identify patients with PSC, conduct a peristomal skin assessment and facilitate patient discussion as to the suitability of a change of stoma pouch to a medical-grade Manuka honey flange.
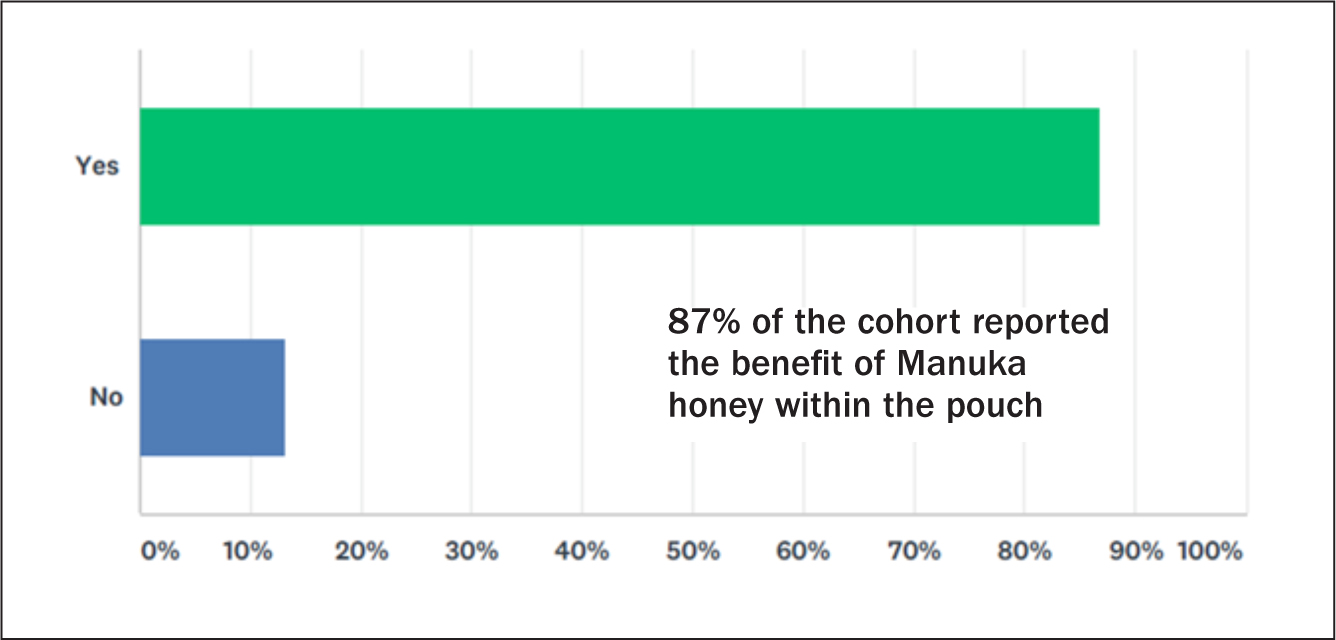
The value of Manuka honey has been described by Woodward (2019) who reported that:
The follow-up review date was determined by the SCN and the patient, the second part of the study evaluation sought confirmation from the SCN and patient when the peristomal skin improvement, if any, was first observed following the introduction of a medical-grade Manuka-honey flange.
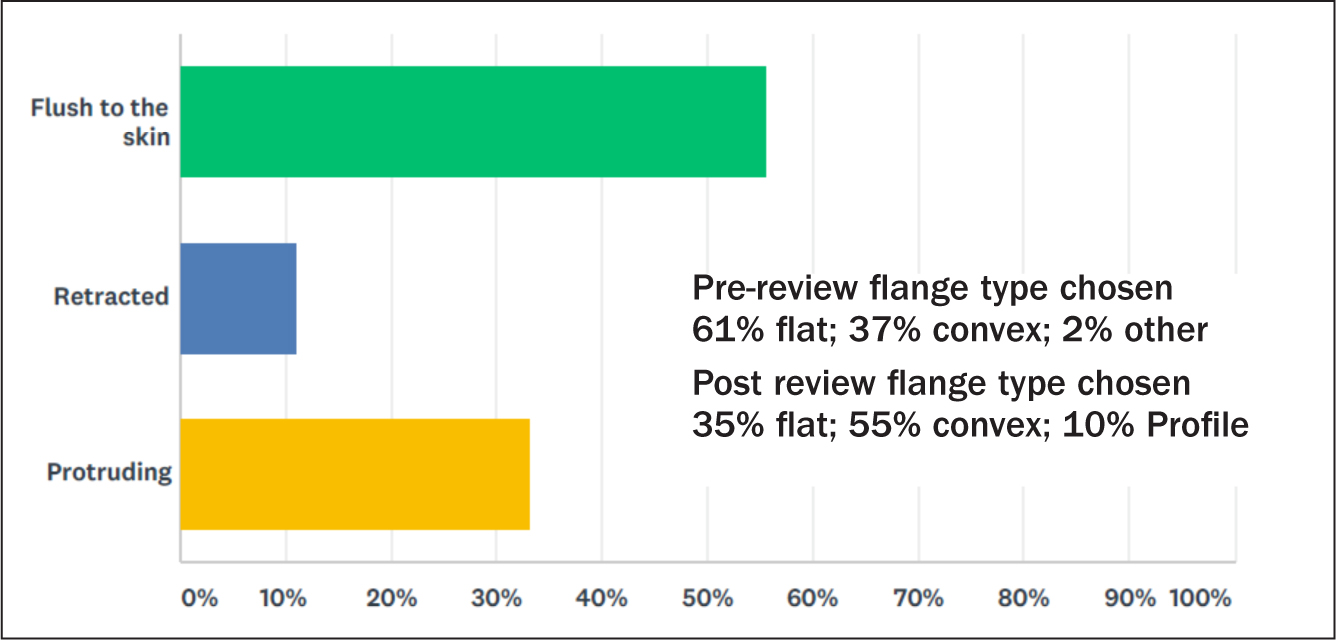
The SCN's reassessment of the patient's stoma recorded 56% flush to the skin, 33% protruding and 11% retracted, the treatment options chosen for the flange types used in the product evaluation reflect through a reduction of 26% of the flat flange type and patients were changed to a convex (18%) and Profile (8%) flange type.
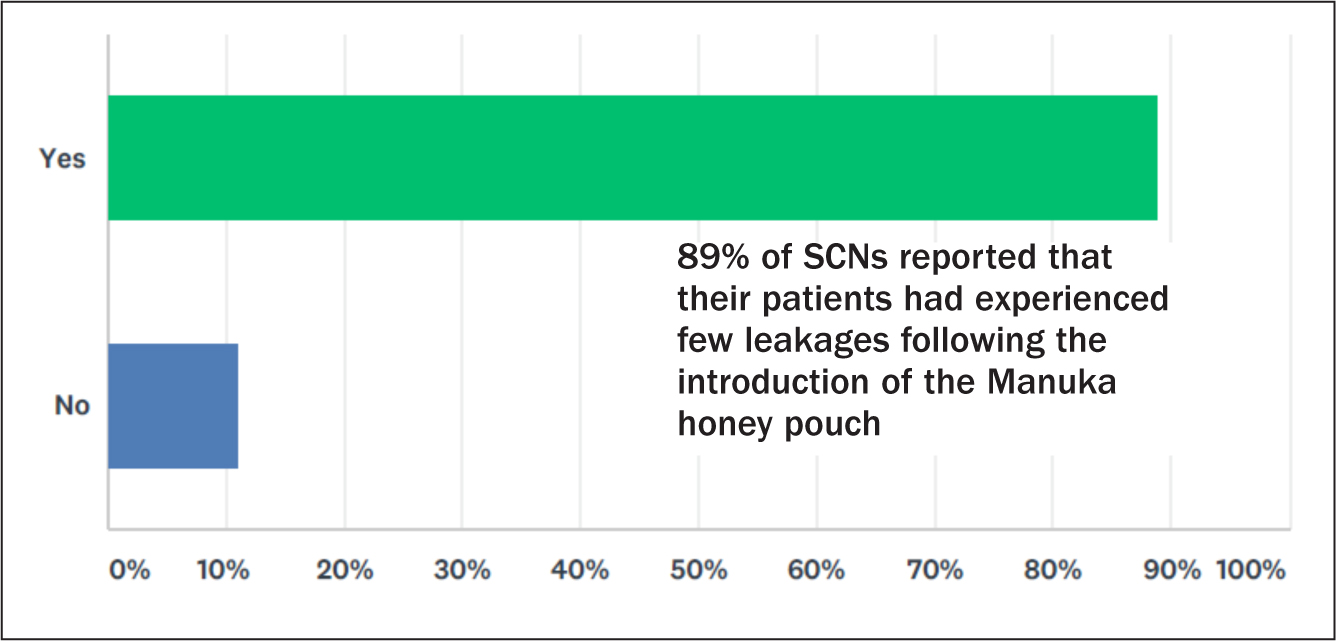
The importance of the SCN's reassessment of the stoma and type of flange used can be shown through the reduced leakage episodes experienced by the patients during the product evaluation. Of the SCNs, 89% reported that their patients had experienced fewer leakages following the introduction, where clinically appropriate, of a non-flat flange and in all instances a flange containing Manuka honey. This resulted in an increased pouch wear time for 62% of patients.
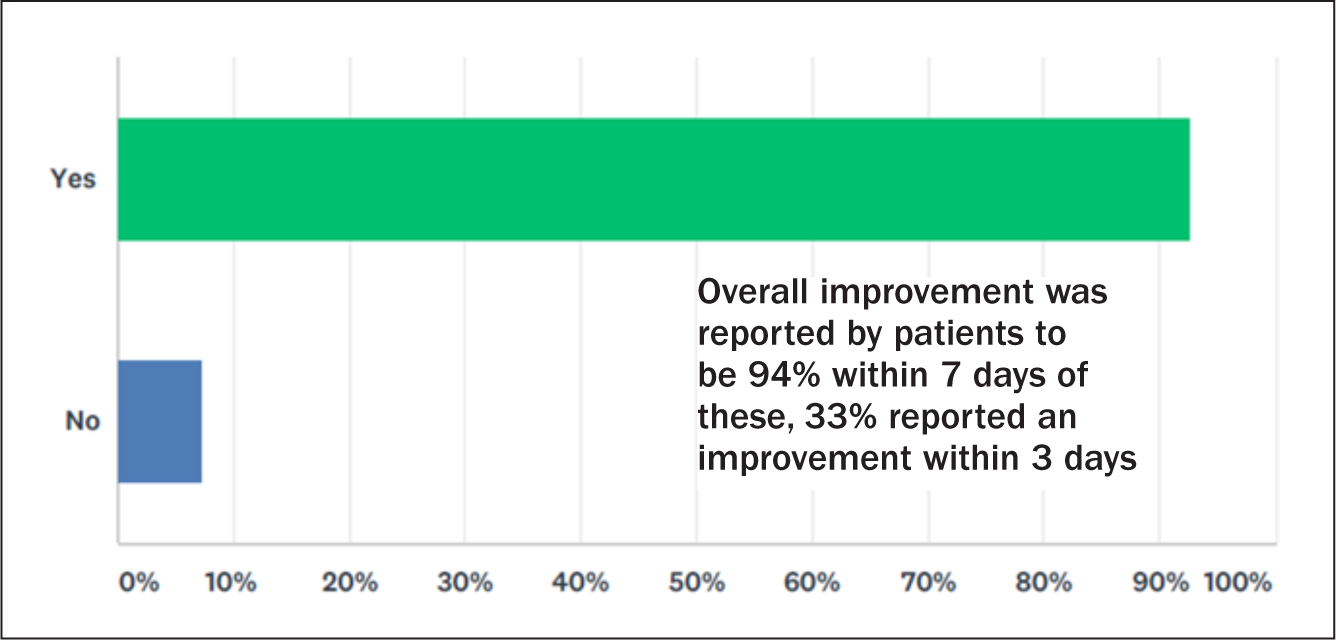
The overall improvement was reported by patients to be 94% within 7 days of these, 33% reported an improvement within 3 days.
Aminu et al (2000) claimed Manuka honey is a reliable alternative to conventional dressings for managing skin excoriation around stomas (ileostomy and colostomy) by facilitating epithelialisation of the damaged surface.
Patients were asked to describe their experience of using an adhesive flange containing medical-grade Manuka honey. The responses were positive and included perceptions and expressions of enhanced comfort, safety and security; feelings of confidence leading to a resumption of daily activity and an improvement in the condition of the peristomal skin.
Qualitative feedback such as this consolidates the importance of ensuring that the patient's experience of and confidence in their pouch system is a positive one.
The SCNs were asked to provide feedback following their patient's experience of the use of the Manuka honey flange (via free text on the study questionnaire). A selection of these comments from the SCNs have been tabulated and are shown in Box 1.
Case Study
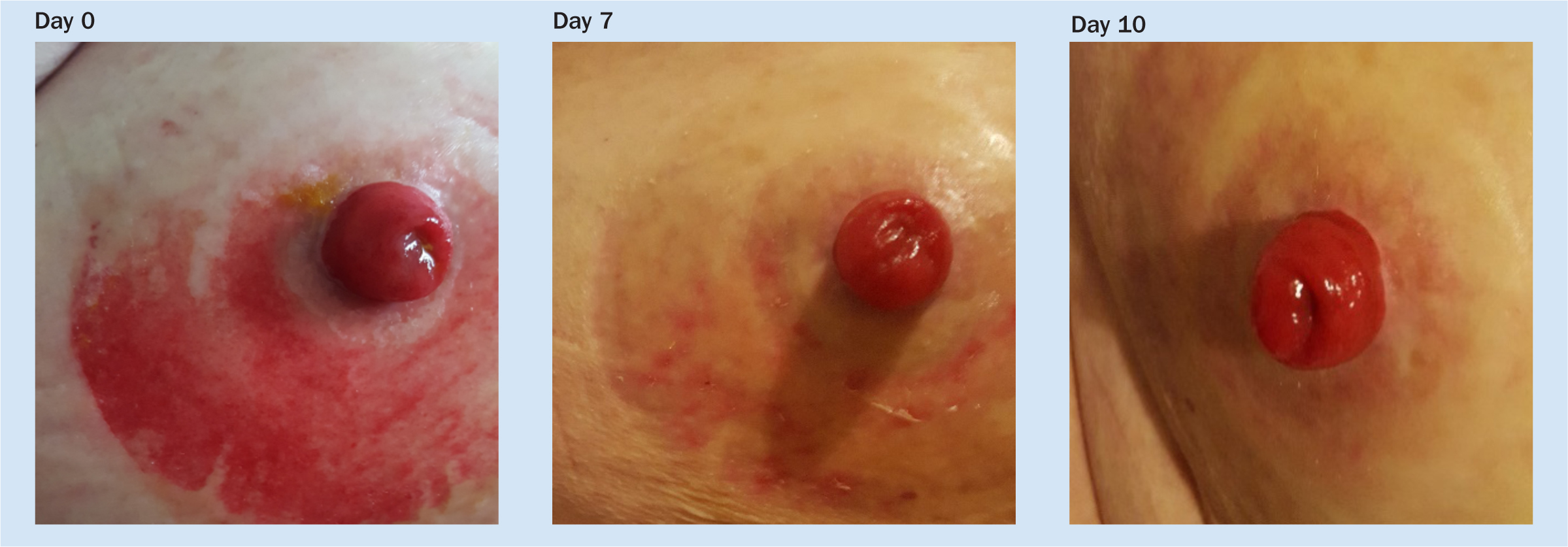
‘Anne’, an 82-year-old lady with dementia, was cared for in her own home by her family, including daily ileostomy care. The family contacted their SCN following the deterioration of the peristomal skin condition.
At initial assessment the SCN observed contact dermatitis caused by a lack of secure flange adhesion to the skin allowing effluent to seep between the flange and the skin. This was causing discomfort resulting in Anne attempting to remove the pouch during the night. This assessment prompted a change of product to a medical-grade Manuka honey flange with the rationale of improving pouch to skin adhesion, supporting skin integrity and ensuring patient comfort.
The family photographed the skin at each pouch change (Figure 8) and gave informed consent for these to be shared. The holistic nursing care and the change to a medical-grade Manuka honey adhesive flange resolved Anne's skin integrity complications.
Conclusion
Peate (2019) stated that:
‘The proverb prevention is better than cure means that it is easier to stop something happening in the first place than to have to repair the damage after it has happened, which is very appropriate in health and social care settings.’
Clinical governance might not be in the forefront of everyone's mind every minute of every day, but it is key to continuous quality improvement, which is important for patient care at all levels. Providers of health and social care services aim to deliver personalised care that is safe, effective, caring, responsive and well-led. Multidisciplinary teams often have to work together, either within or across multiple provider organisations in order to achieve this aim.
All this might seem a little abstract for the day-to-day care of patients, however, specialist nurses working alongside patients with long-term conditions can significantly contribute to addressing the efficiency savings targets required by the NHS. In reducing unwarranted variation in the care delivered and by making clinical decisions relating to products for patients GIRFT has never been more important for both the person with a stoma and the NHS.
Designing and implementing definitive care pathways to manage the challenges presented by people following stoma formation that then can be replicated across an entire stoma care population is challenging due to contextual features of the care settings, geographical localities and localised constraints in which it will be used. Care delivery in the community varies depending on locality with patients seen more or less frequently depending on the assessed clinical need.
In understanding and following up from baseline observations in patients presenting to clinicians with peristomal skin complications, this study shows the importance of re-assessing patients' holistic stoma management in relation to their current peristomal skin condition.
As shown within this study the extent of the problem of peristomal skin complications within their current nursing caseloads was reflected by 43% of the SCNs who reported they had over 60% of patients assessed with peristomal skin complications.
The design of this study enabled detailed patient outcomes to be captured across 26 independent nursing centres, facilitating the review of real-life experiences of patients following the use of a pouching system where the flange contained Manuka honey. The study questionnaire captured the change of treatment pathways implemented by the SCNs as they sought to reduce the level of PSC experienced by their patients.
The change within clinical practice for the study cohort is supported by Kelly O'Flynn's (2016) statement that the assessment and evaluation of the peristomal skin can help nurses decide which is the most appropriate treatment from the wide range of products available.
Results from the independent, multi-centre study supports that through clinical intervention and a reassessment of a patient's stoma, using the most appropriate flange type can improve patient outcomes.
This study brings to the forefront the benefits medical-grade Manuka honey in a flange can provide to both patients and nurses when managing PSC.
Patients and their clinical needs must remain at the very heart of what we do as nurses, a philosophy supported and embedded in the pillars of The Code;
‘Prioritise people, practice effectively, promote safety and promote professionalism and trust.’