

This article summarises a small mixed-methods research project undertaken with trainee nursing associate students (TNAs) during April to June 2021. The project set out to explore the experience of TNAs, their motivation for undertaking the programme, the perception of their role by others and their future career direction. Additional themes were uncovered including the impact of COVID, the efficacy of the TNA programme and professional growth.
Background
The background to the implementation of the nursing associate (na) role that followed on from the mid-Staffordshire NHS Foundation Trust public inquiry (Francis, 2013), the Cavendish Review (Cavendish, 2013) and the Shape of Caring review (Willis, 2015) is well documented (Robertson et al, 2022; Peate 2023). The recommendations from the reports and reviews highlighted the need to bridge the gap between healthcare support workers and registered nurses (RNs). This led to the pilot of the NA role in 2017. The first two waves of the pilot featured 35 NHS trusts (Vanson and Bidey, 2019). Following the initial pilot, the Nursing and Midwifery Council (NMC) approved the NA Standards of Proficiency (NMC, 2024a) and opened the professional register to NAs in January 2019 (NMC, 2023a).
The introduction of the role was initially met with scepticism. For example, it was argued that the numbers of NAs put forward for the pilot were so small that it was hard to see what meaningful impact they could have on the quality of care and patient outcomes (Hayton, 2016; Kessler et al, 2020a). In addition, Launder (2019) pointed out that there were many concerns about the use of NAs, one being the substitution of the RN role. She also pointed out that there seems to be a limited understanding in some quarters as to the remit of the NA role.
However, since the inception of the NA role, the numbers on the NMC register have steadily grown. In September 2023, that number stood at 10505 (NMC, 2023b). In addition, the number of institutions offering NA programmes has also grown. A search of the list of NMC-approved providers (https://www.nmc.org.uk/education/approved-programmes) in May 2024 showed that in England, 110 institutions offered an NA programme. Currently, Northern Ireland, Scotland, and Wales are not offering NA programmes. This is, in part, due to the NMC edict that only English providers could gain approval for delivery in the initial rollout (NMC, 2024b). However, following a request from the Wesh Cabinet Secretary for Health and Social Care the NMC announced in March 2024 that it will ask for approval from the UK government to allow it to regulate the role in Wales as well (NMC, 2024c). This is a significant development as far as the role becoming more widespread, giving increased geographical mobility.
There is clearly a need for the NA role, which has come about as a direct response to failings in health care (Cavendish, 2013; Francis, 2013; Willis, 2015). Primary research into the implementation of the NA role in practice is still in its infancy. Fewings et al (2022) conducted a literature review and identified six research studies; two were by Coghill (2018a, 2018b), three by Kessler et al (2020a; 2020b; 2020c), and a further one was by King et al (2020). The findings from the review by Fewings et al indicated that the TNA programme provided a flexible route into nurse education, as recommended by the Shape of Caring review (Willis, 2015). They also highlighted confusion around the NA role in practice.
The authors identified a further two articles, one by King et al (2023) and one by Robertson et al (2022), that were focused on NAs in the primary care sector. King et al's work highlighted that NA training appeared to focus on secondary care and that, once qualified, NAs faced barriers to progress to RN training. Robertson et al's work focused on workload planning highlighting that, in times of crisis, such as during the COVID-19 pandemic, the line between the roles of student and employee can become blurred. Both again raised the issue of role confusion in practice.
Aims
The overall aims of ths research were as follows:
- To explore the motivation behind undertaking the NA programme
- To examine how TNAs felt that service users and the wider healthcare team perceive the role of the NA
- To explore how TNAs see their career developing post qualification.
Methodology and methods
Mixed methods were used to capture initial data from participants. An online questionnaire was used to generate descriptive statistics and highlight potential areas to be explored in the follow-up focus groups. According to Harnisch et al (2017), at its most basic, a mixed-methods approach draws on a mixture of open-system data collection such as interviews and focus groups and closed-system data collection such as surveys and questionnaires. Using mixed methods allows the use of quantitative and qualitative approaches in one study, enabling the strengths of both methodologies to be combined, with each approach mitigating the limitations of the other (Mikkonen and Kyngäs, 2020). Ethical approval was obtained from The Open University WELS HREC Panel (HREC/3934).
Sample
The total target population comprised 62 TNAs from the southwest region of England. The study set out to recruit the entire population. This is in keeping with purposive sampling when a sample size is small (Campbell et al., 2020). A total of 14 participants completed the online questionnaire, and 6 agreed to take part in the focus groups.
Online questionnaire
The online questionnaire was developed by the researchers and then circulated for peer review by experienced research academics for face and content validity and reliability (Harlacher, 2016). The questions used in the questionnaire are provided in Box 1.
Box 1.Questionnaire questions
- What is the name of the company/organisation/trust that you were working for as a healthcare assistant (HCA)?
- What does the company/organisation/trust you were working for as an HCA do?
- How long were you an HCA before applying for the role of TNA?
- How long have you worked as a TNA?
- How different is your current role as a TNA from your previous role as an HCA?
- To what extent do you agree or disagree with this statement: ‘I am using what I learned during my studies on the NA programme in my current role’?
- Does the team you work with understand the role of an NA?
- To what extent do you agree or disagree with the following statement: ‘My current work fits with my future plans’?
- To what extent are you considering doing the BSc (Hons) Nursing Programme?
Focus groups
Two focus groups were conducted online using Zoom conferencing software. The overarching questions and prompts were developed from the online questionnaire results and the literature review. Each focus group had three participants (6 in total) and was led by a researcher who had no prior relationships with the participants to avoid any unconscious/unintentional bias or risk of coercion (Parahoo, 2014).
The focus groups were transcribed, and the transcripts then analysed using NVivo12. A general inductive approach was used to analyse the raw data from the focus groups. In keeping with this approach, the three research aims were used to provide a focus and the data analysis was carried out without ‘a priori knowledge’, to allow for unexpected and wider themes to emerge (Thomas, 2006). The transcripts were thoroughly read and re-read, then coded, with the initial codes subsequently merged to generate key themes.
Results: questionnaire
The TNAs in this study were on a 2-year apprenticeship programme. The data revealed that they came from a range of practice areas including mental health services, palliative care, acute care, rehabilitation, elderly care, GP practices and community care. Five participants had been working as a healthcare assistant (HCA) for 1–5 years before commencing the NA programme and the same number for more than 5 years. Only one participant had worked in their HCA role for less than 6 months before joining the programme. These results are not surprising as most of the healthcare providers do not recruit externally to the programme but send internal candidates.
Concerning the length of time they had been on the programme, eight participants were in their first year of the programme, two were at the midpoint and four were about to complete the programme. When asked if the TNA role was different from their HCA role, three thought it was vastly different, whereas six thought it was somewhat different, and five felt that the role was just the same (Figure 1a). However, the participants who thought it was just the same were in the first 6 months of the programme. Those who thought that the role was somewhat or very different came from both community and acute care settings with equal representation from both.
In their responses as to how well the wider team understood the role of the NA, one participant indicated the team did not understand the role, and eight said the wider team only understood a little about the role, together representing over half of the participants (Figure 1b). In the question about the use of new knowledge and skills acquired, two strongly disagreed but seven strongly agreed that they did (Figure 1c).
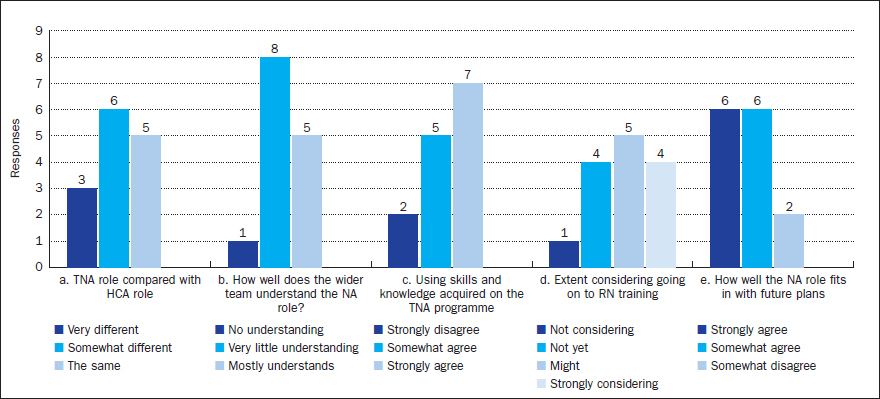
When asked about their future career plans and specifically about undertaking a degree programme to become a registered nurse, four participants were strongly considering this as a progression route, and one discounted this option. The remaining participants responded as ‘unsure’ or ‘not yet’ (Figure 1d). However, six participants ‘strongly’ agreed and a further six ‘somewhat’ agreed that the NA role fitted into their future work plans (Figure 1e).
The findings of the questionnaire were used to generate the ‘grand tour’ questions and sub-questions for the focus groups, shown in Box 2.
Box 2.Focus group questions and prompts
- Why did you decide to complete the NA apprenticeship?
- What has surprised you most about your apprenticeship?
- – Prompt: What has been the most significant thing that has happened to you during your apprenticeship?
- We noticed looking at the survey that many NAs feel work colleagues don't understand their role. How do you feel colleagues, other members of staff, and patients see you?
- – Prompt: Is this different from what you thought your role and contribution would be? Has your role and contribution changed over time? What do your work colleagues need to understand about your role?
- What are your future aspirations as an NA?
- – Prompt: Where do you see yourself in five years' time? Do you hope to do any more study for work?
- How has COVID affected your role as an NA?
- – Prompt: Has COVID changed the job you do? Has COVID changed your career plans or hopes to do further study?
- Are there any further thoughts or information that you would like to share with us?
Results: focus group
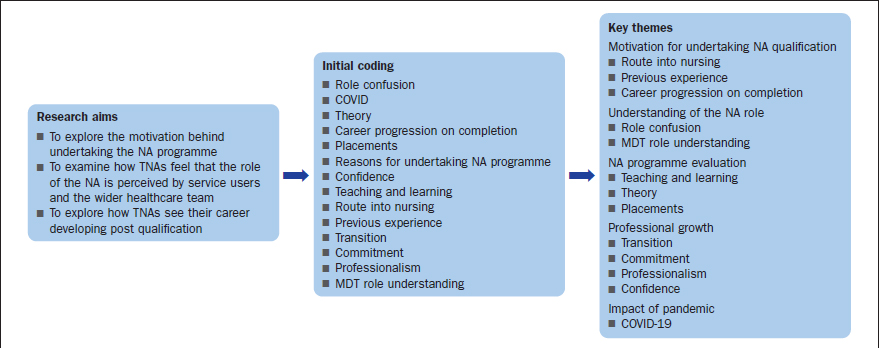
The initial coding produced 14 codes. During the coding process, some quotes were coded to several different initial codes to give a richer understanding of the cross over between the individual initial codes. The initial codes were then merged into five key themes: understanding of the NA role, motivation for undertaking NA qualification, NA programme evaluation, professional growth, and the impact of the pandemic. Figure 2 provides an overview of the coding process.
Theme 1: motivation for undertaking NA qualification
The reasons given were varied including wanting to be able to contribute more to the care and management of the patients. One participant felt they were ‘stuck’ and needed to undertake further development to expand their role. One candidate identified that they saw this as their route into nursing. Some participants felt that they were already doing the NA role and therefore wanted to complete the programme for a salary increase.
When asked whether they saw this as a route to becoming an RN, the views were mixed. Some of the participants identified that they saw the NA role as a professional role in its own right. They commented that they wanted to develop their career as an NA by undertaking further practice development once qualified. Some participants felt that NAs should be involved in the education and training of NAs in the practice education team. Others considered RN training but first wanted to consolidate their learning in the NA role.
‘I was just at a stage where I was stuck, was thinking I can do more, I know I've got more to offer.’
‘I always wanted to go on and do the nursing degree. I still do.’
‘Maybe look at part of the practice educating side with nursing associates. I don't think further study or going on to do a full nursing degree, not for me at the moment.’
Theme 2: Understanding of the NA role
Nearly all participants spoke about the lack of understanding of the NA role. The participants commented that this sometimes led to conflict within the team, especially involving assistant practitioners (APs). Staff in AP roles carry out a similar role to NAs. They normally have completed a foundation degree in health care. However, the foundation degree does not have the same practice requirements as the NA and does not lead to a recordable qualification with the NMC. When the trainee NAs were trying to achieve clinical competencies, they were asked by APs and HCAs to contribute to washing patients or cleaning. Participants agreed that patient care was paramount, but felt they were taken away from learning opportunities. Some commented that they felt like another pair of hands, and they were there to do the ‘messy’ jobs.
Several RNs made comparisons with the phased-out state enrolled nurse (SEN) role, which seemed to make the role of the NA seem more acceptable. Many participants had to advocate for themselves, repeatedly explaining the remit of their role. This was further complicated, as the activities NAs were allowed to do varied between trusts.
‘It was difficult, and I found myself sort of advocating for myself because there were assistant practitioners … at the same band but with a different role, who would get a bit cross … that I could do the medication and I could do this, and I could do that, and I've found it varies very, very much as well from trust to trust …’
Theme 3: NA programme evaluation
All participants gave examples of where they were able to put theory, even theory that they considered irrelevant such as sociology at the time, into practice. They spoke very enthusiastically about the practice placements and the variety of practice placements they undertook on the programme. One participant spoke about the ‘lightbulb moment’ when things fell into place. They also felt that they could take new skills back into their home base. The participants liked the way that the programme built up their skills step by step, with one commenting that they were repeatedly shocked at how well they had done in assignments.
‘I agree with the way that it builds you up and things and I have repeatedly shocked myself at how well I've done and, you know, I'm like, what, is that my score? … for me, the most standout is the lightbulb moments that you get from the learning when you're in practice and you think, ah yeah, that makes sense now, and when it just clicks and, oh, it's a brilliant feeling, it's great.’
Theme 4: professional growth
Participants spoke extensively about the confidence and assertiveness they have gained. This was especially regarding new skills, being able to challenge outdated practice with evidence and to advocate for themselves and others. A common theme was that they felt confident to explore working in different fields rather than just one field of practice, and were open to working in many different areas. The following comments are representative:
‘It's important to speak out … If you see something wrong you need to – it's part of the NMC Code – you need to advocate and you need to stand up to that person or that situation.’
‘It was, if you didn't step up and say something, you would just be marginalised.’
‘It gives you that experience in all four sectors, so I've had no previous mental health experience, no real learning disability experience, I've got a paediatric placement coming up in September, so the beauty of it is you get to experience all these different sectors.’
Theme 5: experiences and effects of COVID
Many of the students were in practice during the COVID-19 pandemic. The main commentary related to the disruption of placements. One participant commented that their employer did not want to release them into external placements because they were worried the student would contract COVID-19 and bring that back to the community setting. Another participant had a complete placement cancelled. A few participants spoke of the fear and pressure generated by COVID-19 as they and their families were concerned about contracting it. One participant talked about an experience where the husband contracted COVID-19 and the stress of trying to cope with caring for him while studying.
‘Because I work in the surgery, they wouldn't let me go out into a different environment because of the spread of infection … my husband got COVID. The stress at one point it really got on top of me … the pressures of doing the assignments … my husband being poorly, not being at work so you're not getting any money.’
Discussion
Some, but not all participants, viewed the NA role as a route to becoming an RN. Other participants wanted to see the NA established as a distinct career pathway rather than as a stepping stone to the RN. Although this is in keeping with views expressed by Hodge (2018), it is in contrast to the work of Fewings et al (2022). Some felt the NA qualification gave them the legitimacy to practice in niche roles in areas such as lymphoedema treatment. Other roles suggested included education of NAs by NAs rather than RNs in the classroom and practice areas and roles in leadership and management.
Some of the participants commented on the SEN role, stating that other members in the team found this was the easiest way to understand the NA role. SEN training was phased out in the UK in the 1990s. Allan and McLafferty (1999) undertook a literature review of the career aspirations of SENs including their desire to convert to RN status. Their findings are similar to those in this study. Although some saw conversion to RN status as a career progression, many SENs did not want to convert. The reasons for non-conversion included reluctance to do further study, family commitments, age and liking the role they were in. Indeed, many SENs went on to do specialist roles and continued with professional development including higher degrees. Those SENs who did want to convert cited that they were doing the RN job already along with fears about the SEN role being phased out and job security.
What was evident from this study was the lack of clarity about the scope of practice of the NAs as this varied from trust to trust. With England reintroducing second-level registrants, there is a need to carefully reflect on how the NA role is developed within the workforce.
Further research is needed to capture how professional identities in new health and social care professional groups become established. In addition, it should include how best to use the NA role in the workforce in relation to workforce planning. This may require looking at other countries who have successfully embedded and successfully maintained a multitiered registrant nursing workforce strategy, such as Australia and Canada (Mildon, 2013; Endacott et al, 2018).
An additional factor that cannot be overlooked is the COVID-19 pandemic. This certainly played a role in shaping the practice experience, with placements not being available and the limitation of available experiences. This concurs with the work of King et al (2022), suggesting that the impact of COVID on healthcare education requires further exploration.
Limitations
There were several limitations to this study. The study had a small sample size and was geographically constrained to the southwest region of England. The sample was also predominately female. This research identified that NA students are keen to develop their own unique professional identities.
Conclusion
This research has provided insight into the role of the NA, including the reasons for undertaking an NA programme and future career trajectories. It has also explored the understanding of the NA role, including role confusion and conflict. The participants in this study expressed that developing the knowledge to underpin clinical proficiencies and using evidence-based practice has increased their confidence in practice. Although some participants considered their career progression to be undertaking pre-registration nurse training, some also saw the NA role as a new discreet profession. There was variation between employers as to which tasks can be undertaken by the NA and what is within their scope of practice. Therefore the deployment of the NA role within the workforce remains, at present, unclear.
KEY POINTS
- The number of nursing associates (NAs) in practice is steadily growing
- There remains confusion over the NA role
- Some NAs see the role as a distinct role and not as a stepping stone on to the registered nurse programme
- Some NAs want to progress into education and leadership roles, as well as specialising in a specific area
CPD reflective questions
- Going forward, how will nursing associates (NAs) influence care delivery?
- How will NAs develop their own professional identity?
- What are the possibilities of specialist NA roles?
- Is there scope for registered associate roles in the other health and care professions?