

Urinary catheterisation is a critical procedure in health care for patients unable to naturally empty their bladders. It is essential that health professionals understand the anatomical and procedural differences between male and female catheterisation in order to ensure safe and effective care. This guide provides an updated overview of the urinary system's anatomy and detailed procedural steps for catheterisation in both men and women, supported by current best practices and recent research.
Anatomy of the urinary system
Male and female anatomy
A comprehensive understanding of the anatomy and physiology of the genitourinary tract in both genders is essential for effective catheterisation. This knowledge is crucial for health professionals, particularly nurses, to deliver holistic care and effectively communicate the procedure to patients. Understanding these anatomical differences also aids in anticipating potential complications and selecting the appropriate catheter size and type for each patient.
The urinary system
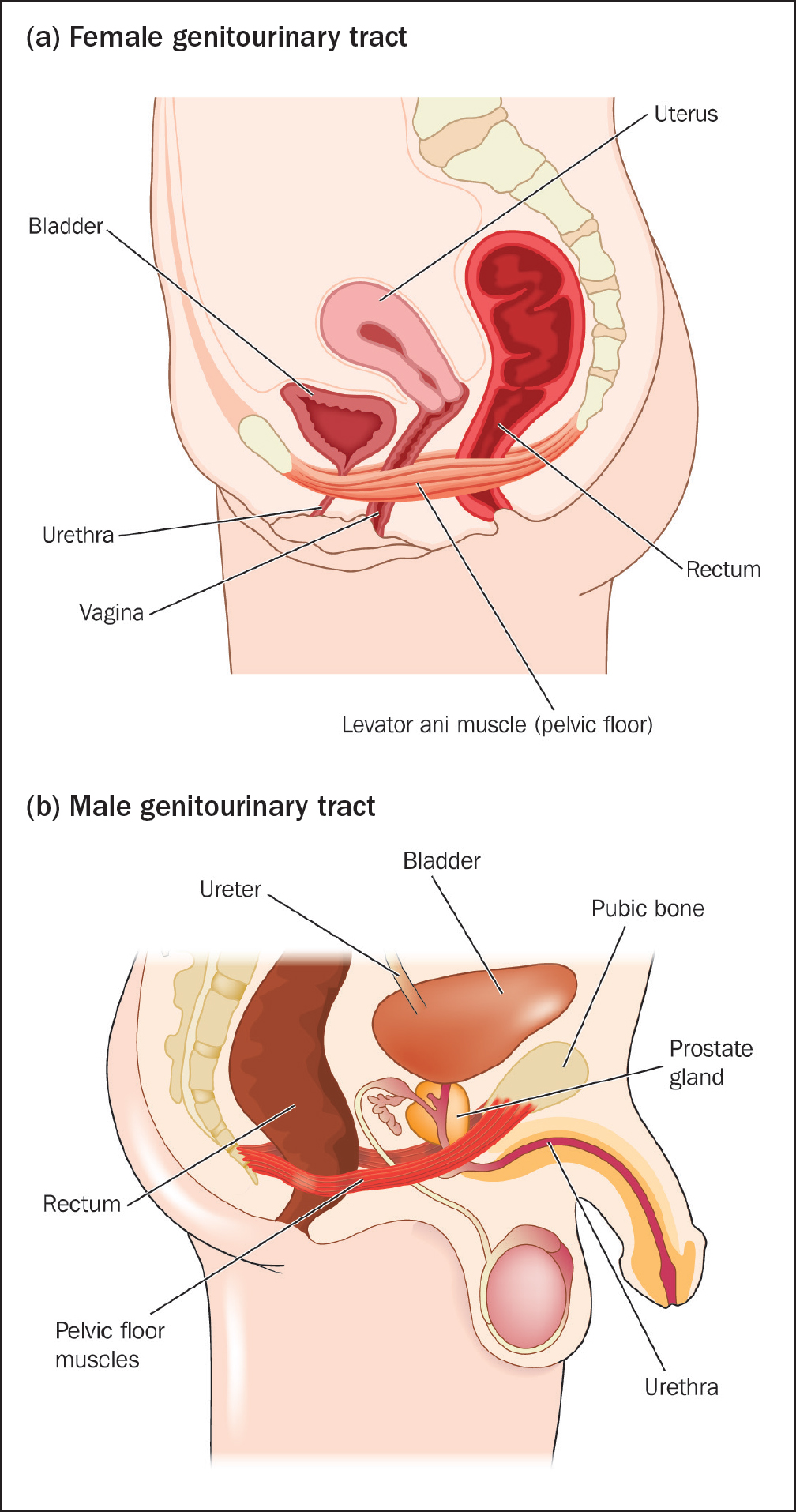
The urinary system, also known as the renal system, is responsible for the production, storage, and elimination of urine. It consists of the kidneys, ureters, bladder, and urethra (see Figure 1).
Understanding the physiological processes of the urinary system, such as the filtration of blood by the kidneys and the storage capacity of the bladder, is equally important. This knowledge helps in assessing the patient's urinary function and identifying any abnormalities that may affect catheterisation.
Key anatomical differences in catheterisation
Female anatomy
Male anatomy
Importance of anatomical knowledge
This anatomical knowledge is vital for several reasons:
By integrating this detailed anatomical understanding into practice, health professionals can enhance patient outcomes, improve procedural success rates, and ensure a higher standard of care during urinary catheterisation.
Preparing for catheterisation
Nursing considerations
Nurses must operate within their competence limits, adhering to the Nursing and Midwifery Council (NMC) Code (NMC, 2018). Before catheterisation, it is essential to communicate with the patient, provide relevant information, and ensure the patient's understanding to obtain informed consent. Respecting the patient's privacy, cultural beliefs, and personal preferences is crucial. Box 1 illustrates the possible physical problems associated with catheterisation and Box 2 illustrates some key nursing considerations, in the form of the equipment that should be prepared for the procedure.
Possible physical problems
Equipment required for catheterisation
Step-by-step procedure for male catheterisation
Documentation
Step-by-step procedure for female catheterisation
Advanced considerations and complications
Catheter valves
Catheter valves are devices attached to the end of an indwelling urinary catheter that allow for controlled, intermittent drainage of urine. They support natural bladder filling and emptying cycles, which helps maintain bladder muscle tone and capacity, reducing the risk of bladder muscle atrophy. By promoting intermittent drainage, they also reduce the risk of urinary tract infections (Holroyd, 2021; Spoolder and Geelhoed, 2023). Catheter valves increase patient mobility and comfort, because they are more discreet and allow for greater freedom of movement compared with continuous drainage bags. This promotes a sense of independence and improves the quality of life for patients requiring long-term catheterisation. An overview of some of the positives and negative aspects of catheter valves is outlined in Table 1.
| Aspect | Positives | Negatives |
|---|---|---|
| Infection control | Reduces the risk of urinary tract infections by allowing the bladder to fill and empty naturally | Improper use or poor hygiene can still lead to infections |
| Bladder function | Encourages normal bladder function and reduces the risk of bladder muscle atrophy | May not be suitable for all patients, particularly those with poor bladder control or cognitive impairments |
| Mobility | Increases patient mobility and comfort compared to continuous drainage | Requires more frequent emptying, which can be inconvenient for some patients |
| Convenience | Reduces the need for continuous drainage bags, which can be bulky and conspicuous | Patients need to remember to open and close the valve, which might be challenging for some individuals |
| Cost | Potentially lower costs over time due to reduced use of drainage bags and related supplies | Initial cost of valve may be higher than traditional catheters |
| Patient independence | Promotes independence and quality of life by reducing the stigma associated with visible urine bags | Requires patient education and compliance, which might not be feasible with all patients |
Securement of catheters, tubing, and bags
The securement of catheters, tubing, and bags is crucial in preventing complications such as meatal tears in men. Various securement methods, including sleeves and straps, have been developed to enhance patient comfort and safety.
Securement devices
In a randomised controlled trial to assess the effectiveness of catheter securement, Calpe-Damians et al (2024) reported that proper securement of catheters can significantly reduce catheter-associated urinary tract infections (CAUTIs), the incidence of meatal tears and other catheter-associated complications.
Catheter passport
The‘catheter passport’ is a patient-held document that provides detailed information about their catheterisation. This includes the type of catheter used, the date of insertion, and any specific care instructions. The passport aims to improve communication between healthcare providers and patients, ensuring consistent and accurate care. The implementation of a catheter passport significantly reduced catheter-related complications and has been shown to improve patient satisfaction (Prieto et al, 2020).
Potential complications
Understanding potential complications is critical for effective catheterisation management. Complications can include CAUTIs, urethral damage, and patient discomfort (Centers for Disease Control and Prevention (CDC), 2024). It is essential to adhere to aseptic techniques and follow guidelines strictly to minimise these risks.
Strategies to minimise complications
Conclusion
Urinary catheterisation is a crucial healthcare procedure requiring a thorough understanding of male and female anatomy, strict adherence to aseptic techniques, and proper equipment preparation. By following evidence-based practices and ensuring patient safety through careful communication and technique,healthcare providers can minimise complications and improve patient outcomes.