
Adolescence is a significant development period and the time adolescents take to reach major developmental milestones varies (Arnett, 2013). Adolescents with long-term health conditions (asthma, diabetes, cystic fibrosis) are of particular interest because of the burdens and limitations associated with their illness (Suris et al, 2004; Michaud et al, 2004; Al-Yateem, 2013; Maslow et al, 2013). Support for adolescents with long-term conditions may reduce the impact of their illness on their lives, meaning their developmental progression could match that of their healthy counterparts (Suris et al, 2004; Michaud et al, 2004; Al-Yateem, 2013; Maslow et al, 2013; Yoo, 2019). However, without appropriate support, these adolescents may be at risk for developing psychological comorbidities and adopting inefficient/maladaptive coping mechanisms (Grootenhuis et al, 2006; Stam et al, 2006; Al-Yateem et al, 2016a).
Many mental health disorders begin before age 14 years. Adolescents with comorbidities have an increased risk for these disorders (World Health Organization (WHO), 2019a), especially those with severe illnesses (Kraaij and Garnefski, 2012; Zirke et al, 2013), and females are more affected than males (Kraaij and Garnefski, 2012). Cultural context (Mihalca et al, 2017) and types of coping strategies (Compas et al, 2012; Stanescu and Romer, 2013) also affect adolescents' coping.
Adolescents use various coping strategies to control the effects of their health condition on their lives (Gil et al, 1997; Schmidt et al, 2003). These strategies influence adolescents' adaptation to their illnesses and the risk of comorbidities, especially psychosocial problems (Barton et al, 2003; Compas et al, 2012). Coping strategies include control-based or primary coping (acting on another's/one's own emotions), secondary control or accommodative coping (adapting to sources of stress) and disengagement or passive coping (avoiding/denying stressors). Secondary control coping may be useful for adolescents with long-term health conditions because disengagement is associated with poor adjustment, and primary control coping may be difficult to achieve (Barton et al, 2003; Compas et al, 2012).
The ability to cope and the type of coping depends on individual, environmental and contextual factors. If individuals cannot manage or make sense of life with their illness, the potential consequences (eg complications, further treatments) may lead to a perceived poor quality of life (Van De Ven et al, 2007; Nogueira et al, 2009; Tiggelman et al, 2014; Oppenheimer et al, 2018; Yoo, 2019). For example, children with type 1 diabetes who used problem-solving coping strategies reported better quality of life than those who used emotion-focused strategies (Jović et al, 2009). Positive spiritual coping (ie using one's relationship with self, ultimate other/God or nature to cope) promotes optimistic attributions for the causes and progression of illness and suffering (Baldacchino and Draper, 2001; Reynolds et al, 2013; 2014).
Various interventions have been found to improve coping strategies, including teaching skills to manage illness (Nogueira et al, 2009; McNamara et al, 2010), improving adolescents' sense of coherence (Tiggelman et al, 2014), cognitive behavioural therapy (Kashikar-Zuck et al, 2013; Douma et al, 2018) and mindfulness-based interventions (Abujaradeh et al, 2018). These interventions should be implemented early, as adolescents' coping mechanisms may become less flexible as they grow older (Gil et al, 1997; Schmidt et al, 2003). If unaddressed, maladaptive coping mechanisms may evolve into negative health behaviours (eg smoking, risky sexual behaviours) (Ginsburg and Jablow, 2006; Taylor et al, 2008).
Advances in healthcare mean that more adolescents with long-term health conditions can attend mainstream schools (Al-Yateem et al, 2016b). However, this creates challenges for school-based carers (Al-Yateem et al, 2016b). A United Arab Emirates (UAE) study found that managing students with long-term health conditions and complex healthcare needs was the highest research priority identified by school nurses (Al-Yateem et al, 2016b). Although school health professionals can contribute to the wellbeing of students with long-term health conditions, adequate support and preparation for these health professionals is lacking (Borup, 2007; Walker, 2012; Abu Dhabi Educational Council, 2014; Al-Yateem et al, 2016b; National Association of School Nurses, 2018).
Consistent with global trends, the prevalence of long-term health conditions among UAE adolescents is increasing (WHO, 2019a, 2019b). Adolescents in the UAE also face cultural and environmental risk factors for developing mental health problems, such as consanguineous marriage and large family units (Saadat, 2011; Denic et al, 2013; Dahdouh et al, 2016; Al-Yateem et al, 2017, 2018). Currently, the UAE focuses on tertiary treatment for children and adolescents with long-term health conditions, with little attention directed to preventive/health promotion interventions. It is essential to focus on these areas to facilitate resilience among children and adolescents with long-term health conditions, and support improved health outcomes and system-wide benefits (eg reduced healthcare expenditure). This study is important as it addresses the needs of this vulnerable UAE population.
Study objectives
Adolescents spend most of their time at home and school. It is important to understand how adolescents cope with their illnesses in these two settings. This study investigated the coping strategies used by adolescents with long-term health conditions in challenging situations (eg exacerbation of illness) at school and home, and identified the characteristics of adolescents' preferred care environment.
Study methods
Research design
This study used a concurrent mixed-methods design, with quantitative and qualitative data gathered concurrently between January and May 2018. Quantitative data were collected using an established questionnaire and qualitative data were gathered by asking participants to answer open-ended questions in a written narrative format.
Population, sample and setting
Asthma and diabetes are common long-term health conditions among UAE adolescents (Ahmed, 2010; Khan, 2013). The treatment, lifestyle adjustments, expected complications, acuity/seriousness of complications and coping are challenges associated with these conditions (Suris et al, 2004; Al-Yateem, 2012). This study included adolescents with asthma or diabetes to represent long-term health conditions. Participants were recruited via schools, where many adolescents with long-term health conditions would be present.
The UAE school health service is managed by multiple authorities. For example, the School Health Section in the Ministry of Health and Prevention manages government-run schools across the country. Health authorities in different Emirates also manage some school health services in that Emirate. This made obtaining accurate information or a sampling frame for the study population difficult, which precluded probability sampling. Convenience sampling was therefore used for this study. Secondary schools in different Emirates were approached, and all students with asthma or diabetes in schools that granted access were invited to participate.
The inclusion criteria for this study were:
All accessible private and government schools in the northern region of the UAE were contacted regarding participation. Participating schools were provided with complete information about the study, and schools that granted access were visited for data collection.
This study adhered to parental consent procedures used by participating schools. Eligible students were identified with the help of school nurses, and approached regarding participation. Students were informed about the purpose of the study, completing the questionnaire, treatment of the data and their rights during participation. Students who agreed to participate were informed their participation was conditional on parental consent (UAE law specifies individuals over 18 years can sign a consent form). Parents of interested adolescents were contacted by the school nurse, who provided full information about this study and their child's participation. Parents returned a signed consent form if their child could participate. Next, data were collected in classrooms during students' activity classes. Students for whom parental consent was not obtained completed usual classes.
Questionnaires were distributed to participating students. Completed questionnaires were returned to a research team member who remained in the classroom during data collection to provide clarification, and answer students' questions as required.
Data collection instrument
This study used the short version of the Coping Strategies Inventory (CSI-S). The CSI-S asks participants to think about a stressful illness-related event in the last 3 months, and rate listed coping interventions by the extent to which they used each strategy (from ‘not at all’ to ‘very much’). Participants rated each strategy twice to describe the extent to which they used that strategy at home and at school.
The questionnaire covered coping in four sub-domains: problem-focused engagement (problem solving, cognitive restructuring); emotion-focused engagement (social contact, expressing emotion); problem-focused disengagement (problem avoidance, wishful thinking); and emotion-focused disengagement (social-withdrawal, self-criticism). These sub-domains were clustered under two broad categories: engagement and disengagement.
The questionnaire included open-ended questions prompting participants to reflect on a stressful situation. Most participants preferred home as the care environment, as home had caring agents who: (1) were close and available; (2) knew how to care for them, understood their individual needs and had the resources to provide/access care; and (3) listened and understood them. Three strategies were commonly used when participants experienced illness complications:
The CSI-S has been widely used and has established validity and reliability. The English version of the CSI-S showed good validity (Cronbach's alpha 0.56–0.80) with patients on haemodialysis in the USA, UK, Canada, Australia and New Zealand (Speyer et al, 2016). No Arabic version of the CSI-S is available, therefore, it was translated collaboratively by a professional translator and a bilingual research team member. These translators worked individually and then as a team to reach agreement on the translated CSI-S. Back-translation into English was performed by another bilingual healthcare professional to ensure there were no major discrepancies. The clarity and readability of the translated questionnaire was assessed by school nurses. In this study, the questionnaire had Cronbach's alpha values of 0.72 (home) and 0.79 (school).
The questionnaire was supplemented with information on participants' gender, age, illness, Emirate and school type. These data were recorded by the research team member with the help of the school nurse.
Data analysis
Counts and percentages were used to describe participants' demographics. As the data were not normally distributed, a non-parametric Wilcoxon signed-rank test was used to investigate statistically significant differences between coping strategies used by adolescents at school and home. A Mann–Whitney U test was used to compare coping strategies by sample sub-groups (ie gender, school type, disease type, age group). Participants' answers to the open-ended questions were analysed using content analysis. This interpretive process explored participants' narratives to identify themes and reach an in-depth understanding (Schreier, 2012).
Ethical considerations
The University of Sharjah Research Ethics Committee approved this study. The research team adhered to principles of participant anonymity. No identifying data (eg names, contact details) were obtained. Completed questionnaires were only accessible to the research team. Participants were informed about their right to withdraw without affecting their study or care at school. However, once questionnaires were given to the research team, participants were unable to withdraw as their questionnaire was not identifiable. Students' assent and parental consent were obtained before data collection.
Results
Survey results
Table 1 shows participants' demographic characteristics. Participants were from five Emirates: Dubai (21.9%, n=90), Sharjah (19.7%, n=81), Ajman (22.6%, n=93), Ras Alkhaima (17.5%, n=72) and Fujairah (18.2%, n=75). Most participants attended government schools (88.3%, n=363), 47.4% were aged 12–15 years and 48.9% were boys. In total, 62% (n=255) of participants had asthma and 38% (n=156) had diabetes.
| n | Percentage | ||
|---|---|---|---|
| Emirate of residency | Dubai | 90 | 21.9 |
| Sharjah | 81 | 19.7 | |
| Ajman | 93 | 22.6 | |
| Ras Alkhaima | 72 | 17.5 | |
| Fujairah | 75 | 18.2 | |
| Age, years | 12–14 | 198 | 48.2 |
| 15–18 | 213 | 51.8 | |
| Gender | Male | 201 | 48.9 |
| Female | 210 | 51.1 | |
| School | Government | 363 | 88.3 |
| Private | 48 | 11.7 | |
| Health condition | Asthma | 255 | 62.0 |
| Diabetes | 156 | 38.0 |
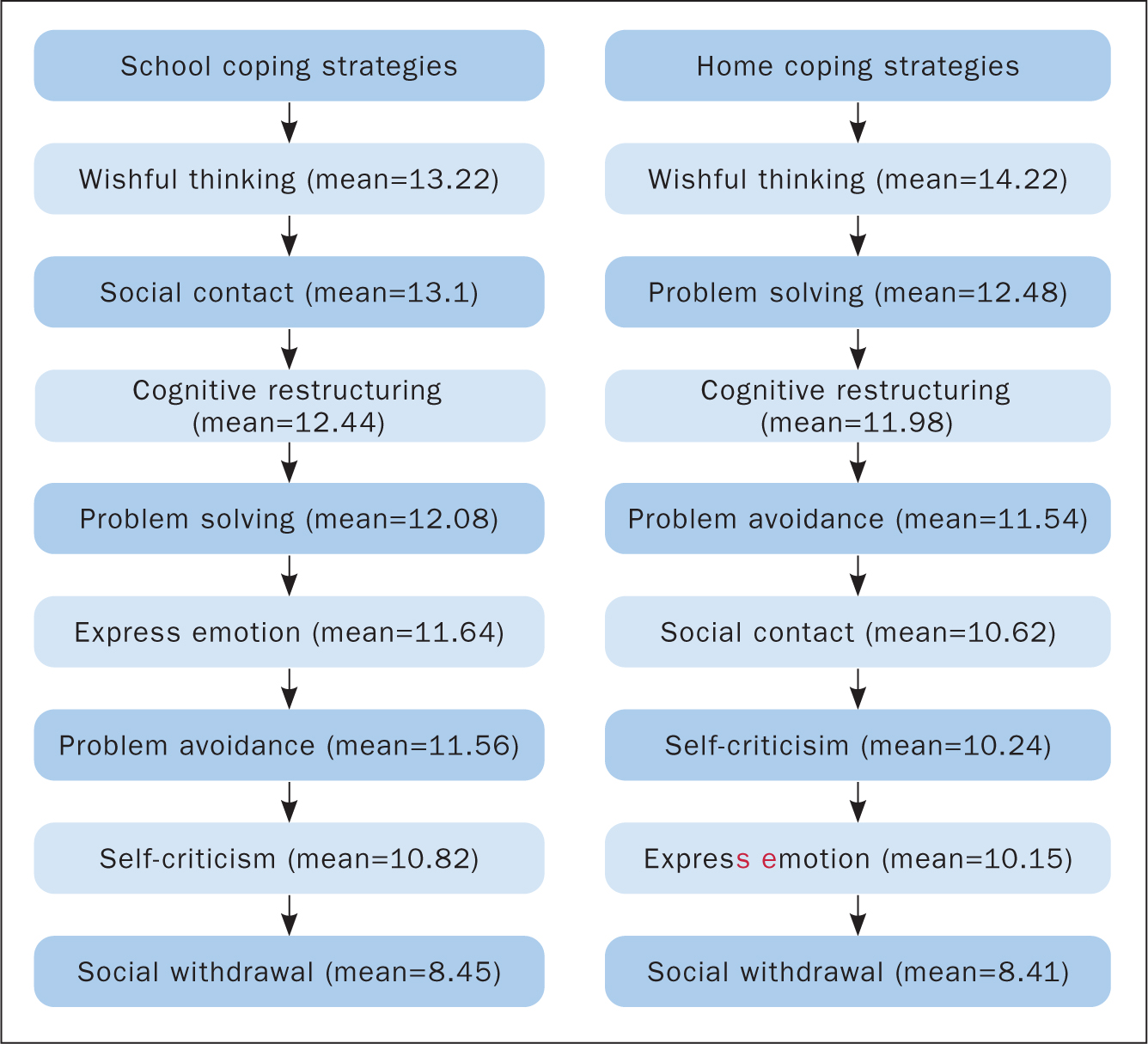
Figure 1 shows the coping strategy dimensions. ‘Problem-focused disengagement’ was used most often at school (mean ± standard deviation (SD) 24.83±5.35, median 25.00) and home (25.75±5.76, median 27.00), followed by engagement strategies (problem solving or adapting emotions). Problem solving was slightly more often used at home (24.54±5.73, median 26.00) than school (24.6±7.59, median 24.00). At school, participants focused on adapting their emotions before solving the perceived problem. ‘Emotion-focused disengagement’ was the least-used strategy in both settings (school: 19.31±4.66, median 19.00; home: 18.53±5.69, median 19.00).

‘Wishful thinking’ was commonly used in both settings (school: 13.22±3.54, median 13.00; home: 14.22±3.67, median 15.00). However, participants sought social contact from peers/their environment at school (13.1±3.63, median 13.00) and family support to solve problems at home (12.48±3.54, median 13.00). Cognitive restructuring was the third most common strategy used at both school and home (school: 12.44±5.91, median 12.00; home: 11.98±3.19, median 12.00). The least-used coping strategy was social withdrawal (school: 8.45±3.04, median 8.00; home: 8.41±3.08, median 8.00).
There were statistically significant differences between home and school for: ‘express emotions’ (P<0.001), ‘social contact’ (P<0.001), ‘self-criticism’ (P=0.004) and ‘wishful thinking’ (P=0.004). Participants used these strategies more often in school than at home, although ‘wishful thinking’ was used at home more than at school (Table 2, Figure 2). Girls used emotional disengagement (mean scores: girls, 20.14; boys, 18.41) and self-criticism (girls, 11.37; boys, 10.25) significantly more often than boys.
| School Mean (SD, median) | Home Mean (SD, median) | P value (Wilcoxon signed-rank test) | |
|---|---|---|---|
| Problem solving | 12.08 (3.87, 12.50) | 12.48 (3.54, 13.00) | 0.573 |
| Cognitive restructuring | 12.44 (5.91, 12.00) | 11.98 (3.19, 12.00) | 0.838 |
| Express emotion | 11.64 (3.06, 11.00) | 10.15 (2.63, 10.00) | <0.001 |
| Social contact | 13.10 (3.63, 13.00) | 10.62 (3.12, 11.00) | <0.001 |
| Problem avoidance | 11.56 (2.95, 12.00) | 11.54 (2.96, 12.00) | 0.691 |
| Wishful thinking | 13.22 (3.54, 13.00) | 14.22 (3.67, 15.00) | 0.004 |
| Self-criticism | 10.82 (3.09, 11.00) | 10.24 (4.29, 10.00) | 0.004 |
| Social withdrawal | 8.45 (3.04, 8.00) | 8.41 (3.08, 8.00) | 0.729 |
SD=standard deviation
Qualitative findings
Some questionnaires were excluded from the qualitative analysis as participants did not complete the open-ended questions, did not elaborate adequately or their writing could not be understood. This was an expected limitation of a written narrative methodology. Forty-two responses that contained adequate elaboration for these questions were included in the qualitative content analysis. This was an acceptable sample size according to qualitative traditions, and allowed a good understanding of students' experiences.
Most participants preferred home as the care environment, as home had caring agents who: (1) were close and available; (2) knew how to care for them, understood their individual needs and had the resources to provide/access care; and (3) listened and understood them. Three strategies were commonly used when participants experienced illness complications: (1) complete reliance on family support; (2) ignoring the problem; and (3) living with the problem.
Care environment
Theme 1: Caring agents who are close and available
This reflected the importance of having caring agents who were close and available when adolescents needed help. These two factors determined the safety of the environment from participants' perspectives. Home was perceived as better able to cater for acute care needs than school.
‘I prefer to be cared for at home because I am close to my family; my family … especially my mother … is always available and helps me. At home I always find somebody around me to help.’
Some participants perceived accessibility to the school nursing service was limited when they became unwell.
‘… I like at home because the nurse or doctor are not always available to help or sometimes busy…’
‘… at school the teacher does not always see me, and sometimes leaves me …’
Participants were afraid of experiencing illness-related issues at school because of this limited healthcare support.
‘One day I felt tired and sleepy in class … I was not able to speak, the students noticed and looked for the teacher and nurses to help me. When they arrived, as my friends told me later, I was not able to speak and they took me to the hospital … I feel scared since then…this might happen again …’
Theme 2: Caring agents who ‘know how, know me and have the resources’
Participants emphasised that carers should know them and their condition, illness history, needs and preferences, and also have the required knowledge and resources to support their interventions. Participants identified these factors as essential to receiving the care they needed and wanted. However, school-based carers were perceived as lacking the ‘know me’, the ‘know how’ or the resources to provide required care.
‘Home is better to solve my problems, because my family understand me…in school the nurse/doctor does not understand me and I don't understand him/her, and they don't know what I want or my problem needs…’
‘At home if I have a problem, it will be OK … my family knows me, they know my medicine … my mum knows everything, and she follows-up all my problems … in school, it is scary because they don't know me well, and they don't have my medicines.’
When these attributes were present in schools, participants spoke positively about their school carers' knowledge of their conditions and sensitivity to their needs. Some suggested that school had the potential to be a good caring environment and an important resource when they faced problems.
‘There is no difference, the nurse is very good here, I like her … she knows me and everything about my problem. I come and talk to her when I have problem.’
Theme 3: Caring agents who listen and understand
Participants suggested that they needed carers who: cared about adolescent health, development and wider psychosocial needs; listened to their needs, requests and complaints; and understood their issues. Most participants favoured home because their carers listened and understood their needs and concerns, and provided care even without them requesting help. In contrast, participants reported school-based carers were not concerned about them unless they asked for help or were called by others for a healthcare issue. Some participants reported that, at school, they were sometimes asked to do things that negatively affected their health condition, stressed them physically/emotionally or embarrassed them in front of peers.
‘Sometimes in the physical exercises classes we were forced to do some exercises, they did not understand that our health condition could get worse as a result … I could not finish the exercises like my friends; this was so embarrassing, I was so slow also because I was tired. I was so frustrated that day.’
In contrast, care at home was generally provided promptly without asking.
‘I came back from my friend house, it was birthday party. I was tired and went straight to my room, my mum noticed … she checked on me and then helped me get better … next day she checked me again and I still was not feeling normal, so she took me to the hospital.’
‘I prefer home because my family is so patient with me, they listen to me all the time.’
When school-based carers met these criteria, it made a difference for participants, and they liked being at school.
‘I like Ms X (the nurse), she always checks on me, she listen to me when I go to her in classes with problems. One day I spoke to her; she listened and she hugged me; that was so nice.’
Home was not the best care environment for all participants. When there were challenges to family functioning (eg marriage conflict, unhelpful parenting styles), participants preferred to be in school.
‘Sometimes when my parents are arguing, I feel tired, also sometimes they are angry from me and shout at me. I also get tired, in school I feel better away from all of this.’
Coping strategies
Three prominent coping strategies were used in both settings: living normally, accepting the illness and seeking external assistance. Living normally was frequently used in school. Participants did not want to look, act or be perceived as different from their peers.
‘I don't like to have health problems at school. I like to live normal and I ignore my health problems here … if I feel something I will try to push it until I go back home.’
Another participant described resisting looking sick in front of peers until they broke down.
‘… there was a part in school that day, and I was OK, then I started to shiver…and feel tired. I sat on my table at class, and students were talking to me and I could not respond, they called the teacher and the nurses afterward … I woke up in the hospital.’
Some participants reported being bothered when they were asked to do things that made them different from or unequal to their peers.
‘Sometimes, when they ask me to do things … not considering my health problem … especially in the PE [physical education] class. I always push myself too hard to do it, and sometimes I was the last to finish … I will be very tired afterward, and that ruins my day.’
Living normally was also supported by religious beliefs; some participants cited the need to live normally with their illness and accept it as it being from ‘God’ because they would be ‘rewarded’ for accepting their illness.
When school health professionals actively provided education about the importance of peer support, the outcomes appeared to be positive. Adolescents with health issues were less sensitive about their peers' involvement in their illness, had more control of their illness (eg not delaying taking medications, avoiding potentially harmful actions) and other students were responsive and prepared for potential health issues. One participant noted that students in her class were considerate, which made her life easy. She attributed this to the school health professionals and teachers who had created this positive environment.
Seeking help/assistance and relying on family members and others nearby was another commonly used coping mechanism. Participants reported they actively asked for help or received help automatically from their family for illness complications. Many sought help from school health professionals when they perceived these professionals as helpful and capable.
Discussion
This study supported a comprehensive understanding of the coping strategies used by adolescents with long-term health conditions at school and home. The quantitative component revealed the coping strategies most frequently used by participants. The qualitative component allowed a deeper understanding of participants' preferred care environment for illness-related issues and their rationale for selecting these coping strategies.
Data integration: comparing the quantitative and qualitative results
Both study phases showed that adolescents initially implemented negative coping strategies (eg living normally, avoiding the problem/disengaging), followed by strategies where they engaged at emotional and behavioural levels to adapt to their illness (Table 3).
| Qualitative findings | Quantitative findings | ||
|---|---|---|---|
| Home | School | ||
| Negative coping | Living normally | Problem-focused disengagement | Problem-focused disengagement |
| Positive coping attempted | Accepting the illness | Problem-focused engagement | Problem-focused engagement |
| Seeking external assistance | Emotion-focused engagement | Emotion-focused engagement | |
Adolescents' use of negative coping strategies (eg problem avoiding/disengagement) before moving to positive coping strategies was a major issue, because it could expose them to further complications and risks. However, negative coping strategies may be expected because adolescence is characterised by exploration of risky behaviours (eg smoking, driving at speed). These behaviours are as prevalent among adolescents with long-term health conditions as their peers, despite the potential for adverse health effects (Suris and Parera, 2005; Ginsburg and Jablow, 2006; Taylor et al, 2008). Early intervention may improve adolescents' coping and reduce these risky behaviours (Abujaradeh et al, 2018; Douma et al, 2018; Failo et al, 2018).
This study also highlighted girls' vulnerability to adopting negative coping strategies (eg self-criticism, emotional disengagement), which could expose them to psychological or physical risks. This finding was consistent with another study (Kraaij and Garnefski, 2012) that reported girls were more vulnerable to psychological comorbidities and experienced more depressive symptoms than boys with similar health conditions. An added difficulty in the UAE context is the restrictions placed on females (especially during adolescence), including mobility, social interactions (particularly with males) and employment opportunities. Exposing adolescents to additional stress and anxiety may compound this problem.
Another concern was that the school setting did not provide healthcare services that met adolescents' needs and expectations. This suggests adolescents are not being equipped with healthy, positive strategies to face challenges/stressors and prevent illness complications. This is not unique to the UAE, as similar issues have been reported in the international literature. Specific problems include shortages of school nurses, the growing number of children managing ill health at school (CBC News, 2019; Wofford, 2019) and the impact of school absences when appropriate support is not available (Looman and Farrag, 2009).
Improving school healthcare services may promote the health and welfare of adolescents with long-term health conditions. When functioning, these services may become a first choice for adolescents to access when they experience health problems. For example, many participants spoke positively about their school healthcare experiences when the healthcare provider was knowledgeable, approachable and available. Good quality services for children and adolescents with long-term health conditions need to be responsive, timely and provided by knowledgeable, competent healthcare providers (Al-Yateem et al, 2016b).
Adolescents with long-term health conditions used negative coping strategies because of limitations in available care, especially in school where carers were not available, approachable or knowledgeable about their health condition/needs. Home-based carers may also lack training or knowledge about their child's health condition, and families may experience conflict/difficulties; all of which affect a carer's ability to care for their child. Peer pressure and adolescents' own need to be ‘normal’ may also push them to ignore/avoid their illness in an attempt to ‘live normally’.
Long-term health conditions place a significant burden on healthcare systems. The 2002 World Health Report indicated that long-term health conditions would account for 60% of the global burden of disease by 2020. Although this report included long-term health conditions among older adults, it highlights the importance of reducing the effect of this problem on all individuals and healthcare systems (WHO, 2002).
Study limitations
The written responses to open-ended questions offered an anonymous opportunity for participants to reflect on their experiences and provided important findings; however, it precluded the possibility of asking participants to elaborate or clarify a point. In addition, many incomplete/unclear responses were excluded from analysis, which could have been avoided if data were collected in individual in-depth interviews.
The multiple authorities managing school health services in the UAE hindered the acquisition of an accurate sampling frame and data about the schools and students' details. Therefore, probability sampling was not possible, and convenience sampling was used. In addition, the response rate could not be calculated as the total size of the population could not be determined. This might have affected the generalisability of the study results.
Finally, although the CSI-S has been widely used with adult populations, it has not been similarly used among adolescents. However, the analysis of adolescents' qualitative narratives supported the questionnaire results, which provided some certainty about the validity of the questionnaire among this population.
Conclusion
School-based healthcare services offer an opportunity for health promotion and prevention, especially for adolescents with long-term health conditions. However, school healthcare providers need support and training to perform their roles efficiently. Barriers to effective school healthcare services identified in this study may inform the development of school services to better support this population.
Increased investment in support for adolescents and their carers is necessary to develop healthy coping strategies among adolescents early in their illness. This will protect them from developing negative/maladaptive coping strategies, and may reduce the burden of complications on adolescents, their families and the healthcare system. Extra support for girls with long-term health conditions should be considered in the UAE and other countries with similar cultural contexts.
Future studies could focus on designing and evaluating interventions that encourage adolescents with long-term conditions to adopt positive coping mechanisms. The needs of this population and the elements of high-quality services should be emphasised in health professional education to ensure they can respond to the needs of this vulnerable group. Furthermore, specialised training for school nurses (eg a specialty qualification) needs to be high on the healthcare service development agenda.