

The primary goal of lymphoedema management is the prevention of oedema exacerbation and cellulitis (International Lymphoedema Framework, 2006). The condition can be managed conservatively or surgically. For conservative treatment, complex decongestive therapy is recommended: this includes skin care, manual lymphatic drainage, compression therapy, exercise therapy and self-care instruction (International Lymphoedema Framework, 2006). These conservative techniques have been shown to be efficacious: improved outcomes include decreased oedema, decreased recurrence rate of cellulitis and improved quality of life (Li et al, 2016; Mendoza and Amsler, 2023; Webb et al, 2023). However, a survey of patients with lymphoedema in Japan and abroad found that the recurrence rate of cellulitis was as high as 50% (Dai et al, 2019), suggesting that lymphoedema management goals are not being met fully.
One possible reason for this clinical challenge is poor access to lymphoedema specialists, a group of professionals that includes therapists. A previous study showed an association between a history of cellulitis and poor access to lymphoedema specialists (Dai et al, 2021). This indicates the need to establish a system to provide increased access to specialists. However, in Queensland, Australia, survivors of gynaecological cancers who had lymphoedema reported a higher need for physical/daily living support, which was especially the case for those residing less populated and remote areas (Beesley et al, 2008). In Japan, facilities that include experienced lymphoedema specialists are unevenly distributed by region, so it is important to increase the availability and access to these specialists for both patients and healthcare providers.
The authors therefore developed a remote system for the management of lymphoedema. In recent years, telemedicine and telenursing have attracted attention for a range of reasons, including the prevention of spread of infectious diseases (Ökten and Gündoğan, 2022), ageing populations and regional disparities in health care (Cao et al, 2024): for example, countries such as the UK have published guidelines on the remote treatment of people with lymphoedema (Noble-Jones et al, 2021). Using a remote system enables health professionals to monitor a patient's affected limbs and self-care status, despite variations in local or regional facilities. Furthermore, the authors consider that telemedicine technology facilitates patient access to lymphoedema care specialists, enabling oedema exacerbations and cellulitis outbreaks to be better treated and managed. In Japan, not having access to care is estimated to affect oedema exacerbations and cellulitis outbreaks. (Dai et al, 2021).
In other specialties, telemedicine has been shown to be effective in improving self-care and regular treatment management in diabetic patients (AkbariRad et al, 2023), and to manage and alleviate symptoms in postoperative prostate cancer patients (Sato, 2020). According to the authors cited above, the ability of health professionals to communicate with patients remotely in real time supports patient assessment and the collection of patient data, leading to early detection and treatment of symptoms. Additionally, remote systems have enabled non-specialists to more readily connect with specialists and therapists. Based on the research cited above, the quality of treatment and care can be further improved by directly connecting patients with specialist professionals.
Research on remote management has been used to verify the feasibility of exercise therapy (Wazir et al, 2020; Mortimer et al, 2024) and the development of a system to monitor the progression of lymphoedema (Rajab et al, 2023; Syed Ibrahim et al, 2023). However, the effectiveness of health professionals providing patients with education on the conservative lymphoedema management of their condition, including self-care, has not been explored. Failure to connect patients with lymphoedema specialists may lead to exacerbation of oedema and increased recurrence of cellulitis.
Therefore, the authors decided to develop a remote self-care education system for lymphoedema patients and to verify its feasibility. The study involved a local health professional and a specialist lymphoedema therapist providing a joint consultation with the patient.
Purpose
The case study illustrates how a remote system was used to provide conservative lymphoedema therapy that included patient education and self-management. The specialist was a certified lymphoedema therapist (CLT); in Japan, accreditation for this role can be gained by a range of health and allied health professionals, such as doctors, nurses and physical therapists.
Method
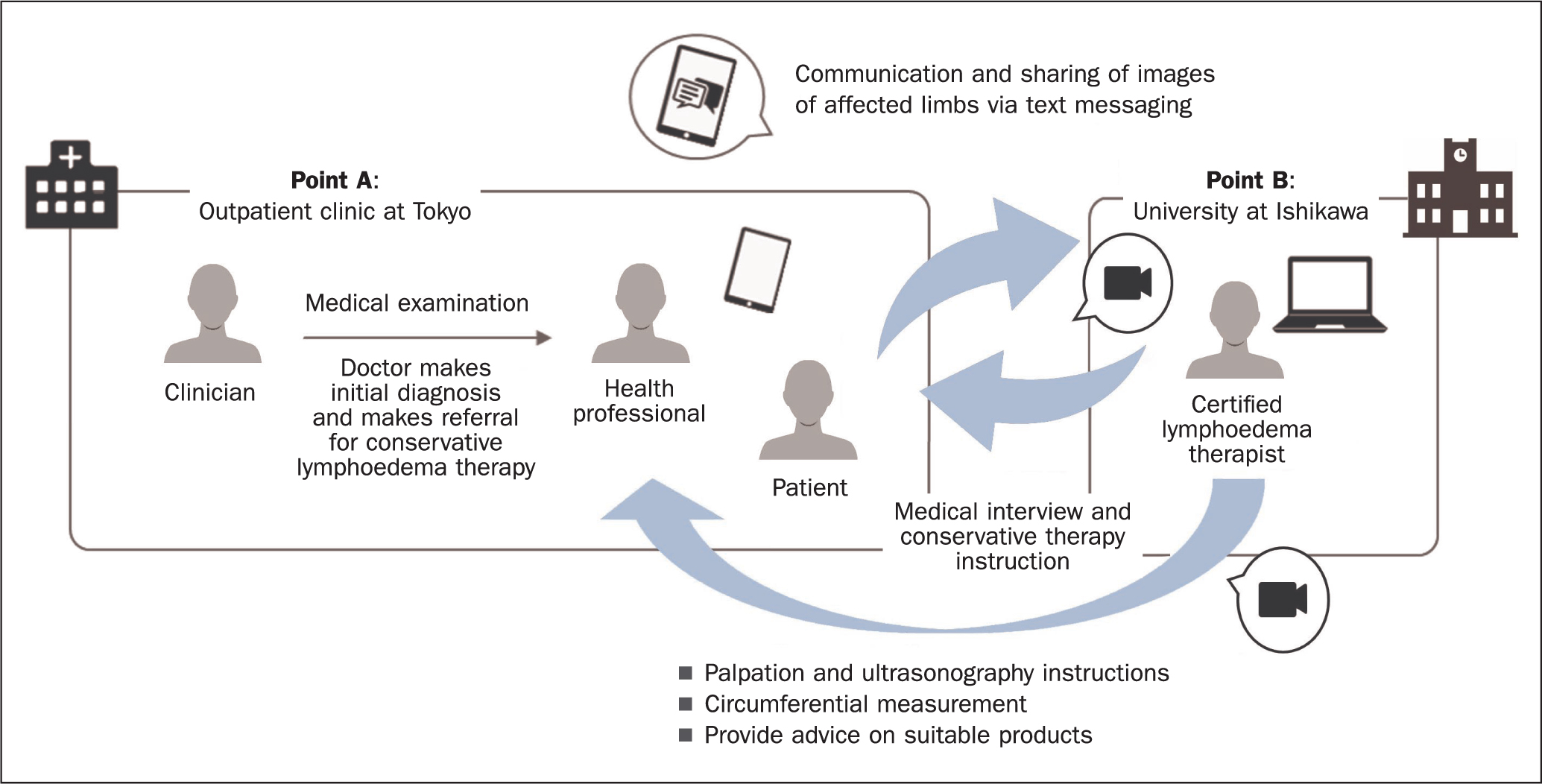
Figure 1 provides an overview of the system, which uses the Kaleido TOUCH® telecare system (D‘PULA Medical Solutions Corporation) that facilitates remote real-time audiovisual and text communication, and image transfer between points A and B via dedicated equipment that includes a handheld device with a camera. In the case study, the system was used to connect the patient and two health professionals, one of whom was present with the patient at the local outpatients clinic in Tokyo (point A) while the other, the CLT, was based at Ishikawa University. The distance between the two points is about 200 km. The technology enabled the therapist based at point B to provide guidance to the patient on lymphoedema self-care and daily care, with the support of the local health professional, who was at point A with the patient, via video and the chat function.
The system was developed in accordance with the Guidelines for Appropriate Implementation of Online Medical Treatment (Ministry of Health Labour and Welfare, 2023), which ensures that patient information is securely handled. The remote monitoring system and purpose of the study were explained to the patient, orally and in writing. The patient provided written informed consent to take part. In advance of the study, the two health professionals shared the conservative treatment protocols. The patient's details were anonymised for analysis by the researchers.
Case study
The patient was a 35-year-old woman with secondary lymphoedema of both lower extremities following surgery for uterine cancer, who subsequently developed cellulitis several times. She had experienced lymphoedema with recurrent cellulitis and underwent lymphatic venous anastomosis (LVA).
The patient began to manage the lymphoedema through self-care following LVA wound healing. The lower limbs were classified as having stage 2 (moderate) lymphoedema as per International Society of Lymphology (2009) classification. The local health professional in the outpatients clinic at point A did not have experience of conservative treatment of lymphoedema. Therefore, self-care and daily living education for complex decongestive therapy was provided to the patient remotely by the CLT who had more than 10 years' experience.
Practicalities of remote self-care education
Lymphoedema observation and assessment
Table 1 shows the interactions, observations and measurements that can and cannot be carried out remotely in order to provide a patient with guidance on self-care and to deliver lymphoedema therapy. The interactions with the patient in the case study are described below, guided by the necessary steps as set out in Table 1.
| Sequence of steps | In-person interactions between patient and local health professional and face-to face observations necessary to deliver self-care education and therapy | Communication/assessment method with remote certified lymphoedema therapist (CLT) | Assessment |
|---|---|---|---|
| Greetings/introduction | Patient acceptance to receive conservation lymphoedema therapy instruction remotely | Video calls with patients | ◯ |
| Listening to audio | Video calls with patients | ◯ | |
| Face-to-face on-screen communication with specialist at Point B | Video calls with patients | ◯ | |
| Interview | Local health professional obtains the patient's current and previous medical history (gynaecological and breast cancer, and treatment), onset of disease, skin colour changes, progression of oedema, presence or absence of pain, presence or absence of cellulitis, onset of disease and site, history of treatment for lymphoedema and its effects, daily life and work | Video calls with patients |
◯ |
| Visual examination | Local health professional records general observations about the patient (facial impression, posture, functional anatomy, movement harmony) | Observation through video images | △ |
| Left-right difference in oedema, running of surgical scars, and presence/absence of clothing encroachment, presence of neurological symptoms, lymphocoele, lymph leakage, lymph fistula | Observation through video images | ◯ | |
| Skin colour change/rash, skin tension | Observation through video images | △ | |
| Physical examination | Palpation (skin hardness, skin temperature, presence of Stemmer sign, pressure scar formation, skin dryness, sclerosis, keratinization, and elephantiasis), undertaken by the local health professional | Sharing of palpation results, with the in-person health professional providing the remote CLT with information/measurements | X |
| Imaging | Ultrasonography undertaken at point A by the local health professional to determine oedema status and distribution: thickening of epidermis and dermis layers, decreased echoluminance, fibrous tissue breakdown, thickening of subcutaneous fat layer, increased echoluminance) | View images taken by health professional via chat |
△ |
| Doppler (presence of venous complications) | – | ||
| Measurements | Measurement of water content in affected limb | – | |
| Measurement of the circumference of affected and healthy limbs | The sharing of measurements by the health professional at point A with the patient and the remote CLT at point B | X |
◯ Factors that were not a problem, even remotely
△ Factors that were not possible remotely
X Factors that were partially acceptable remotely
– Factors that were not implemented in this case study
Greetings/introduction
The introductory greetings were smooth, and included gaining consent for remote audiovisual instruction, which allowed both parties to communicate in real time.
Interview
The CLT at point B was able to converse with the patient and understand the cause and the location of cellulitis, whether the patient wore stockings – noting the type and duration of wear, and providing the patient with verbal advice on how to apply stockings correctly. The presence or absence of pain, work status, allergies, and daily activities were also noted by both clinicians.
Visual examination
With the help of the health professional at point A who was with the patient, the shape of the affected limb, presence or absence of wounds, rash, erythema and skin tightness were observed and shown to the CLT using the handheld camera. However, it was difficult for the CLT to adequately observe these clinical manifestations due to the low resolution of both the camera at point A and the screen at point B.
Physical examination
Assessment of the patient's lymphoedema included palpation by the local health professional, as it was clearly not possible for the remote CLT to do this. The severity of the lymphoedema was determined by the level of skin hardness and the presence of Stemmer's sign, with the findings communicated verbally to the specialist at point B.
Imaging
This again was not possible for the CLT at point B to undertake directly, so the local clinician took images of the affected limb and performed ultrasonography. The images and ultrasound scan results were then shared with the CLT as image and video information.
Measurements
The local clinician made measurements of the patient's ankle, lower leg, thigh and below-knee circumferences of both the affected and healthy limbs, with the information once again, being conveyed verbally to the remote CLT.
Conservative therapy education
Based on the results of the assessment undertaken by the local clinician, the CLT was able to provide the patient with guidance on managing the lymphoedema (Table 2).
| Sequence of steps | Requirements for conservative therapy education | Communication/assessment method with certified lymphoedema therapist (CLT) | Assessment |
|---|---|---|---|
| Self-assessment and self-care education | Prevention of oedema exacerbation, confirming the patient's understanding of oedema, providing information on factors to observe, and identifying exacerbating factors. This includes stressing the need to avoid sitting or standing for prolonged periods of time, avoiding excessive muscle movement and heavy work, the importance of elevating the affected limb, avoiding excessive pressure on the limb, and continuing with treatment for systemic and venous diseases). It is also important to stress the need for good weight management | Video calls with patients | ◯ |
| Preventing the development of cellulitis (confirming awareness of the disease and explaining the risks of cellulitis, teaching observation points and skin care: skin protection and moisturising, maintaining cleanliness and dealing with emergencies) | Video calls with patients | ◯ | |
| Practice of care | Manual lymphatic drainage (educating the patient on how to carry out lymphatic drainage) | – | |
| Compression therapy (how to select appropriate compression bandages and garments based on the results of observation and assessment, and educating the patient on how to apply them correctly) | Video calls with patients |
△ | |
| Exercise therapy in compression (exercise therapy instruction) | – | ||
| Lifestyle guidance | Counselling and guidance on appearance, sexuality and bladder voiding (patients may have urination difficulties due to oedema in the genital area). Providing advice on work and carrying out household chores | Video calls with patients | ◯ |
◯ Factors that were not a problem, even remotely
△ Factors that were not possible remotely
X Factors that were partially acceptable remotely
– Factors that were not implemented in this case study
Self-assessment and self-care education
The patient received education from the remote CLT on how to perform a self-check, to enable her to assess her own skin and degree of oedema. In addition, she received advice on self-care, skin care, drainage, exercises, and on the importance of avoiding extended periods of sitting or standing.
Practice of care
The CLT advised the patient on the use of compression therapy: namely, the most suitable type of compression garment (pantyhose style) and correct sizing (2L), along with the required optimal compression pressure (30 mmHg), based on the interview/observation of the patient, circumferential diameters, and ultrasonography. The method of putting on and removing the garment was explained, including when to remove it if the patient had any concerns.
The inability of the CLT to check the fit of the garment is a limitation of the remote system, but this was overcome by having the local health professional with the patient at point A.
Lifestyle guidance
The main concern expressed by the patient during the consultation was regarding the risk of infection. In response to the patient's responses to questions, general skin care advice was provided by the CLT to reduce risk factors for cellulitis.
Follow-up clinic visit
Four months after the initial consultation, the patient visited a lymphoedema outpatient clinic, but did not request a follow-up remote self-care consultation. There was no worsening of the oedema or recurrence of cellulitis on the affected limbs (Table 3).
| Area measured | At initial remote session with certified lymphoedema therapist (CLT) | At 4-month follow-up | ||
|---|---|---|---|---|
| Right leg | Left leg | Right leg | Left leg | |
| 10 cm above the knee | 49 cm | 46 cm | 50 cm | 44 cm |
| 10 cm below the knee | 43 cm | 43.5 cm | 42 cm | 40 cm |
| Ankle | 27 cm | 28 cm | 26 cm | 28.5 cm |
Discussion
This is the first study to report on the remote management of lymphoedema, using telemedicine to connect the patient and local health professional, both based in the outpatient clinic, with a remotely based CLT, who was able to provide self-care guidance and advice via this approach to consultation. Although the effectiveness of face-to-face conservative therapy for lymphoedema has been previously reported (International Lymphoedema Framework, 2006), the authors' systematic review did not find any reports evaluating remote self-care education. This case study revealed the usefulness of providing remote self-care guidance in lymphoedema management, as well as related issues. In addition, in this case study, communication between the patient and health professional at point A and the CLT at point B was straightforward, but differed from conventional communication between health professionals and patients, in that it included the involvement of two professionals (one of whom was with the patient), who were able to share information and provide the patient with relevant education and advice. This system could offer a new approach to delivering telemedicine.
The greetings and interview steps in the preliminary observation and assessment of the patient's lymphoedema status, and the subsequent self-care education, met the requirements of the management protocol used and no problems were encountered (Tables 1and2). Communication with the patient through video and observation of the affected limb were possible, just as they can be carried out in person. The key reason that remote lymphoedema self-care education and guidance were possible was due to the collaborative development and application of the lymphoedema management protocol between the health professional at point A and the CLT at point B. The protocol allowed both clinicians to provide the patient with the same level of care as they would receive during a face-to-face consultation. It allowed healthcare providers at both points to implement the same patient goals with a common understanding of self-care education plans and methods.
Parts of the visual examination and screen diagnosis were partially feasible, even remotely. Although it was possible to observe the appearance of the affected limb on-screen, it was difficult to identify skin tone and texture; this issue was attributed to insufficient camera and video screen resolutions. The assessment of skin texture becomes more important as severity of lymphoedema increases. Improvement and development of better techniques, for example, by having access to equipment with higher image resolution, are considered necessary. Although palpation is also essential for assessing lymphoedema severity, this limitation of remote assessment was mitigated by the presence of a health professional who was able to assess and verbally communicate the observations and measurements. A further point is that, although not applicable in the present case study, patients with lymphoedema of the lower limbs may develop oedema in the genital area, which requires monitoring.
Tasks that are not possible to remotely perform include palpation, limb circumference measurement, and lymphatic drainage. Skin firmness is an important characteristic in the observation of lymphoedema, and circumference measurement and ultrasonography are important indicators for assessing oedema status (International Lymphoedema Framework, 2006). In addition, the CLT was unable to check the fit of elastic compression garments, or to undertake lymphatic drainage using palpation techniques. It is worth noting that patients have reported being satisfied and reassured when a health professional examines their skin in a face-to-face consultation (Da Rocha Rodrigues et al, 2021), although, in this study, the authors did not evaluate this aspect.
A second remote self-care instruction session was not required for the case study patient, for which there are two possible reasons. First, there were no issues to discuss because there was no history of oedema exacerbation or cellulitis recurrence. It has previously been reported (Briet et al, 2014) that patients seek online access to specialists when they are dissatisfied with their treatment or want to seek further information, and it is possible that this patient did not meet these criteria. Second, the patient may not have been satisfied with the remote self-care education. It has been reported that, when patients have a choice between face-to-face care and telemedicine, they tend to choose the face-to-face option (Elhakeem et al, 2022). Patients' needs therefore may be more readily met face to face compared with remote assessments.
Based on the possibilities and challenges of remote self-care education identified in this case study, the authors plan to undertake further work to refine and improve the system and management protocol. The authors therefore propose a protocol whereby conservative therapy is initially provided in person, with palpation and care performed and education provided. Following this, the patient's ability to continue these activities independently can be evaluated remotely. To increase patient satisfaction with complex decongestive therapy, a hybrid format is important, including having regular face-to-face interactions and remote self-care education. In addition, the authors consider it necessary to develop objective tools to enable the face-to-face outpatients health professional and the remote CLT to simultaneously assess skin hardness for more accurate information sharing. The authors consider that some aspects of care implementation can be followed by introducing methods to remotely educate patients on the use of lymphatic drainage and compression therapy using virtual reality. This would require that health professionals and CLTs involved in telemedicine consultations are themselves provided with adequate education and training in conservative lymphoedema management therapies.
In the case described in this article, communication was established between the patient and health professional at point A and the CLT at point B. This was made possible by the fact that the local health professional and the CLT at the target facility had a history of collaboration. Although the feasibility of a similar model between facilities with no history of collaboration could not be demonstrated, there is no reason why the system cannot be potentially extended to other regions and facilities in future. However, further studies are required.
Although patient satisfaction was not evaluated, this case study suggests that it is possible to implement a telecare system to deliver patient education in conservative lymphoedema therapy. In future, the authors recommend that longitudinal observation and accumulation of cases are conducted to verify the effectiveness of the educational guidance, and to compare this with the effectiveness of face-to-face education, as well as evaluating patient satisfaction.
Conclusion
A remote system connecting a patient and a health professional who were both in the outpatients clinic, with a CLT was proposed as a method of conservative treatment for lymphoedema. The authors' case study evaluated the role of remote lymphoedema management using conservative therapy. The findings suggest that implementation of this system is beneficial for patients and health professionals, and would particularly benefit rural regions where access to healthcare services may be more difficult. Future studies are necessary to confirm the effectiveness of this approach and evaluate its efficacy in providing high-quality treatment.