
Health literacy (HL) was defined by the World Health Organization in 1998 as: ‘The cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health’. Patients with liver cirrhosis, which is a chronic and complex disease, are required to understand and act on many health messages and understand the organisation of the healthcare system to enable them to act and take precautions to maintain optimal health status.
Furthermore, liver cirrhosis can lead to episodes with hepatic encephalopathy (HE). This is a debilitating manifestation of liver disease, affecting the lives of patients and their relatives (Bager, 2017) that will vary between patients and within an individual over time. If liver cirrhosis is accompanied by HE, patients' ability to understand and act appropriately on health issues will be impaired. When developing disease-related material for patients with liver cirrhosis, it is therefore vital to take into account individual patients' different levels of HL. Consequently, it is imperative for nurses providing information to patients to understand a patient's level of HL.
The most common measure for assessing HL are self-administered questionnaires. However, if patients have difficulties with self-administration, the questionnaire can be completed using an interview approach. The Australian Health Literacy Questionnaire (HLQ) is a validated and comprehensive questionnaire (Osborne et al, 2013) consisting of 44 questions that cover nine conceptually distinct areas of HL. However, in a group of patients, of whom a considerable proportion is vulnerable, there is a question over whether such a long questionnaire is feasible. A less comprehensive questionnaire might be more useful as a screening tool in clinical practice. Face validity is one measure that can be used to assess validation of questionnaires: it includes evaluating the overall appearance of the questionnaire, the questionnaire design, and the number of questions included.
The aims of the study were to test the face validity of three HL questionnaires and to reveal possible factors for low face validity in a population of outpatients with liver cirrhosis.
Methods
Participants
Adult patients with liver cirrhosis were included consecutively from the liver unit outpatient clinic at Aarhus University Hospital, Denmark. Patients with HE or known severe cognitive impairment (eg, dementia or psychosis) were excluded. Assessment of HE was performed as a clinical judgement by a consultant. Patients were enrolled in the study over a period of 3 months until about 25% of the entire pool of patients with cirrhosis was included (n=108).
Questionnaires
All the patients were required to complete three HL questionnaires, which were administered to participants in a random sequence. The questionnaires were the Single Item Literacy Screener (SILS), the Brief Health Literacy Screening Tool (BRIEF), and three domains of the Health Literacy Questionnaire (HLQ) (Morris et al, 2006; Haun et al, 2009; Osborne et al, 2013). Furthermore, patients were asked to complete the EQ-5D-3L, developed by the EuroQol Group (Rabin and de Charoo, 2001), to record their current health status, and to provide sociodemographic information. If the patients needed help with the questionnaires, the need was assessed by the investigators. The scores and interpretation of the results were accomplished according to the scoring manual for each instrument. Permission to use the questionnaires was given by the progenitors of the tools.
Single Item Literacy Screener
The SILS instrument is a single-item screening tool to identify limited reading ability. The SILS asks: ‘How often do you need to have someone help you when you read instructions, pamphlets, or other written material from your doctor or pharmacy?’ Possible responses are:
Scores greater than 2 were considered to be positive, indicating some difficulty with reading printed health-related material (Morris et al, 2006). The question was translated into Danish by the investigators and pilot tested in a subpopulation of 10 patients.
Brief Health Literacy Screening Tool
The BRIEF tool was developed in the USA and comprises four questions (Haun et al, 2009; 2012):
Each question has five response options on an ordinal scale. The four items were translated into Danish by the investigators and pilot tested in a subpopulation of 10 patients.
Health Literacy Questionnaire
The full HLQ encompasses 44 items split into nine domains. However, it is possible to use each domain separately. The three domains—‘Social support for health’ ‘Ability to actively engage with healthcare providers’ and ‘Understand health information well enough to know what to do’—were used in this study. Each of the domains consists of five questions. The response options were:
The HLQ was validated in a Danish context in 2016 (Maindal et al, 2016).
EQ-5D-3L
The EQ-5D-3L is a generic instrument for measuring health-related quality of life (HRQoL), which has been validated in a variety of international settings both among general populations and in patient studies (see www.euroqol.org). There is also a Danish version of the questionnaire. The EQ-5D-3L classification system comprises 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each of which has three levels (no problems, moderate problems, and extreme problems) (Rabin and de Charro, 2001).
A single index score can be derived by combining the levels of each dimension. If the response was ‘no problems’ in all five dimensions, the health stage will be regarded as ‘full health’. In total, 243 different health stages can be derived from the questionnaire.
Randomisation
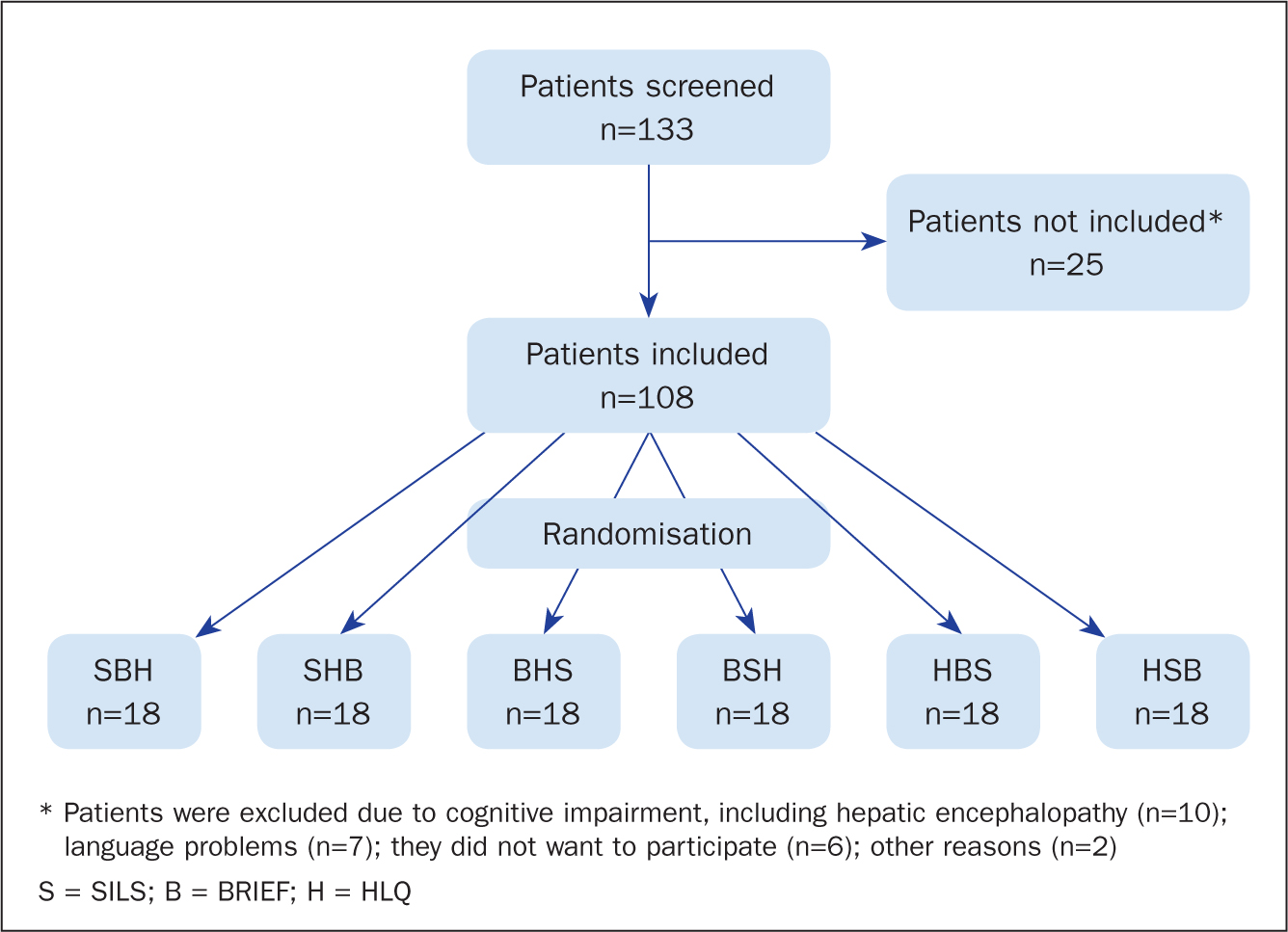
In order to avoid bias, the three HL-questionnaires were assigned randomly. Randomisation was done using http://www.randomization.com. Patients were randomly assigned to one of six groups (Figure 1).
Disease and sociodemographics
In addition to the HL and HRQoL-questionnaires, sociodemographic data and some disease-related information were obtained from the patients' electronic medical records (type of cirrhosis, severity of cirrhosis and comorbidity).
Statistics
The results were expressed as percentages, means and standard deviations (SD). Student's t-test or Fisher's exact test were used to test for differences. The software programs EpiData Entry v3.02 (EpiData Association) and Stata v15 (StataCorp LLC) were used for data entry and analysis.
Ethics
Patients were informed that participation was voluntary and that returning a completed questionnaire would be considered as giving informed consent. According to Danish law, approval from the Danish Ethical Committee was not necessary. The study was approved by the Danish Data Protection Agency (Reg. nr. 1-16-02-874-17), as required. Permission was sought from and obtained by the progenitors of the questionnaires to use them in the study.
Results
Between November 2017 and February 2018, 133 outpatients were screened for the study. Twenty-five patients were not included, mainly due to HE, cognitive impairment and language problems. The remainder (n=108) were randomised to one of six groups for allocation to the three HL questionnaires (Figure 1). A total of 39 patients (36%) needed help to complete the HLQ tool. The patient characteristics are presented in Table 1. The majority of patients had alcohol-related liver cirrhosis (65%); most were born in Denmark (90%) and spoke Danish at home. Furthermore, the majority of patients were retired (70%).
| All (n=108) | Needed help (n=39) | Not needed help (n=69) | P value | |
|---|---|---|---|---|
| Gender [men], n(%) | 59 (54.6) | 27 (69.2) | 32 (46.4) | 0.03 |
| Age, mean years (SD) | 60.6 (9.4) | 59.9 (11.0) | 61.0 (8.5) | 0.59 |
| Cohabitation [yes], n(%) | 67 (63.8) | 23 (59.0) | 44 (66.7) | 0.53 |
| Country of birth, n(%) | 0.45 | |||
| Denmark | 97 (89.8) | 35 (89.8) | 62 (89.9) | 1.00 |
| Inside Europe | 6 (5.6) | 2 (5.1) | 4 (5.8) | 1.00 |
| Outside Europe | 5 (4.6) | 2 (5.1) | 3 (4.3) | 1.00 |
| Speaks Danish at home [yes], n(%) | 102 (96.2) | 36 (92.3) | 66 (98.5) | 0.14 |
| Education, n(%) | ||||
| < 8 years | 12 (11.1) | 8 (20.9) | 4 (5.9) | 0.03 |
| 8–9 years | 26 (24.3) | 9 (23.1) | 17 (25.0) | 1.00 |
| 10–11 years | 31 (29.0) | 14 (35.9) | 17 (25.0) | 0.27 |
| Student | 28 (26.2) | 5 (12.8) | 23 (33.8) | 0.02 |
| Other | 10 (9.3) | 3 (7.7) | 7 (10.3) | 0.74 |
| Employment, n(%) | ||||
| Employed | 14 (13.0) | 0 (0.0) | 14 (20.2) | 0.01 |
| Unemployed | 10 (9.2) | 4 (10.3) | 6 (8.7) | <0.01 |
| Retired | 76 (70.4) | 32 (82.1) | 44 (63.8) | 0.87 |
| Missing | 8 (7.4) | 3 (7.6) | 5 (7.3) | 0.03 |
| Cirrhosis diagnosis, n(%) | ||||
| Alcoholic | 70 (64.8) | 31 (79.5) | 39 (56.5) | 0.02 |
| PBC | 20 (18.5) | 3 (7.7) | 17 (24.6) | 0.04 |
| Cryptogenic | 3 (2.8) | 0 (0.0) | 3 (4.4) | 0.55 |
| Other | 15 (13.9) | 5 (12.8) | 10 (14.5) | 1.00 |
| Complications, n(%) | ||||
| TIPS, current | 19 (18.0) | 4 (10.3) | 15 (21.7) | 0.19 |
| UGIB, previously | 30 (27.8) | 12 (30.8) | 18 (26.1) | 0.66 |
| HE, previously | 34 (31.5) | 16 (41.0) | 18 (26.1) | 0.13 |
| Severity, n(%) | ||||
| Child Pugh A* | 55 (50.9) | 14 (35.9) | 41 (59.4) | 0.02 |
| Child Pugh B* | 45 (41.7) | 21 (53.9) | 24 (34.8) | 0.04 |
| Child Pugh C* | 8 (7.4) | 4 (10.2) | 4 (5.8) | 0.31 |
| Comorbidity, n(%) | ||||
| None | 23 (21.3) | 4 (10.2) | 19 (27.6) | 0.03 |
| 1 | 52 (48.1) | 19 (48.8) | 33 (47.8) | 0.92 |
| 2 | 25 (23.1) | 12 (30.8) | 13 (18.8) | 0.16 |
| >2 | 8 (7.4) | 4 (10.2) | 4 (5.8) | 0.40 |
SD = standard deviation; PBC = primary biliary cholangitis; TIPS = transjugular intrahepatic portosystemic shunt; UGIB = upper gastrointestinal bleeding; HE = hepatic encephalopathy
Strong indicators for the need to have help with compiling the HLQ were that they:
All the patients who required help to complete the HLQ also needed help to complete the BRIEF and SILS questionnaires, as well as the EQ-5D-3L questionnaire. As the need to have help with completion applied to all questionnaires, the random order of allocating patients to questionnaires turned out to be unimportant. The need for help to complete the HLQ was also associated with reduced HRQoL. As shown in Table 2, reduced HRQoL was significantly associated with the need for help, especially if respondents had mobility problems and if their general health status was reduced. Problems with self-care, pain/discomfort, and anxiety/depression were found to be non-significant.
| All (n=106*) | Needed help (n=39) | No help (n=67) | P value | |
|---|---|---|---|---|
| EQ-5D-3L | ||||
| 11111 (full health), n(%) | 22 (20.8) | 3 (7.7) | 19 (28.3) | 0.01 |
| Mean EQ-5D-3L index score (SD) | 7.3 (1.8) | 7.6 (1.7) | 7.1 (1.8) | 0.10 |
| Mobility | ||||
| No problems, n(%) | 60 (56.6) | 15 (38.5) | 45 (67.2) | < 0.01 |
| Some problems, n(%) | 46 (43.4) | 24(61.5) | 22 (32.8) | < 0.01 |
| Confined to bed, n(%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Self-care | ||||
| No problems, n(%) | 91 (85.8) | 31 (79.5) | 60 (89.6) | 0.15 |
| Some problems, n(%) | 15 (14.2) | 8 (20.5) | 7 (10.4) | 0.15 |
| Unable to wash or dress, n(%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Usual activities | ||||
| No problems, n(%) | 49 (46.2) | 18 (46.2) | 31 (46.3) | 0.99 |
| Some problems, n(%) | 48 (45.3) | 20 (51.3) | 28 (41.8) | 0.34 |
| Unable to perform, n(%) | 9 (8.5) | 1 (2.5) | 8 (11.9) | < 0.01 |
| Pain/discomfort | ||||
| No problems, n(%) | 39 (36.8) | 11 (28.2) | 28 (41.8) | 0.16 |
| Some problems, n(%) | 59 (55.7) | 24 (61.5) | 35 (52.2) | 0.35 |
| Extreme problems, n(%) | 8 (7.5) | 4 (10.3) | 4 (6.0) | 0.46 |
| Anxiety/depression | ||||
| No problems, n(%) | 66 (62.3) | 23 (59.0) | 43 (64.2) | 0.59 |
| Some problems, n(%) | 36 (34.0) | 13 (33.3) | 23 (34.3) | 0.91 |
| Extreme problems, n(%) | 4 (3.7) | 3 (7.7) | 1 (1.5) | 0.14 |
| Mean EQ-5D-3L visual analogue scale [0–100] (SD) | 66.5 (20.5) | 58.9 (21.8) | 70.9 (18.4) | < 0.01 |
The single SILS question, BRIEF question number one, and HLQ question 2 (information) all ask respondents about their ability to understand written health information. Figure 2 illustrates agreement between the three similar questions. Calculations found no statistical differences between answers to the three questions, neither for those who needed help nor for those who did not.
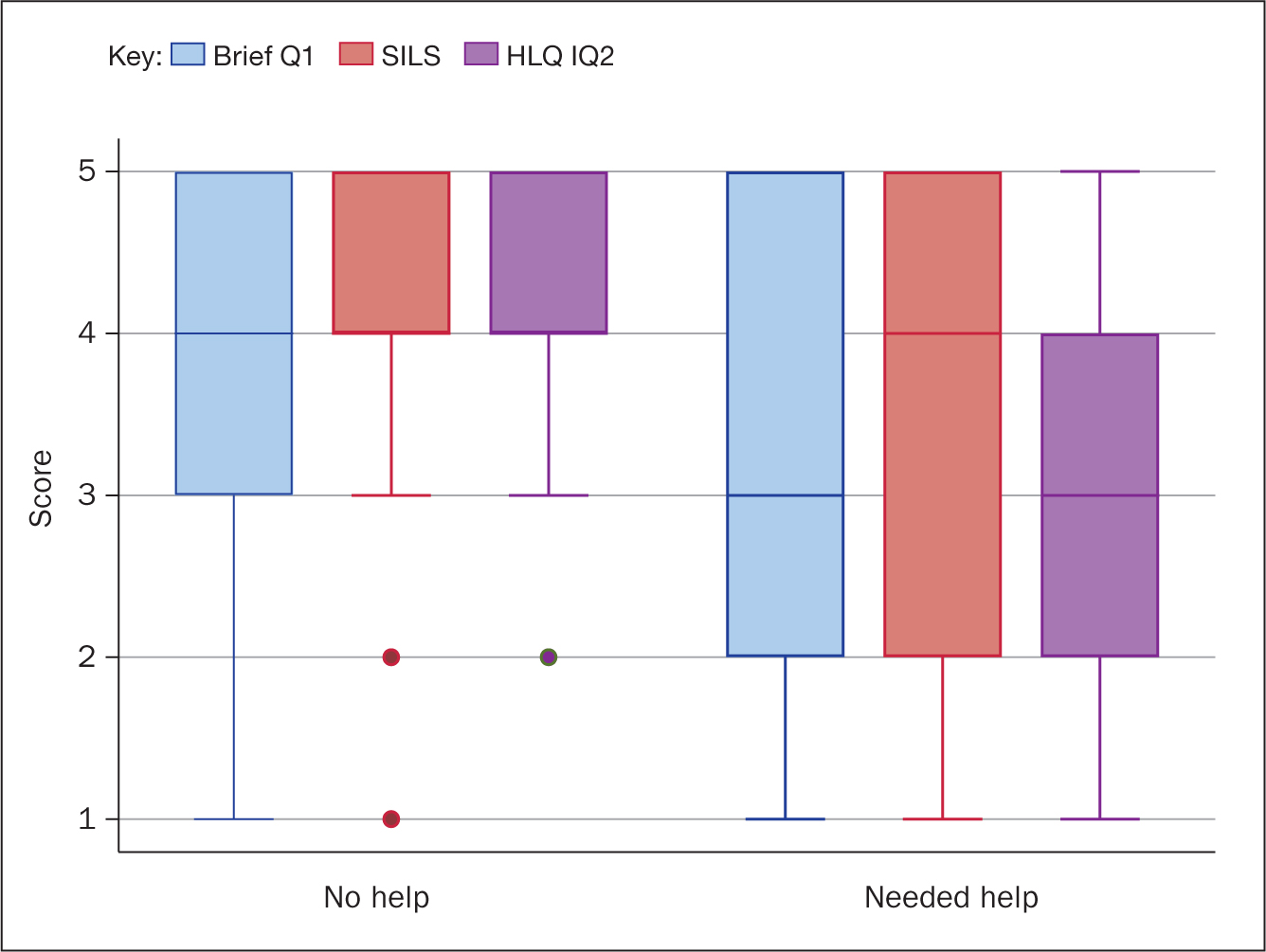
The patients who needed help expressed a fear of not giving the correct answer, mainly because they did not understand the content of the questions. Most patients who needed help had come to the outpatient clinic without a relative.
Discussion
This study reveals that monitoring HL using self-administrated questionnaires in patients with liver cirrhosis is challenging. Regardless of the length of the questionnaire, approximately one-third of participants needed help to complete them. The group of patients who needed help was characterised mainly as having a low level of education, being male, retired, and having alcohol-related liver cirrhosis. Furthermore, those who needed help had a lower HRQoL (especially reduced mobility) than those who were able to complete the questionnaires independently. Many participants also responded that they had difficulties understanding the content of the questions. This is a dilemma. The level of HL is measured mainly through self-administered questionnaires of varying lengths. If a subgroup of patients has difficulties with even a single question, alternatives must be considered. A possibility could be to guide all patients when answering the questions in order to standardise data collection; alternatively, information about HL could be revealed through qualitative interviews.
If patients with liver cirrhosis have special challenges regarding HL, consideration could be given to developing a disease-specific HL questionnaire for this group. However, there are numerous HL questionnaires. The HL home page (http://healthliteracy.bu.edu/all) lists 133 different tools. Furthermore, if one-third of patients is unable to complete even one question without help, they would face the same problems with a disease-specific HL questionnaire.
In clinical practice, one option could be to use a patient's ability to complete a self-administered questionnaire to screen for low HL. Those who ask for help can be expected to need special attention regarding information, understanding health issues, and the structure of the healthcare system. Another options, as illustrated by this study, is the need to pay special attention to those patients with alcohol-related liver cirrhosis who are male and have low levels of education.
Conclusion
One-third of patients with liver cirrhosis needed help to complete even the simplest HL questionnaire. Most difficulties were associated with alcohol-related liver cirrhosis, low level of education and being male. No self-reported HL-questionnaire was found to be ideal for this patient group. However, the longer a questionnaire is, the more information can be collected—if you can rely on the answers.