

Interprofessional collaboration (IPC) involves different health professionals working co-operatively to positively impact the quality and safety of patient care, by integrating their skills and maximising their contribution to the care of the patient. It is worth highlighting that the pandemic affected the perception of IPC, with an increase in risk perception and awareness of the importance of this way of working compared with pre-pandemic times.
One definition of IPC describes it as a simple approach that is achievable in practice but, to ensure that it works well, an imbalance of authority, disagreement between health professional groups, and poor understanding of mutual roles and responsibilities all have to be taken into account (Carradore et al, 2022). It can also be defined as a collaborative practice, with a variety of health professional groups working with patients, families and caregivers to ensure the delivery of the highest possible quality of care (Muusse et al, 2023).
Once integrated successfully into a workplace, IPC can promote behaviours that encourage true multidisciplinary teamwork, which will bring significant benefits for patients, as well as the team members themselves. IPC is particularly vital in work settings in which critically ill patients and time-dependent conditions are treated, such as acute care settings. In the literature, the term ‘acute care’ is generally used to refer to clinical settings that provide urgent care to critically unstable patients; however acute care settings encompass a much wider range of services, including emergency care, urgent care, intensive care, short-term stabilisation, prehospital care, critical care, trauma care and acute care surgery (Hirshon et al, 2013). IPC is an important defining determinant of high-quality care in intensive care units (ICU), even though its implementation is complex and its components are not clearly defined (Boltey et al, 2023).
A recent study by Carradore et al (2022) investigated to what extent and with which professionals Italian nurses in acute care settings dealt with most often. The study used a quantitative approach, combined with the IPC scale Italian version (Vittadello et al, 2017), to explore nurses' views in acute care settings, such as general ICU, specialist ICU and emergency units. It found that nurses in these settings collaborate with a range of health professionals, including radiographers. In fact, Carradore et al (2022) found that radiographers were the third most frequent group with whom the nurses in the study collaborated daily. Nurses have a vital role in supporting patients requiring mobile radiography, which is needed in cases where a patient's condition makes it impossible for them to be transported to the radiology department. The combined knowledge of health professionals involved in mobile radiography – the referring doctor, radiographer and nurse – is critical in obtaining high-quality diagnostic images and ensuring consistent diagnoses.
Aim
The purpose of this study was to investigate the perception of IPC by both nurses and radiographers in acute care settings, to help identify factors that support or hinder its implementation.
Methods
Design
A descriptive qualitative research approach that drew on feedback from focus groups with the conversation guided by a moderator was used to investigate the perception of IPC by nurses and radiographers working in acute care settings. This approach was taken because it enables better interpretation of the data and elicits rich descriptions from participants (Sandelowski et al, 2000), which can be used to inform the implementation of new interventions to improve practice.
Participants and setting
Nurses and radiographers at the Azienda USL of Piacenza took part in the study on a voluntary basis. Participants were based in the following acute care settings: the emergency room (ER), the orthopaedic emergency room (OER) that includes a ward and a radiology suite), general ICU, cardiac ICU, a haemodynamic unit and angiography. Each nurse participant worked in only one of the above settings; however, the radiographer participants worked across a number of settings (for example, ER and angiography). It was agreed to recruit nurses and radiographers who had at least 3 years' work experience in the study settings, excluding professionals with a managerial role and those not fluent in the Italian language. The inclusion and exclusion criteria are shown in Table 1.
| Inclusion | Exclusion |
|---|---|
| Nurses and radiographers: |
Nurses and radiographers: |
Recruitment took place by e-mail: an invitation was sent to staff by ward/service managers of the departments and units selected for the study. Data saturation was used to guarantee the completeness of the information (Hennink and Kaiser, 2022).
Data collection
The focus group conversations generated content for analysis and were guided by a moderator, who used a series of broad questions (see Table 2) to provide a loose structure to the discussions. The focus groups were hosted on the Microsoft Teams platform and took place in January and February 2024.
| Question 1 | What do you see as interprofessional collaboration (IPC) between nurses and radiographers in acute care settings? Are you able to define it? You should use key words too |
| Question 2 | Would you like to describe to the group what you think are the fields of competences for these two professional groups? In which areas do they collaborate? |
| Question 3 | Would you like to describe to the group your experience of IPC between nurses and radiographers, reporting some lived cases? |
| Question 4 | Are you able to describe to the group some factors that facilitate or hinder IPC between these two professional groups? |
| Question 5 | What would you recommend to promote and enhance? IPC between these two professional groups? |
| Question 6 | Are there other considerations that you would like to share? |
The first question aimed to ‘break the ice’ and was intentionally general. The second addressed mutual perceptions about the competencies of the two professional groups, to explore the topic in greater depth, with participants' basic knowledge as a starting point. They were subsequently encouraged to take part in the discussion by narrating their lived experience, to bring a more personal perspective to the conversation. These personal stories generated talking points surrounding factors that can either hinder or facilitate IPC for each group to discuss. The focus group conversations concluded with a request for participants to express their point of view, based on what they has heard in the discussion, and to provide suggestions or voice other issues they would like clarified, to enable conclusions to be made.
With the consent of participants, the conversations were audio recorded and transcribed verbatim, with the audio recording and text file then saved on an external device to ensure that only the researchers had access to the data. Each focus group was conducted by a moderator, along with a facilitator and two external observers. There were four focus groups, two consisting of radiographers and two of nurses; none mixed the two professions. The confidentiality and anonymity of participants was ensured by allocating an individual participant number, and each focus group was also identified with a code.
Data analysis
The focus group data were analysed using Braun and Clarke's (2006; 2024) thematic analysis approach, according to which data are transcribed, re-read and the main themes and subthemes identified. These were then colour coded and reviewed.
Two researchers (CR and AB) independently analysed the focus group conversations, and their conclusions were discussed by the entire research team in order to identify the overarching themes and subthemes.
Ethical considerations
The audio recordings of the focus groups were kept for the duration of the study, allowing for data transcription and analysis. Pseudonymised data will be stored on a password-protected university computer for 7 years. The study was conducted according to the good clinical practices and principles outlined in the 2024 Declaration of Helsinki.
The study was approved by the Ethics Committee ‘Area vasta Emilia Nord’ (Code No. EC 566/2023/OSS/AUSLPC). The Azienda USL of Piacenza authorised the study (resolution 2023/0000495 dated 7/11/2023.) Participants were asked to read and sign a detailed informed consent form prior to being enrolled in the study.
Rigour
The study was designed in the light of the principles of credibility, transferability, dependability and confirmability (Koch, 2006; Crowe et al, 2015; Cypress, 2017). Credibility has been ensured by reporting faithful descriptions of the entire research process and by consensus of the research group on interpretation data. This process involved the following steps:
Transferability was ensured by describing the context in which the recruitment of participants took place and the characteristics of each participant, to enable comparisons to be made with research conducted in similar and/or different contexts. Reliability was ensured by questioning the quality of all stages of data collection and analysis. To achieve confirmability, an observer was always present during the focus group discussions to take notes useful for the interpretation of the data.
In addition, the entire research group debriefed by re-checking all the material produced. These are important criteria to determine the rigour of a qualitative study (Koch, 2006; Crowe et al, 2015; Cypress, 2017).
The Consolidated Criteria for Reporting Qualitative Research guidelines (COREQ checklist) (Tong et al, 2007) have been followed to report on the findings of the study.
Results
A total of four focus groups were held, each lasting about 120 minutes, involving a total of 25 participants: 15 radiographers and 10 nurses. The first focus group included 7 radiographers (participants 1–7); the second included 8 radiographers (participants 8–15); the third and the fourth group each included 5 nurses (participants 16-20 and participants 21-25, respectively). Participants' demographic characteristics are shown in Table 3.
| Variable | Nurses | Radiographers | |
|---|---|---|---|
| Gender/Sex | Male | 3 | 8 |
| Female | 7 | 7 | |
| Years of experience | 3–5 years | 5 | 2 |
| 6–7 years | 5 | 8 | |
| 8–9 years | - | 2 | |
| 10–15 years | - | 2 | |
| More than 15 years | - | 1 | |
| Services and units | Emergency room/emergency orthopaedic room | 6 | 15 |
| Intensive care unit | 4 | - | |
| Angiography | - | 10 | |
| Haemodynamic unit | - | 3 | |
| Total | 10 | 15 | |
Focus group analysis
Four main themes/dimensions emerged from the analysis of the focus groups comments, highlighting the issues perceived as affecting collaboration between nurses and radiographers in acute care settings. These were:
The themes were synthesised using an inductive approach and are graphically presented in Figure 1. Each theme represents a conceptual area and its subthemes.
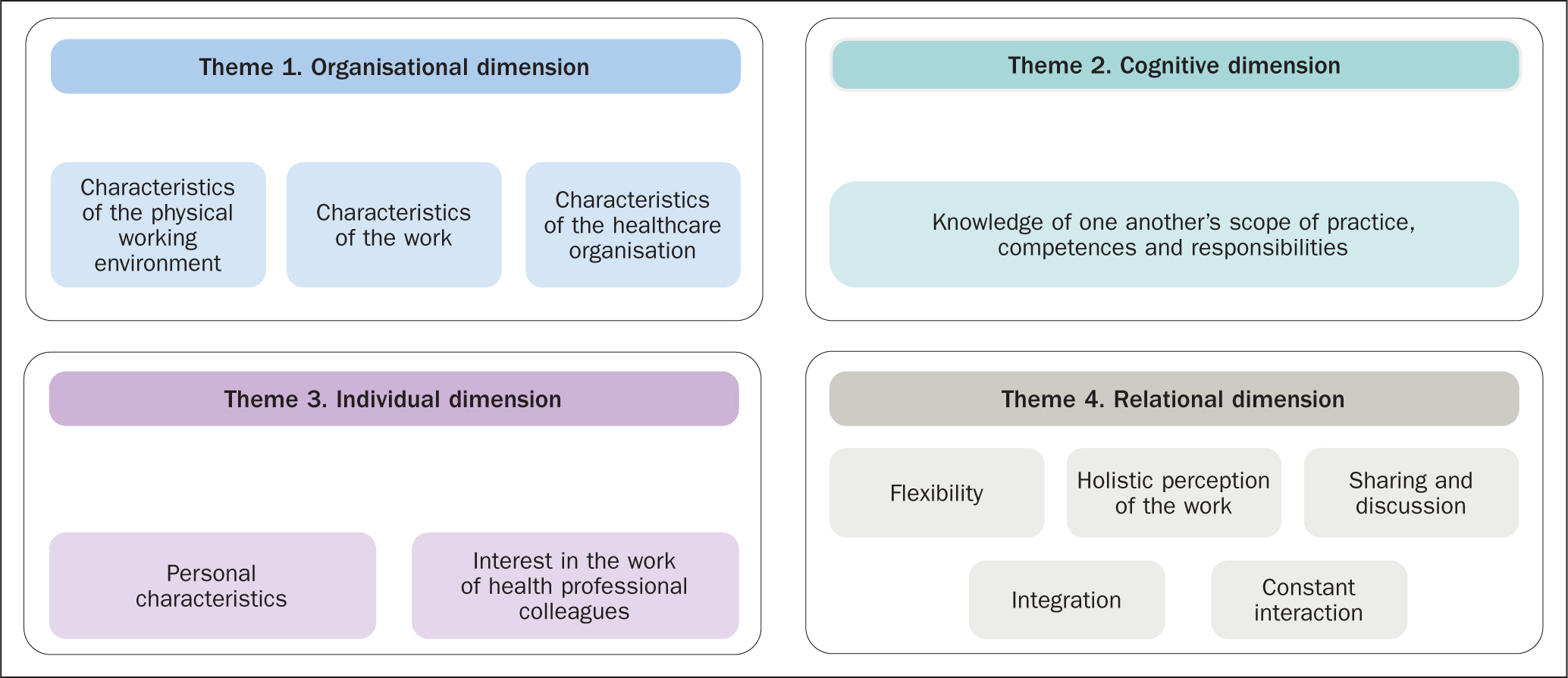
Theme 1. Organisational dimension
The organisational dimension encompasses subthemes related to the policies in place in acute care settings, including the broader policies of the healthcare organisation's strategic management. Three subthemes were identified within the organisational dimension:
Characteristics of the physical environment
This subtheme shows that, despite needing to work closely, the nurses and radiographers were expected to work in separate physical spaces. One radiographer confirmed that this was problematic:
‘Even when we are in the same emergency room, we work in two different environments … so maybe one [the radiographer] doesn't know the tasks the other [the nurse] undertakes. Often the nurse presses for certain diagnostics but maybe doesn't realise how long it takes to do them … it's not only the time to perform the examination, but the time to prepare and arrange the patient in a certain way. Similarly, maybe we [radiographers] do not know the internal dynamics that exist in emergency rooms because we do not always see how many patients they have and what confusion there is.’
‘In some diagnostics, unfortunately there is no proximity between radiographer and nurse. If I work in the radiology department of the emergency room and I do only X-rays, I have no relationship with a nurse… the nurse is not needed there.’
Characteristics of the work
This subtheme includes the workloads of nurses and radiographers (routine and unexpected, when services/wards may be overcrowded), type of work (individual or in a team), and work-related stress. Participants reported that there were differences between the two professional groups in establishing and maintaining the professional-patient relationship. One nurse stated:
‘I don't think about it, a critical patient creates much more pressure for us [nurses] than for the radiographers.’
In addition, the nurses stated that when, for example, they requested a diagnostic imaging:
‘… one day there were 15 X-rays to be taken of the same patient in general ICU. The radiographer kept coming in and out of the room … our colleagues [with another patient] also had to drop everything, go out and come back in. But we still managed to do well, with the right attitude and competent staff, because the radiographer was also impeccable and everything went well and quickly, despite the amount of work.’
‘Sometimes radiographers call to ask if I can accompany the patient to diagnostics. If I answer that I am [unable to do this] but we need the X-ray in the shortest possible time, some radiographers don't mind coming for the patient, while … other colleagues … organise external transport and don't physically come to the emergency room for the patient.’
Characteristics of the healthcare organisation
This subtheme includes the healthcare organisation's policies, such as the organisation of shifts and the allocation of human resources. Radiographers expressed the following views:
‘There are so many of us on shift, like them [nurses].’
They recognised that:
‘The organisation creates dynamics that hinder the collaboration.’
Theme 2. Cognitive dimension
The cognitive dimension subthemes relate to participants' knowledge of both nurses' and radiographers' scope of practice, which stipulate the roles and proficiencies required of their respective professional group. The cognitive theme is well represented by the following subtheme:
Knowledge of each other's scope of practice
This subtheme includes the knowledge of the activities that are performed respectively by nurses and radiographers. First, there is an attitude of defensiveness on the part of both radiographers and nurses, proven by a misunderstanding of each other's scope of practice. The radiographers stated:
‘What does it take to do an X-ray? Then maybe it's not just the time itself to perform the technique but the patient must be prepared …’
‘Sometimes I feel like they think I'm sitting and resting.’
Nurses also emphasised the tasks that came within their scope of practice:
‘… [it is within] our competencies to ensure the safety of the patient, the monitoring, the safety of the devices and of the medication administration … the responsibility of the radiographers is to produce an image.’
As one nurse stated, knowing each other's scope of practice could help understand how to better collaborate. The nurse said:
‘… maybe we don't even know their world, so for us it's just performing the X-ray or CT, but maybe they have a thousand other tasks to accomplish.’
Another nurse stated:
‘It often happens [that it's necessary] … to take several [images for] the same patient and together we collaborate to find the right position, to mobilise the patient properly, using the correct devices.’
Theme 3. Individual dimension
The individual dimension encompasses the subthemes that belong to the individual and personal sphere of the professionals, which may influence the work in acute care settings. The individual dimension includes:
Personal characteristics
This subtheme covers the specific character traits of individual health professionals, for example having patience when working with others, having good social skills and having common sense; the mindset, ethics and morals of an individual are also important. One nurse contributed the following:
‘There are also shifts where the radiographer is precise and calls us to know something about the patient and, if it is possible, she/he comes to take the patient directly from our room, if the exam is urgent.’
Interest in the work of health professional colleagues
This subtheme underlines the attention paid to the other health professional (nurse or radiographer) colleague. In general, the radiographers opinion was that nurses
‘Don't care what [the radiographer] is doing at that moment.’
Comments such as the following illustrate that the radiographers felt that their nurse colleague was not interested in their role and did not consider:
‘… what I am doing in my diagnostic area.’
Theme 4. Relational dimension
The relational dimension considers the relational subthemes that determine the relationships between nurses and radiographers in acute care settings. Within this dimension the following subthemes were identified:
Constant interaction
This subtheme includes recognition of the need for mutual support. Both professions recognise that ongoing support is an important aspect of working together in a team, whether regularly or on occasion:
‘There are cases in which it is difficult to lift one of our patients, perhaps with a lot of equipment. In those cases, it becomes essential to help the radiographer to put the X-ray device under the patient to facilitate his work. In this we always manage to collaborate […]’.
‘Ours are two professions that go together, there is no one job without the other… if the patient is unco-operative or allergic… [we] must work together… [do things in step] together… I [will] lend [my colleagues] a hand and vice versa.’
‘In the haemodynamic unit, there is a very strong collaboration. During emergencies we [radiographers]… [may do some of] the nurse's work and this brings us even closer … also because they actually become our trainers.’
‘There is a lot of collaboration with the radiographers who come to do the imaging on the ward, often several images have to be taken… we collaborate in finding the right positioning of the patient, taking into account all the equipment, so we are a point of reference for them and vice versa.’
‘A bit like what happens in angiography, you don't replace the nurse, but … I will go and get any [devices or supplies they may need] if they are busy … we help them in certain circumstances.’
‘In the case of general ICU, if it's me and a colleague, it's the radiographer …[who will tell] us how to help them … do the X-ray in the shortest possible time.’
This subtheme also includes routine actions and habits, regular interaction between colleagues with partly overlapping roles, the repetition of work tasks and years of experience for example:
‘Collaboration can be reached … in trauma teams, the work of radiographer and nurse becomes a bit of a hybrid, but … I have to know what the nurse is doing and … [vice versa]. In the haemodynamic unit, there is collaboration because there is knowledge of what the other is doing … in other areas there may not even be a willingness to know what the other has to do.’
‘Sometimes I connect the injector to the patient's venous access, I don't wait for the nurse … In the same way, I expect that maybe if I am doing complex diagnostic imaging that involves a lot of post-processing work, the nurse will help the patient off the table, without … having to interrupt my work. We can interchange on some activities, working together on the same diagnostics.’
‘I think it's the fact that in haemodynamic unit you work six hours with certain people to do certain procedures, so it's natural to know what the nurse does.’
Another facet of this subtheme encompasses an individual's empathy, their ability to anticipate the actions and needs of their counterpart in the team, the ability to empathise with other colleagues and to contribute to a favourable atmosphere in the workplace. One radiographer stated:
‘When working as part of a team, such as in haemodynamic unit or angiography, where radiographers and nurses work together on the same diagnostics for a long time, they take on parallel but sometimes overlapping roles and so certain things come naturally to you.’
Integration
This subtheme refers to nurses and radiographers feeling that they are working as part of a team. Nurses, in particular, recognised that this comes into play when the radiographer arrives in ICU and has to do more than one X-ray, with one nurse saying:
‘We are able to agree which one [should be done] first, which one [should be done] next.’
It also includes the need for effective communication, dialogue and a positive attitude to understanding the work of the other professional. The nurses' comments included:
‘There's harmony … as if we're [working as] one.’
Moreover, this subtheme implies trust. The radiographers, before integrating in the team, acknowledged that:
‘When I arrived on the ward at first I found, not exactly hostility, but almost a fear on the part of the nurses who did not know me. That is, if I took an extra step and I did something that wasn't strictly my remit as a radiographer… the nurse… [would snap and raise] her voice, because it seemed like she didn't trust me. Then, with time, I felt more integrated. They also saw that I was competent and so they were able to “delegate” their simpler tasks.’
Radiographers recognised that good collaboration with the other professionals they work with improves their own performance, with one commenting:
‘Sometimes, during some examination in the ICU ward, we need to modify the patient position to obtain the correct image. While I check the technical aspects, the nurse helps me with the non-technical things, for example how the patient is breathing. In this way, she/he helps me to work better and the patient in particular benefits from this.’
Flexibility
Collaboration between colleagues is also dependent on the subtheme ‘flexibility’, which depends on the ability of colleagues to reach agreement by overcoming any rigidity in undertaking their roles or misunderstanding of one another's areas of professional competence.
One of the radiographers effectively expressed the need for flexibility by describing the consequences when each professional rigidly sticks to their own scope of practice:
‘If the other acts as a soldier, thinking and doing only his/her own task, the relationship becomes a cage.’
Holistic perception of work
This subtheme suggests that one's job should be viewed not simply as a set of tasks listed in a job description that have to be followed rigidly, but instead taking them as an opportunity to consider the bigger picture. It emphasises the importance of going beyond one's own duties for the benefit of the patient, adopting a holistic view of the entire workflow involved in patient care. This approach fosters collaboration among professionals sharing a set of common goals, by encouraging them to pay attention to the entire process within which the patient is involved. As one radiographer commented:
‘… [it promotes] a relationship that has the good of the patient as its ultimate goal.’
Sharing and discussion
This subtheme includes shared training and having joint meetings. The radiographers, in particular, reported the need to schedule meetings together with nurses:
‘We both come into contact with the same patients in angiography, where the preparation of the patient before placing them on the couch affects both us and the nurses. We work together, we are both in contact with the same patient and each instructs them …in line with their remit.’
The need to plan debriefing sessions following specific cases that both sets of professionals had dealt with as a team was also underlined. One of the radiographers put forward the idea of adopting a work plan, suggesting that this would provide both groups of professionals with a forum to discuss the procedures in which they had been involved, to explore complementary perspectives and to learn from each other.
‘Moments of sharing and discussion are certainly useful because they allow you to enrich yourself and have new ideas. Often, we don't know what the nurses do in a particular ward and they don't know what we do.’
‘Knowing more than just the professional profile would also be appropriate, as it would be to understand the work plans of the two professions, the timings we have [to follow].’
Recommendations for the future improvements
Guided by the moderator and using a question-and-answer approach, focus group participants put forward some interesting recommendations to improve IPC, including:
Discussion
The purpose of the study was to investigate nurses' and radiographers' perception of IPC in acute care settings, by capturing the their views on the process of IPC between the two professions and identifying factors that support or hinder the implementation of IPC.
Analysis of focus group data led the researchers to identify four overarching themes, each of which could be further divided into a number of subthemes, in the context of IPC by nurses and radiographers working in acute care settings, namely:
As emerged from data analysis, the organisational dimension affects how both professional groups perceive IPC. In particular, it emerged from the focus groups that nurses and radiographers working in environments such as ER and OER (medical rooms and radiology) were physically separated from one another by physical barriers such as walls and corridors, making it difficult for them to interact and communicate with one another. By contrast, in an ICU, where health professionals work closely together within the same space, IPC is facilitated by the ease of having eye contact and effective communication.
Unfortunately, physical barriers, where identified, are difficult to remove. However, in future it might be worth investigating clinical environments that have a different physical arrangement of medical rooms and the radiology suite within the ER and OER. The constant flow and rapid turnover of patients in the ER can sometimes result in nurses paying less attention to preparing patients for a diagnostic radiological procedure, such as ensuring the removal of clothes with metal hooks and jewellery. In contrast, a radiographer in ER interacts with a patient only for the duration of an imaging procedure, which is a much a shorter period of time compared with ER nurses, who are in contact with the patient for the duration of their hospitalisation in the unit until they are discharged or transferred to another ward.
The physical barriers and constant flow and rapid turnover of patients in the ER, as cited by participants, may represent a point of misalignment between the two groups of health professionals, due to the lack of knowledge of their respective workloads at different time points during a shift. In addition to this shortfall of knowledge, a lack of effective communication may compound any frustration felt by health professionals.
The issue of ‘time’ was perceived by the majority of focus group participants as a negative factor, which was affected by the structure and policies of the healthcare organisation, since staff mix and human resources are not always at optimal levels to cope with service demand. This can cause disharmony between nurses and radiographers, frequently leading to misunderstandings, sometimes to the detriment of the patient (Will et al, 2019; Heip et al, 2022). Another important issue that emerged was the lack of knowledge of one another's scope of practice.
However, this lack of knowledge does not prevent implementation of IPC. Both groups of health professionals are bound by their codes of conduct (Federazione Nazionale Collegi Professionali Tecnici Sanitari di Radiologia Medica (FNCPTSRM), 2004; Federazione Nazionale Ordini delle Professioni Infermieristiche (FNOPI)2019) and generally work together as a team. However, study participants indicated that a deeper understanding of one another's roles might bring better integration and foster a healthier atmosphere in the workplace. Consequently, collaboration based on clear professional expectations (working and relational) would contribute to improving the quality of IPC.
In addition, it is important to consider factors such as an individual nurse's or radiographer's personality characteristics, common sense and technical skills. Both professionals groups are governed by their own codes of conduct (FNCPTSRM, 2004; FNOPI, 2019), which promote collaborative interpersonal relationships, as well as requiring proficiency in clinical and technical skills that, at times, need to be integrated with those of other health professionals with whom they are working to deliver optimal patient care. In this context, ‘soft skills’ have increasingly become more crucial for professionals to enable them to perform their role to a high standard (Gnecco et al, 2023; Lamberti et al, 2023).
Of note is that communication skills were unequivocally identified as the basis of good IPC across all four focus groups, although the modes of communication may vary depending on the working environment. It is important to point out that, when healthcare workers have adequate time to carry out their roles, both verbal and non-verbal communication are effective for sharing crucial information (Goulart et al, 2016), while a lack of time owing to heavy workloads has been shown to lead to ineffective communication, which can be a barrier to communication. Effective communication may promote respect between colleagues and increase the chance of resolving differences in viewpoints/professional opinion, thus making decision-making easier (Muusse et al, 2023). In a study by Mudadi et al (2024), radiographers identified poor communication as one of the top three barriers to IPC: when health professionals fail to communicate effectively, patient safety can be compromised due to reasons such as critical information being omitted, information being misinterpreted and failure to recognise changes in patient status.
Furthermore, effective communication in combination with a manageable workload may enhance the quality of care and encourage the adoption of a holistic approach. Consequently, both nurses and radiographers may work more collaboratively for the benefit of the patient. While the nurse is responsible for patient care and safety throughout the patient journey, the radiographer's role is to undertake a rapid procedure, positioning the patient correctly and using optimal techniques to ensure that precise diagnostic imaging is obtained. This illustrates the close relationship between the roles and the expertise of these two professionals areas over the course of a diagnostic procedure. And it is the ongoing dialogue between the two health professionals and their willingness to be proactive and dedicated to the patient that make this possible. It is clear that improving the quality of communication between nurses and radiographers is crucial.
The question-and-answer format guided by a moderator resulted in focus groups participants putting forward some interesting recommendations for improving IPC, as presented in the Results section. These suggestions echo the recommendations that can be found in the literature. In particular, the idea of scheduling debriefing sessions to understand one another's point of view is similar to that described by Baxter and Brumfitt (2008): they highlighted that this leads to ‘greater patient safety and mutual support’. Also of note is that, in a study by Mudadi et al (2024), radiographers identified the lack of a clearly stated, shared and measurable purpose as an important barrier to IPC. This emphasises the importance of implementing programmes that encourage a shared vision for different members of the team.
A similar concept was outlined in Reeves et al (2017), who reported clinical audits or debriefing sessions as a supportive strategy for IPC implementation. Another interesting recommendation is that of shadowing colleagues in different clinical environments. Educational programmes, including curricula and in-service training, are also effective in creating and strengthening interprofessional competencies (Vaseghi et al, 2022). For example, there are benefits in providing students on clinical placement with the opportunity to shadow other professional groups, as would working together in a simulated environment at university. Having joint lectures would be equally fruitful.
Limitations of the study
This study has a number limitations. The aim was to recruit health professionals from different acute care settings, but not all settings were represented equally. This was partly due to the stringent inclusion criteria, such recruiting only healthcare workers with 3–15 of years of experience.
In addition, in order to foster a relaxed atmosphere and promote participation, the focus groups each consisted of the same professional group. Although this strategy may have had a positive impact by allowing participants to freely express their thoughts and feelings, it may also have led to bias. In any future research, it may be beneficial to have mixed groups of nurses and radiographers, and to analyse new themes, should any emerge.
Another limitation could be the exclusion of nurses and radiographers who are not fluent in Italian because this may have brought some additional viewpoints to the focus group discussions.
Conclusion
This study has highlighted the multifaceted nature of IPC between nurses and radiographers working in acute care settings, emphasising the critical role of organisational, cognitive, individual and relational dimensions. By analysing the perceptions and experiences of these health professionals, the authors identified several key factors that may facilitate or hinder effective IPC.
Organisational aspects such as the physical environment, workplace/organisational characteristics and the healthcare organisation's policies significantly influence the collaborative dynamics between nurses and radiographers. Cognitive factors, including mutual knowledge of one another's roles and competencies, are essential for fostering a shared understanding and respect for the other's professional contribution.
Characteristics, such as individual behaviours, patience and having an interest in the work of professional colleagues, also play a vital role in IPC. These factors, although not as easy to adapt and change, can be addressed through targeted training and professional development initiatives aimed at enhancing soft skills and promoting a culture of empathy and mutual respect.
Relational dimensions, encompassing ongoing interaction, integration, flexibility, holistic perception of work, sharing knowledge and engaging in discussion, are crucial for building strong collaborative relationships. Effective communication and trust are fundamental to these interactions, enabling health professionals to work together seamlessly for the benefit of the patient.
The recommendations for future improvements, including joint training sessions, audit-like meeting, and shadowing a colleague, align with the literature and offer practical steps to enhancing IPC. Implementing these strategies can lead to better integration of nurses and radiographers, ultimately improving patient outcomes and the overall efficiency of care delivery in acute care settings.