
Bronchiolitis obliterans syndrome (BOS) following allogenic haematopoietic stem cell transplant (HSCT) is considered the manifestation of chronic graft versus host disease (cGvHD) in the lung (Del Fante and Perotti, 2017). BOS affects about 14% of patients with cGvHD, mainly in the first 2 years following transplant (Au et al, 2011) and is one of the most frequent late-onset non-infectious pulmonary complications following HSCT (Del Fante and Perotti, 2017). BOS is characterised by progressive airflow obstruction in the absence of respiratory infection, which significantly affects patients' quality of life (Yoshihara et al, 2007; Amin et al, 2015). In the early stages of pulmonary cGvHD, although some patients may be asymptomatic the majority often present with non-specific symptoms such as mild dyspnoea on exertion or a dry, non-productive cough (Hildebandt et al, 2011). It was suggested by Efrati et al (2008) that functional and structural changes occur earlier than the manifestation of clinical symptoms and subsequent physical impairment. Pulmonary complications occurring following allogeneic HSCT substantially contribute to morbidity and late mortality in patients presenting with impaired lung function (Palmer, 2016).
Despite advances in assessment, diagnosis and treatment, the clinical prognosis for patients with pulmonary manifestations of cGvHD remains poor. In recent years the revised National Institutes of Health (NIH) consensus of diagnostic criteria for lung cGvHD or BOS has facilitated standardisation in diagnosis, assessment and management of this condition (Jagasia et al, 2015). BOS is a devastating complication of transplant, occurring in 3% to 6% of all transplant patients with prevalence in cGvHD increasing up to 14% (Palmer, 2016). Essentially, detection and diagnosis rely on the identification of obstructive decline in pulmonary function in the absence of alternative aetiologies. Hildebrandt et al (2011) suggested that early detection of obliterative airway disease may be achievable through longitudinal comparison of values for forced expiratory volume in 1 second (FEV1), when there is still a possibility that the damage may be reversed. The NIH consensus project on clinical trials in chronic GvHD Ancillary Therapy and Supportive Care Working Group (Carpenter et al, 2015), and German/Austrian/Swiss Consensus Conference On Clinical Practice In Chronic GvHD (Hildebrandt et al, 2011), recommend that lung function spirometry should be assessed at 3-monthly intervals for 2 years following HSCT via pulmonary function testing (PFT). Although PFT are recommended by the NIH and the German/Austrian/Swiss consensus group this recommendation was followed by fewer than 50% of transplant centres replying to the consensus group's survey (Hildebrandt et al, 2011). The reason for the discrepancy is unknown; possible explanations could be related to cost and patient compliance (Palmer, 2016).
Cheng et al (2016) compared the FEV6 (forced expiratory volume in 6 seconds) and FEV1 results of cGvHD patients (n=437) at day 0, day 80 and 1 year following HSCT. These results displayed a linear correlation at all time points, suggesting that handheld spirometry may be used as a screening tool for sub-clinical changes in this cohort of patients, potentially reducing the need for regular, lengthy and costly PFTs.
The authors' unit therefore devised a pilot study to establish whether a similar relationship could be found between FEV1 via PFT and peak expiratory flow (PEF) via peak flow handheld spirometry in cGvHD patients receiving extracorporeal photopheresis (ECP).
Methods
Between 1 November 2016 and 31 December 2017, cGvHD patients attending for ECP were supplied with a handheld peak flow meter (Mini-Wright, Clement Clarke), educated on how to accurately perform peak flow readings and asked to record their results daily. However, following a compliance review in February 2017, patients were asked to record results a minimum of once weekly. In line with NIH 2015 consensus recommendations (Carpenter et al, 2015), PFTs continued to be recorded at 3-month intervals, alongside simultaneous handheld peak flow meter data collection. After 12 months all data from PFT and peak flows meters were reviewed and analysed. Individual expected peak flow readings were calculated for each patient using the peak flow meter chart supplied, which was adapted by the manufacturer from Nunn and Greg (1989). The actual readings were collected along with the percentage predicted for both handheld as well as full spirometry testing.
Fifty patients were originally included in the pilot study. (See Table 1 for demographics) Peak flow results from handheld devices could be compared only with the PFT results at patient reviews that were at 3, 6, 9 and 12 months after starting the pilot if they were recorded within 2 days of each other.
| Male; n | 16 | |
| Female; n | 3 | |
| Age; range | 18–71 years | |
| Time of onset of GvHD after transplant; median (range) | 3 (1–34) months | |
| Underlying diagnosis | Acute leukaemia/myelodysplastic syndrome | 9 |
| Lymphoma | 1 | |
| Chronic leukaemia | 4 | |
| Myeloma | 1 | |
| Other | 4 | |
| Type of transplant; n | Unrelated donor | 9 |
| Sibling/related donor | 5 | |
| Donor lymphocyte infusion (DLI) | 2 | |
| Unknown | 2 | |
| GvHD site; n | Skin | 15 |
| Joints | 3 | |
| Oral | 7 | |
| Eyes | 3 | |
| Gastrointestinal | 3 | |
| Liver | 5 | |
GvHD: graft versus host disease
Results
Table 2 shows the results of the analysis for correlation between the different respiratory tests, and the data for month 3, month 6 and month 9 are plotted in Figure 1. At month 3, 19 patients had PFT and handheld meter results that could be compared showing a significant positive correlation in both observed and predicted PEF versus FEV 1.
| Time point | Number of patients | Observed FEV1 versus PEF | % predicted FEV1 versus % predicted PEF | ||
|---|---|---|---|---|---|
| Correlation coefficient | 95% confidence interval | Correlation coefficient | 95% confidence interval | ||
| Month 3 | 19 | r=0.74, p=0.0003 | 0.43-0.89 | r=0.47, p=0.0435 | 0.017–0.76 |
| Month 6 | 9 | r=0.89, p=0.0013 | 0.55-0.98 | r=0.55, p=0.1239 | 0.18–0.89 |
| Month 9 | 9 | r=0.84, p=0.0743 | -0.16-0.99 | r=0.67, p=0.2199 | -0.52–0.98 |
| Month 12 | 3 | r=0.23, p=0.8524 | r=0.35, p=0.7742 | ||
FEV1: forced expiratory volume in 1 second (measured through pulmonary function testing); PEF: peak expiratory flow (measured with handheld peak flow meter)
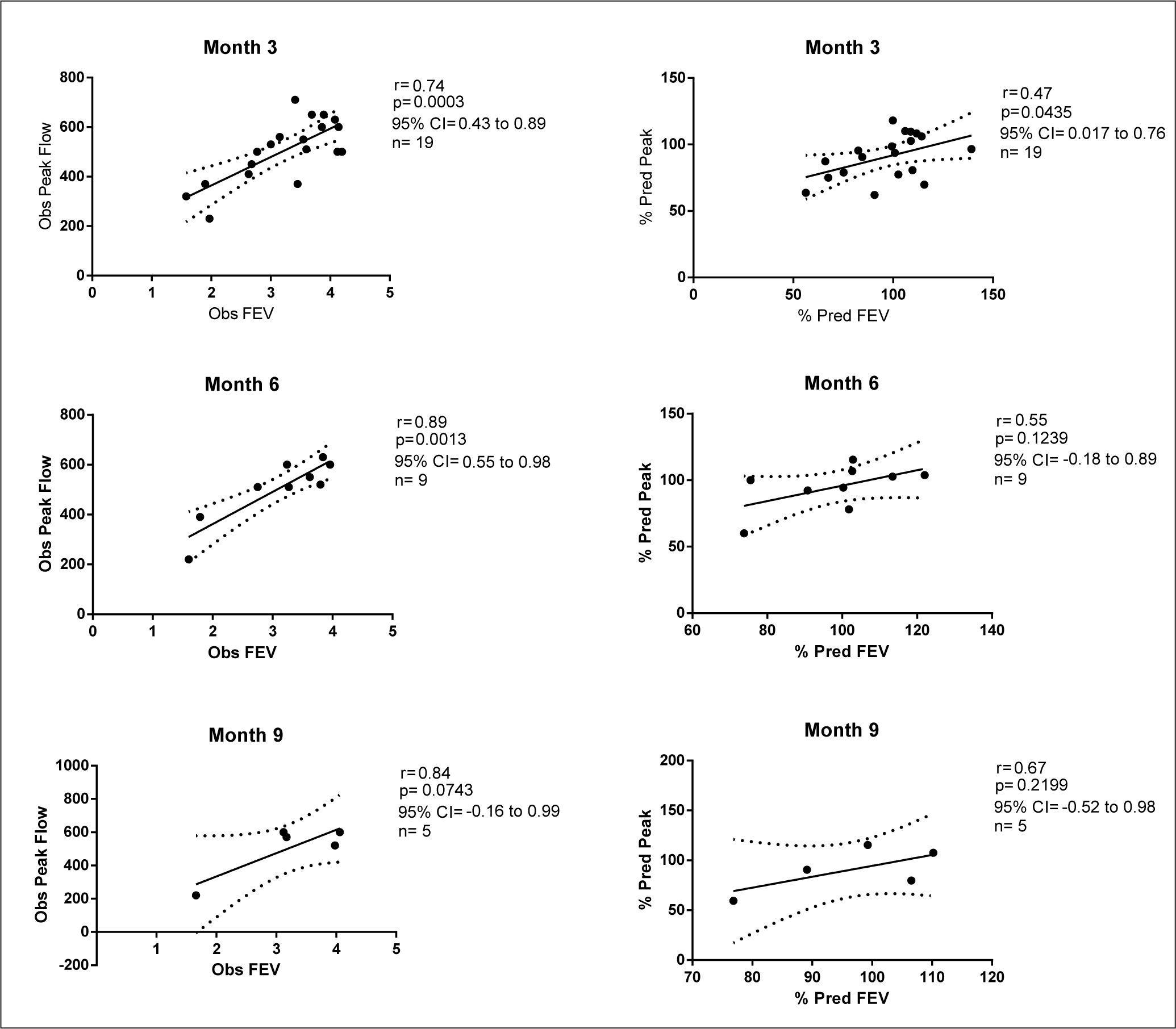
At month 6 there were 9 patients that had PFT and hand held meter results that could be compared, showing a positive correlation in both observed and predicted PEF versus FEV1 that was significant in the observed values. At this point, 11 patients were lost from the pilot study; there were 2 deaths, 7 patients' study data were incomplete or not returned, 1 patient suffered repeated chest infections so was unable to complete the PFT and 1 patient achieved a complete response to ECP and completed treatment.
At month 9 there were 5 patients that had PFT and handheld meter results that could be compared, showing a positive correlation in both observed and predicted PEF versus FEV1, although neither of these correlations were statistically significant. At this point 4 more patients were lost from the pilot study; 1 patient completed ECP, 1 patient suffered repeated chest infection so was unable to complete the PFT, and the other 2 patients were scheduled to have PFT outside the agreed review date.
At month 12, 3 patients had PFT and handheld meter results that could be compared; however, there was no correlation between PEF and FEV1 values in either observed or predicted values. The final 2 patients were scheduled to have PFT outside of the agreed review date.
Discussion
This pilot study illustrated that the monitoring of handheld peak flow meter readings has the potential to become an acceptable method of monitoring lung function longitudinally in patients with cGvHD. However, there are some questions that need to be addressed.
With regard to the handheld peak flow meter, how soon after transplant should patients start recording readings and how often these should be taken? Ideally, lung function should be tested before transplant to get a baseline, then as soon after transplant as possible to determine whether the transplant has had any effect on respiratory function and any subsequent drops can be noticed quickly. In this pilot study, for a significant number of patients requesting recordings every day resulted in poor compliance (62% of patients did not participate from the start) and requesting a minimum of once a week increased compliance only slightly (a further 36% did not comply for the full 12 months). Therefore, some work would need to be done to address compliance issues. If handheld peak flow is introduced early after transplant it could become second nature for the patient—in a similar way to the regular blood glucose testing involved for patients with diabetes—which could improve overall compliance. There is also scope to investigate other methods of monitoring FEV1 and forced vital capacity (FVC) to see whether a different method could improve compliance.
This pilot study consisted of a small patient population, which is likely to be the reason for the results at month 9 and 12 being less encouraging than at months 3 and 6. Another issue caused by the small number of participants is that none of them had been diagnosed with lung involvement on starting ECP. Patients with pulmonary complications were not excluded from the study because all those attending the unit were encouraged to participate. The results were monitored for each patient over the 12-month period because a 10% drop could indicate the development of a pulmonary complication. The results for each participant were reviewed and no sign of a clinically significant drop of 10% was noted in either the PFT spirometry or handheld meter results. Future studies would need to include patients with pulmonary complications to ascertain whether the correlation is still present between the PFT spirometry and handheld meter when changes are observed.
The authors of this pilot study are not suggesting replacing PFT with handheld peak flow monitoring, because more research is needed. However, many regional areas have limited access or no access to PFT, so handheld devices could be an easy, low-cost method of monitoring lung function longitudinally within this patient population. If the correlation between FEV1 and PEF results remains robust when observed in a population with existing or newly developed pulmonary complications, then there could be scope for using PFT. Regular PEF monitoring should be used as an addition to PFTs every 3 months to pick up changes earlier, perhaps when symptoms first start, to allow prompt spirometry measurements and clinical assessment A handheld peak flow meter costs on average £12 for each individual named patient and can be continually used until it needs replacing due to damage, whereas PFT costs on average £70 every time the patient has a test. For centres that are currently unable to offer respiratory function monitoring, the low cost of a handheld meter would provide them with this option, improving patient care. In addition, PEF monitoring will identify worsening of respiratory function due to infection and allow earlier intervention, which would potentially have both economic and, more importantly, quality-of-life benefits for the patients.
Another advantage of using handheld devices to assess peak flow is that it can be a way to empower patients. Allowing them to monitor their own peak flow and report any changes between treatment visits may make them feel more in control of their treatment. This may also assist in identifying reductions in lung function early so that appropriate treatment can be started as soon as possible rather than having to wait for it to be identified at a scheduled 3-month review.
There is a separate debate regarding which value is the best indicator of lung function decline in patients with GvHD. The question is whether spirometry alone is a sufficient indicator of decline, or whether using TLCO (transfer factor of the lung for carbon monoxide) as an indicator would improve accuracy. It could be suggested that peak expiratory flow results from a handheld peak flow meter may not be as accurate as FEV1, FVC and FEV1/FVC ratio as recorded by a PFT for the detection of lung function decline—although the correlation seen in this pilot study suggests that they provide similar results. It could also be suggested that TLCO in addition to FEV1 would further increase the chance of detecting lung function decline at an early stage; however, this requires further investigation.
Conclusion
Due to the results of this pilot study showing a significant correlation between the results from PFTs and handheld devices, the authors' unit now actively encourages patients to record regular peak flow readings, allowing the early identification of subclinical drops in respiratory function. In the absence of an alternative aetiology, urgent PFT may then be scheduled to further analyse the patient's lung function. Future results will continue to be compared, assessing the ability of peak flow readings to accurately assess any reduction in lung function, assisting in the timely detection of early lung cGvHD or BOS.
The take-home message for nurses working with this group of patients is to monitor them for early lung cGvHD or BOS and, because the results seen from this pilot study show significant correlation, to recommend that nurses start recording handheld respiratory function results and empower patients to take some control of their treatment plan as well.