

Nurses and midwives in leadership positions have been recognised as essential for global health promotion, disease prevention, and achieving goals related to health and social care (Salvage and White, 2020; Klopper et al, 2020; Rumsey et al, 2022). To achieve health for all, nurses and midwives need to be provided with leadership development opportunities so they can be strategically positioned to respond to reform and positively transform health care (Adcock et al, 2022; James and Bennett, 2020).
Effective leadership is essential for building a sense of safety and improving performance and work productivity in healthcare teams (Labrague, 2024), particularly in times of crisis such as the COVID-19 pandemic (Ahern and Loh, 2021). Yet, mounting evidence has shown that health systems across the world, including in the UK, have grappled with the realities of postCOVID financial scarcity (Saghafian et al, 2022; Kentikelenis and Stubbs, 2022; Koumpias et al, 2022). This may affect longstanding health and care staff shortages (Hamouche, 2023), and the ability of systems to proactively invest in transformation and respond to increased population mental health needs (Toulany et al, 2022; Wong et al, 2023). This is despite expectations that all health professionals will continue to improve healthcare services, to provide high-quality care with a focus on patient safety (NHS England, 2019). Therefore, investment in nurse and midwife leadership development is vital if we are to continue to expand capability and capacity to positively influence health within these challenging contexts (Bond et al, 2022).
Introduction
The COVID-19 pandemic exposed healthcare teams to new challenges, requiring rapid changes to their leadership and operational practices (Pandit, 2021). There has been an increased reliance on digital platforms for care delivery, increased diversity within the workforce due to international recruitment, and pressures on clinical staff such that more support is needed to retain the existing workforce (Desveaux et al, 2019; McKee et al, 2021; Junaid et al, 2022; Naghavi et al, 2024). These ongoing changes will increasingly impact on the fundamental ways health and care is delivered and, given that workforce challenges are likely to continue, significant transformational change is needed in education, health and care service delivery design, as well as models of care provision (Ustgorul, 2022).
Therefore, there is a need to ensure effective nursing and midwifery leadership at executive levels and that a nursing presence is obvious within future policy agendas. As such, the development of effective nursing and midwifery leaders who are prepared and primed to respond to these challenges must continue.
In terms of developing effective healthcare leaders, there has been a longstanding fascination with the personality traits and behaviours associated with leadership (West et al, 2015), as well as with the competencies specific to leadership, such as technical, conceptual and interpersonal skills. Transformational leadership theory (Bass, 1990; 1999) has dominated the research landscape. The goal of most leadership development programmes is to transform ‘followers to leaders’ and it is this idea that underpins the ‘healthcare leadership model’ and provides the basis in the UK for the national strategy for leadership development (NHS Leadership Academy, 2013). However, the application of transformative ‘learning’ theory (Mezirow, 2000) has also proven effective in enabling nurses and midwives to develop increased self-efficacy in relation to perceptions of the self as a capable and competent leader (Bond et al, 2023), with potential to have a much wider impact regarding improving patient care, and, by inference, perceptions of quality.
In the context of the rapidly evolving healthcare landscape, shifting demographics (Naghavi et al, 2024) and changes in leadership roles over time (Vasset et al, 2023), it is unclear what additional skills and attributes nurse and midwife leaders are likely to require in future. Knowing this is important to enable those delivering leadership development programmes to plan appropriately, to ensure that their programmes are designed and adjusted to what is needed within the complex health and care landscape that nurses and midwives are currently working in (Pandit, 2021).
Given the rapidity of change in the UK, for example the NHS reform agenda and broader workforce plans, it is essential to gain insight into what the perceived needs might be, in terms of leadership requirements in the future. Thus, the authors took an exploratory approach to gain understanding from those working in the nursing and midwifery professions.
Ethical considerations
Formal ethical approval was not required because this was the consultation phase of a wider service evaluation, focusing on the future of nursing and midwifery leadership. Data were collected using a questionnaire, which was publicised via The Florence Nightingale Foundation's (FNF) website. The consenting process involved informing participants that names and contact details would be collected and that the feedback would be anonymised in data analysis and dissemination activities. As such, implicit informed consent was obtained from all participants.
Data were stored on a secure cloud server, accessible only to FNF employees, and kept in accordance with European Union General Data Protection Regulations.
Method
Purpose
To identify the skills and knowledge that, in the view of the respondents, future nurse and midwife leaders might require in the next 6 years.
Data collection
An online semi-structured questionnaire was designed to explore perspectives on the future requirements for nurse and midwife leaders. It was made available on the FNF's public website and was live between 27 September 2023 and 31 October 2023. Both quantitative and qualitative date were collected. This article explores participants’ responses to the qualitative element of the questionnaire, in which they were asked to reflect on the following question:
- Imagine the health and care system in 2030, what different and additional leadership skills and attributes will nurses and midwives need?
A total of 101 people completed the questionnaire. The majority of respondents were female (72.2%), registered health professionals (86.1%), and aged between 45 years and 64 years (57.3%). Table 1 provides an overview of demographic information.
| Questions/information requested | n=101 | % (1DP) |
|---|---|---|
| What is your relationship with Florence Nightingale Foundation? | ||
| None | 4 | 3.9 |
| Alumni | 46 | 45.5 |
| Alumni champion | 3 | 2.9 |
| Applicant | 2 | 1.9 |
| Donor | – | – |
| Academy associate | 4 | 3.9 |
| FNF team member | 1 | 0.9 |
| Leadership programme participant | 9 | 8.9 |
| Member (paid subscriber) | 2 | 1.9 |
| Mentor | 3 | 2.9 |
| Sponsor | 8 | 7.9 |
| Supporter | 18 | 17.8 |
| Trustee | – | – |
| Person receiving health/care services | 3 | 2.9 |
| Person caring for someone receiving health/care services | 5 | 4.9 |
| Other | 12 | 11.8 |
| Do you have a health professional registration? | ||
| Yes | 87 | 86.1 |
| No | 9 | 8.9 |
| No response | 7 | 6.9 |
| NHS pay band/grade or equivalent | ||
| 4 | 1 | 0.9 |
| 5 | 3 | 2.9 |
| 6 | 17 | 16.8 |
| 7 | 8 | 7.9 |
| 8a | 12 | 11.8 |
| 8b | 8 | 7.9 |
| 8c | 10 | 9.9 |
| 8d | 5 | 4.9 |
| 9 | 9 | 8.9 |
| Very senior manager | 5 | 4.9 |
| Other | 13 | 12.8 |
| No response | 11 | 10.8 |
| Work nation | ||
| England | 83 | 82.1 |
| Scotland | 8 | 7.9 |
| Northern Ireland | 4 | 3.9 |
| Wales | 3 | 2.9 |
| Gender | ||
| Female | 73 | 72.2 |
| Male | 9 | 8.9 |
| No response | 17 | 16.8 |
| Prefer not to say | 1 | 0.9 |
| Age group (years) | ||
| 25–34 | 7 | 6.9 |
| 35–44 | 18 | 17.8 |
| 45–54 | 37 | 36.6 |
| 55–64 | 21 | 20.7 |
| 65 and over | 5 | 4.9 |
| No response | 14 | 13.8 |
| Ethnicity | ||
| White - English/Welsh/Scottish/Northern Irish | 50 | 49 |
| White Irish | 5 | 4.9 |
| White Other | 5 | 4.9 |
| Black African | 8 | 7.9 |
| Black Caribbean | 2 | 1.9 |
| Asian Indian | 4 | 3.9 |
| Asian Filipina/Filipino | 2 | 1.9 |
| Asian Pakistani | 1 | 0.9 |
| Asian Other | 2 | 1.9 |
| Arab | 1 | 0.9 |
| Mixed White and Black Caribbean | 2 | 1.9 |
| Mixed White and Black African | 1 | 0.9 |
| Mixed White and Asian | 2 | 1.9 |
| Mixed other | 1 | 0.9 |
| Prefer not to say | 2 | 1.9 |
| No response | 13 | 12.8 |
| Nationality | ||
| British | 55 | 54.4 |
| Irish | 7 | 6.9 |
| Scottish | 4 | 3.9 |
| English | 12 | 11.8 |
| Nigerian | 2 | 1.9 |
| Polish | 1 | 0.9 |
| Qatari | 1 | 0.9 |
| Romanian | 1 | 0.9 |
| Spanish | 1 | 0.9 |
| American | 2 | 1.9 |
| No response | 15 | 14.8 |
Qualitative data analysis
Data were extracted and transferred to a Microsoft Word document. The information was analysed using a content analysis approach, as described by Elo and Kyngäs (2008). First, the data were checked to ensure that no individual and/or organisation had been referred to by name; no direct reference to any individual or organisation was noted. While extracting the data, any recurring words, or segments of words, were noted.
The analyst then familiarised themselves with the corpus of data, noting the frequency of recurring words, and any collocated words or sentences that appeared around key words (key words were noted during the extraction phase, when lifting of raw data from the webform). The second stage of the analysis involved recording the various subcategories identified within the data. Subcategories were then grouped together to form overarching categories. Finally, taking a systematic, iterative approach (Merriam and Tisdell, 2015) enabled the core category of ‘Nursing & Midwifery Leadership’ to be identified (see Figure 1).
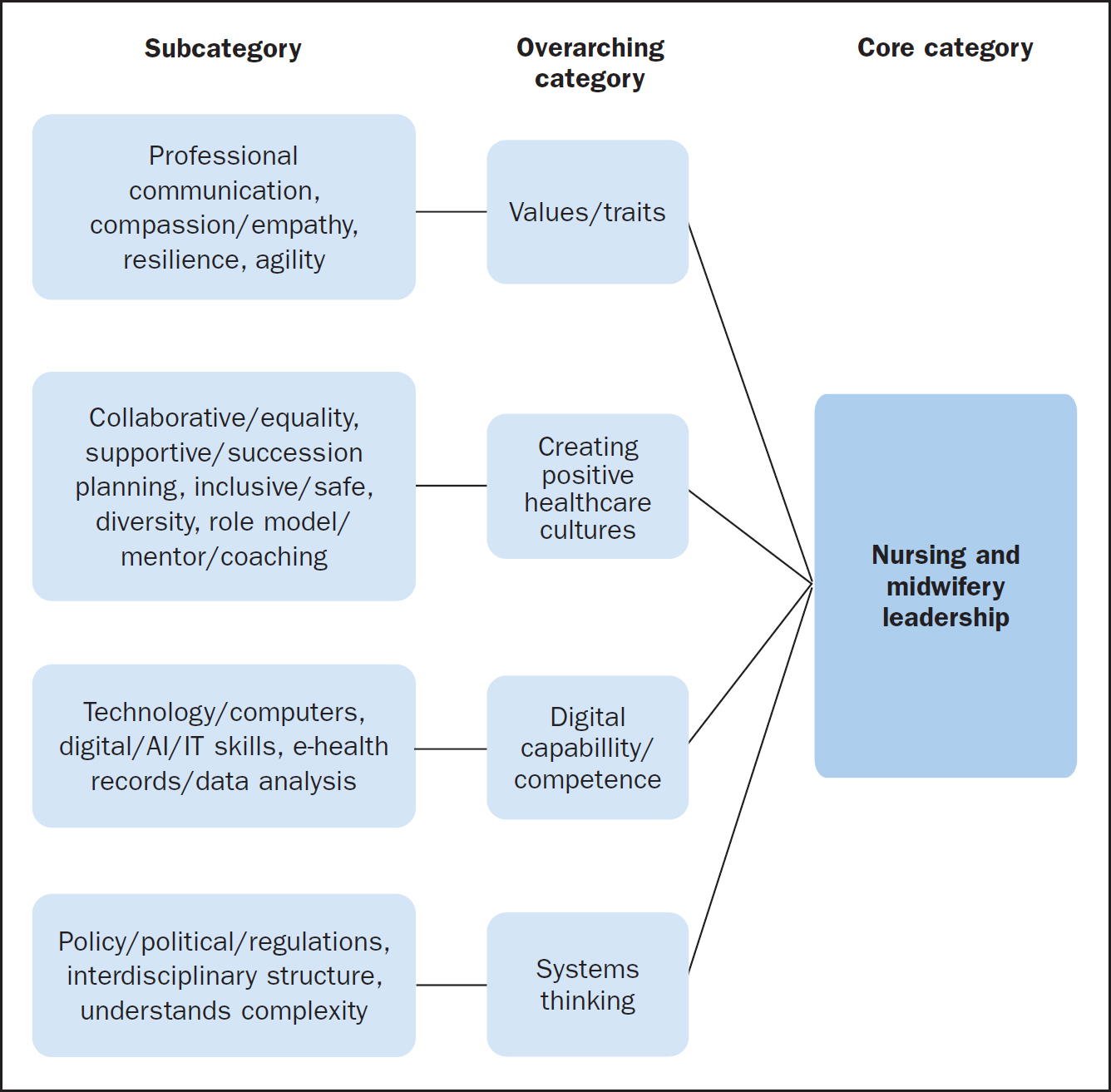
Findings
The findings demonstrated that the comments simultaneously reflected respondents’ understanding of how they considered the nursing and midwifery professions now, and in relation to the question that was asked. Four overarching categories were identified:
- Values/traits
- Creating positive healthcare cultures
- Digital capability/competence and
- Systems thinking.
Examples from the data have been presented to illustrate the type(s) of comments made by survey respondents. In places, there were notable links between the overarching categories. Where applicable, this has been signposted within the following narrative account.
Values/traits
Professionalism
First, it was noted that comments related to the values and traits that respondents perceived might be required by future leaders or those that might need to be developed. This included, for example, continuing to uphold professionalism and the standards integral to the professions, eg by nurses and midwives being models of integrity and leadership for others to aspire to, as outlined in the Nursing and Midwifery Council (NMC) (2018)Code. In terms of the future of the nursing and midwifery professions, the comments suggested that nurses and midwives need to develop an active and participatory role in making and influencing decisions about the way the professions might continue to develop. Respondents referred to this as having a professional voice, for example.
‘… enactment of professional values that we hold dear and underpin nurses’ and midwives’ service to society.’
‘Stronger professional voice.’
‘Developing political voice – stop being “done to”.’
Communication
Communication skills were considered to be important, with respondents’ comments referring to the ability to engage with both patients and staff. Communication was also noted with regard to the hybrid approaches to working that emerged during and since the COVID-19 pandemic, and in terms of future technological advancement. Clearly, this subcategory (communication) was linked to the overarching category of ‘values/traits’ in terms of comments related to developing technological skills and using technology to communicate.
‘As always, good communication is essential.’
‘They will need strong communication skills to engage with patients and their families in a rapidly changing healthcare landscape.’
‘Much more tech skills… working more remotely so clear leadership, communication and vision.’
‘Embracing new technology to communicate.’
Compassion and empathy
It was clear that within the corpus there was general consensus that future nursing and midwifery leaders would need to hold values that were aligned more with kindness, compassion and empathy. However, the language was superficial and there was little by way of attempts to elaborate on what these value/traits might look like in practice.
‘Always considered as kind, compassionate.’
‘More compassion.’
‘Compassionate and inclusive leadership.’
‘All those who deliver services to provide high quality evidence-based care in a kind, compassionate way.’
Although the importance of the overarching category ‘digital capability/competence’ became evident throughout the process of analysis, it was clear that respondents placed equal importance on personal values and humanistic approaches, which they considered would continue to be key in future nursing and midwifery leadership:
‘Leading with empathy.’
‘Empathy will still be important as well as IT skills.’
‘Design thinking – human-centred approach to problem-solving that encourages empathy and collaboration.’
‘Nursing remains a core skill that cannot be fundamentally delivered by technology alone.’
Resilience
Respondents highlighted the need for future leaders to have personal resilience to address the challenges that might arise in healthcare environments in the future. These comments were made with reference to previous challenges, such as the COVID-19 pandemic, as well as ongoing issues such as staffing shortages and how these impact patient care. A few comments noted that self-care would be an important consideration to reduce burnout and improve wellbeing and/or resilience. However, respondents did not explain what they meant by the word ‘challenges’ in the context of leadership.
‘Adaptive, resilient, intuitive, diverse and responsive to patient and staffing needs.’
‘Increasing staff morale with a positive attitude and encouraging emotional resilience.’
‘More resilience to be dealing with challenges.’
‘Nursing leaders should prioritise their own self-care and resilience to prevent burnout and maintain their wellbeing, which in turn allows them to lead effectively.’
Agility
Some comments mentioned the need for future nursing and midwifery leaders to have the ability to respond to the abovecited challenges, eg to be agile and adaptable, and able to prepare to address any challenges; however, these comments were few.
Creating positive healthcare cultures
Respondents noted the need to address the changing landscape of health care in future, with comments saying that leaders would need to ensure positive, psychologically safe, working environments. This type of comment was made relative to the overarching category ‘values/traits’; for example, emotional intelligence was noted as a characteristic that would enable future leaders to manage and support teams effectively:
‘Nursing leaders should possess strong emotional intelligence to foster a positive work environment, manage conflicts, and provide support to their teams during stressful situations.’
‘… how to work together and how to communicate to enable psychological safe working environments.’
Collaborative and supportive
In the subcategory ‘collaborative/equality’, comments stressed the idea that hierarchical structures should be reduced to enable future leaders to work in a collaborative way. One comment noted the need for future leadership development programmes to be multidisciplinary, with the suggestion that this would enable collaborative leadership and the benefits of this to be realised: Other comments supported this.
‘Stepping away from authority figures and making sure those in charge approach leadership collaboratively.’
‘…human-centred approach to problem-solving that encourages empathy and collaboration.’
‘Awareness of hierarchy but the ability to treat all as equal.’
The idea of working collaboratively, in partnership with other professionals, was identified as synonymous with nursing and midwifery practice as currently practised. There were suggestions that this would be an important aspect of the working environment in 2030.
‘Work collaboratively across organisations.’
‘We are known for our collaborative working and this will be at the forefront of working in 2030.’
‘Collaboration with various healthcare professionals, such as physicians, pharmacists, and therapists, is essential for holistic patient care. Future nursing leaders should excel in teamwork and interdisciplinary communication.’
In the working environment of the future, the view was that the idea of leaders working collaboratively would be extended from the immediate team to the wider multidisciplinary network. However, there were also comments on the need for future leaders to create a positive working environment both within the team and across various organisations. The content of these comments centred on ‘support’ and ‘supporting’ team members, creating positive working environments. Support was mentioned with regard to backing other people's ideas, enabling career development, and staff wellbeing. Respondents gave consideration to nurses and midwives at all levels.
‘Leaders will need to find and encourage and support the innovators within their teams and champion ideas.’
‘Open to new ideas, empower others, see opportunities, value and embrace difference, be open to new ideas, and spot and support talent.’
‘Leaders need support in the moral injury that inevitably comes from working in the NHS.’
‘Leadership needs to value and support talent at the bottom.’
‘Career development and support for the midwives, maternity support workers and all those who deliver services to provide high quality evidence-based care in a kind compassionate way.’
With reference to the working environments of the future, comments focused on the need for leaders to be nurturing and empowering, drawing on their underpinning values and traits in order to deliver high-quality patient care. A subcategory within ‘creating positive healthcare cultures’ acknowledged the need to grow leaders’ talent within the immediate working environment. For example, several short/segments used the phrases ‘plan ahead’ and/or ‘succession planning’.
Inclusive and diverse
The topic of patient safety was also touched upon, stressing the need to create safe environments in the future. Equally, some respondents cited the need to establish conditions within which staff would feel psychologically safe to escalate concerns about patient care:
‘Culturally safe places.’
‘…enable psychologically safe working environments…’
‘Creating spaces for psychological safety, if nurses fear to escalate concerns due to judgement, that impacts patient care.’
‘Be able to stand up and say no, if they feel the route is unsafe for their staff and/or the people in their care.’
Comments on safety cultures were related to the concept of co-production and the idea that future leaders would create environments within which care would be undertaken collaboratively and include the patient voice, in relation to both co-production and advocacy.
‘Ability to influence safety cultures. Ability to coproduce care with people receiving it.’
‘Ensure the patient voice is brought into the solution thinking.’
‘Advocating for patients’ rights, safety, and well-being remains a core nursing skill. Future leaders should be strong patient advocates, working to ensure the best care possible.’
Comments in this category noted the need to provide care to diverse populations, as well as the requirement that leaders be equipped to recognise and respond to diversity:
‘Should be able to lead within different and diverse communities; should be able to connect with diverse communities.’
‘Cultural competence for diverse patient populations, and the ability to lead interdisciplinary teams to provide holistic care.’
‘…diverse and responsive to patient and staffing needs.’
Role modelling and coaching
The final set of subcategories within this overarching category focused on leaders as role models, coaches and mentors. It was also remarked that leaders new to the role are likely to need coaching themselves.
‘Leaders need to get coaching/mentoring during the first six months of their new role.’
‘Nurses need to be excellent role models and good communicators.’
‘Leaders need to have time to be able to work on the wards to provide that role modelling opportunity.’
‘Coaching, mentoring and succession planning/professional development.’
‘Coaching skills will be required by leaders to empower teams to reach their potential.’
Many of the comments in this subcategory were presented in the form of short segments and not fully elaborated. However, they fitted ‘interpretatively’ with this overarching category (‘creating positive healthcare cultures’) because the concepts of role modelling, coaching and mentoring were construed as relating to the less visible aspects of health service organisations.
Digital capability/competence
Technology skills
There was a wide variety of comments throughout regarding the digital capability/competence of future leaders. Although direct nursing care was considered a core skill, nursing and midwifery practice was noted to be (and increasingly expected to become) informed and driven by technology and technological advancement. Consequently, leaders would need to be competent in this area.
‘Technology will also play a part in consultations, with more online appointments, maybe to triage face-to-face work, so IT facility will be needed there too.’
‘In 2030, nurses and midwives will require advanced leadership skills such as digital literacy for managing health technology, adaptability to evolving healthcare models.’
‘Technology is likely to be playing an ever-increasing part in healthcare so we need to ensure our leaders are equipped for this.
New technology was commented on in relation to ways of communicating with patients. However, these comments were fragmented and difficult to interpret, eg ‘new IT solutions’.
‘Embracing new technology to communicate.’
‘New IT solutions.’
‘Using new technology to interact with patients.’
Understanding AI
Other comments noted the need for nurse and midwife leaders to understand that artificial intelligence (AI) would become a facet of their role in the future. Some of these comments were fragments, whereas others described the need for AI to be used to enable the nursing role to evolve alongside developments in technology.
‘Working alongside AI.’
‘Leadership development for technology, innovation, AI.’
The need for future leaders to keep up with technological developments was notable across this category.
‘I imagine that AI will play a much more prominent role so CPD will be even more necessary to keep up with developments.’
‘A good level of digital skills and understanding of AI/ML [machine learning] technology will be required with an openness to work outside of traditional roles of nursing but instead at the intersection of different industries in order to raise the profile of nursing to help improve health and preventing illness.’
‘There needs to be a far higher level of digital and data literacy …We need to understand that virtual nursing is a reality.’
E-records/data analysis
As previously stated, the comments of some respondents were short and fragmented, whereas others elaborated at greater length, noting the need for leadership to encompass AI, technology, and enable healthcare staff to develop digital capability to improve patient care and/or outcomes.
‘Nursing leaders should be comfortable with healthcare information systems, electronic health records (EHRs), and telemedicine technologies. Understanding data analytics and utilising technology to improve patient care and outcomes will be crucial.’
‘Data analytics, data science skills, understanding of technology impacts of care.’
‘Nursing leaders should have skills in data analysis, interpretation, and using data to improve patient care and resource allocation.’
Across the corpus of data, comments in the overarching category of ‘digital capability/competence’ were much more expansive, and comments on this topic were more prevalent than comments in the other overarching categories.
Systems thinking
Policy/regulations
The final overarching category included comments that future leaders would apply an approach that would take into account the overall system, as well as its individual parts. Moreover, the comments reflected the wider landscape within which health care takes place. Respondents referred to policy and the political drivers that regulate and govern healthcare practices. Comments referred to complexity and decision-making with regard to patient care, as well as planning for the future of the profession.
‘Complex decision making with a good background on policy and regulation.’
‘Awareness of government policy and plan ahead of time.’
‘Understanding healthcare policy and advocating for changes that benefit patients and the nursing profession.’
‘Political acumen to articulate the impact of nursing and midwifery and ensuring that we are represented.’
Interdisciplinary structure
Multidisciplinary working was noted, and comments were made in relation to interdisciplinary care and the structure of care systems, this included reference to digital systems and technology within the wider structure that would benefit service improvements. Likewise, digital literacy was noted as important for enabling a systems thinking approach to health care in the future.
‘…an understanding of the organisational structure of the NHS (eg ICS/ICB etc) systems working and a focus on population health.’
‘…ability to lead interdisciplinary teams to provide holistic care.’
‘A system led approach to support reporting, data and service improvement.’
‘To be leaders of the future nurses and midwives need exposure to the wider systems of our NHS, University's, ICB's, AHSN's.’
‘Digital proficiency, inclusivity, systems thinking, research aware and enabling.’
Complexity
Ultimately, the need to understand complexity was noted as key to the future of nursing and midwifery leadership. The comment below is representative of such comments and is the final subcategory within this overarching category.
‘The world seems to be ever more complex, and the pace of change is accelerating. Although it is hard to accurately forecast the state of the world in a decade, there are forces which will likely shape our world, as well as health and care, in 2030: science and technology, sustainable environment, and socio-political changes.’
Again, as noted within previous overarching categories, the idea of technology and technological advancements was of major significance within the category ‘systems thinking’.
Discussion
This first stage service evaluation has gained a variety of perspectives regarding the perceived skills and knowledge that future nurse and midwife leaders might need. The authors were able to generate both qualitative and quantitative data from the questionnaire. In this article, the authors focused on a qualitative data analysis generated from the responses received to the open question:
- Imagine the health and care system in 2030, what different and additional leadership skills and attributes will nurses and midwives need?
The findings of this evaluation support contemporaneous research showing that transformational and authentic leaders can positively influence healthcare cultures, which in turn will reduce adverse events and improve standards of health care (Labrague, 2024). Analysis of the questionnaire comments underlines the need for leadership development programmes to focus on transformational styles of leadership and to evaluate this in relation to patient safety and healthcare outcomes. This is important as competent leaders are known to be crucial for the development of psychologically safe organisational cultures, which are antecedents to enhancing patient safety (O'Donovan and McAuliffe, 2020; Wang et al, 2021).
Data analysis for the current study highlighted comments in the overarching category ‘digital capability/competence’. Across the data, digital technologies – and the idea that future leaders will be digitally capable – was clearly a focus of the comments, many of which were made specifically in relation to communication and patient care. This is consistent with the findings of Desveaux et al (2019), underlining the importance of leadership in digital innovations and the successful implementation of digital healthcare systems. However, respondents also made clear that this increase in the use of digital technology would need to be balanced with the underpinning personal values/traits of nurse leaders that could not be replaced with technology, namely the delivery of compassionate, humanistic, holistic care. This resonates with the idea that the development of compassionate healthcare cultures facilitates positive patient experiences and enhances health outcomes, as has been observed in a variety of contexts (West, 2020; Malenfant et al, 2022; Bond et al, 2024).
The values and traits described across the data were also notable in relation to the capacity of future leaders to create positive healthcare cultures, for example, emotional intelligence, working collaboratively and in a supportive way was considered important for staff to have positive working environments (as well as enabling patients to have a voice). Likewise, the professional voice was considered to encourage strong leadership. However, the comment types made in this category were short segments and not fully explained, which made the meaning of ‘professional voice’ unclear. On the other hand, this may indicate individual feelings relating to agency, or respondents may be unable to elaborate on how this might be achieved in the future. Finally, the analysis revealed comments relating to the complexity of healthcare systems. Future leaders will need to understand this complexity, as well as how to function effectively within complex healthcare environments, to realise positive outcomes for patients in the future.
Limitations
There are several limitations to this evaluation. First, in terms of geographical area, the majority of the responses came from participants working in England, with 98 people indicating that they worked in the UK. This makes it difficult to comment on whether the findings could be extrapolated and would be relevant in a global context.
Second, with respect to the ethnicity of respondents, the majority (n=60; 59.4%) wereWhite, so the data are not necessarily representative of the diversity of the healthcare workforce. However, the proportion of non-White respondents was greater than the proportion of registered nurses, midwives and nursing associates from Black, Asian and minority ethnic backgrounds, recorded as 27.7% as of March 2023 (NMC, 2023). It should be noted that the number of registered nurses and midwives changes daily, so it is difficult to determine accurately whether the composition of the study sample was representative of the UK workforce.
This makes it difficult to ascertain the direct transferability of the findings to other contemporary healthcare contexts. However, the majority of healthcare leaders in the UK areWhite, according to current statistics (NHS England, 2022).
A large proportion of respondents (86.1%) were registered nurses and midwives, representing a wealth of professional knowledge and experience, which enhances the credibility of the study's findings and represents the lived experience and expectations of the respondents.
Most respondents were either alumni (n=46), or supporters of the FNF (n=18). These viewpoints could consequently be perceived as being biased due to respondents providing answers that they expected would be seen in a favourable light by their peers or because there could be a perceived conflict of interest. The co-authors of the study are also employees of the organisation that disseminated the questionnaire among its professional networks. However, the analysis was undertaken by a researcher external to the organisation, which aimed to reduce bias and mitigate conflicts of interest.
A minority (n=12) of the 101 respondents did not provide any open responses/comments. Additionally, some participants provided a very short response using a few words, for example ‘increased use in technology’. In some cases, a one-word answer was provided, eg ‘compassion’. This limited the amount of qualitative data received. Therefore, the meanings within the data may be limited due to these shorter responses. Eighty-seven respondents were registered professionals, with the remainder responding ‘other’. It is therefore reasonable to state that this was a clearly defined and highly representative sample of participants, which strengthens the relevance and significance of the findings (Morse, 1999; Cho and Trent, 2006).
Conclusion
Leadership development for future nurse and midwife leaders should place emphasis on transformational and transformative leadership. There needs to be more research with a focus on identifying the underpinning mechanisms of change and ‘how’ tranformational leadership styles might be linked to safety cultures, improvements in health outcomes and better patient care.
Key personality traits and digital skills are essential for future leaders in nursing and midwifery. Communication skills are especially important in technology-focused environments, allowing leaders to engage with both patients and staff. Compassionate and inclusive leadership is also vital, and emotional intelligence is core to creating psychologically safe workplaces.
Given the ongoing challenges in health care, resilience and adaptability will enable leaders to foster supportive work cultures, champion team innovation, and promote staff wellbeing through mentorship and career development. In terms of digital skills, leaders will require a high degree of digital capability and technical competence. As health care becomes increasingly technology driven, leaders should be skilled in AI, digital health records, and data analytics to enhance patient care and organisational efficiency.
Finally, a strong sense of professionalism and development of a ‘professional voice’ in decision-making is necessary as this will enable future leaders to advocate effectively for the advancement of their profession.
KEY POINTS
- The study explored perspectives on the leadership skills and attributes future nurses and midwives might need
- Digital competency was perceived to be important, however, this was not viewed as a replacement for humanistic approaches to nursing and midwifery leadership in the future
- Transformational and authentic leaders can positively influence healthcare cultures, which reduces adverse events and improves standards of health care. This should be the focus of future leadership development programmes
CPD reflective questions
- How do you enable a culture of safety within your clinical team? Write a list and see if this matches any of the subcategories found from the content analysis presented in this article
- As a leader, what does it mean to have a strategic view of health care and how would you explain this to newly qualified nurses to help them understand complexity and promote patient safety?
- Reflect on a time when you felt ‘psychologically safe’ and where there was an ‘open culture’ of safety promoted within the workplace. Who was leading the team and what skills and attributes did they possess?