
The human body strives for a core temperature within a narrow interval around 37 °C (Sessler, 2015). All cellular activity is temperature dependent and a change of ±0.2 °C affects vital organs and their function and will start a range of compensatory mechanisms to maintain normal core body temperature in a healthy individual (Sessler, 2015). When a patient is anaesthetised normal temperature regulation is disturbed due to vasodilation, leading to greater heat redistribution (Sessler, 2016). Inhibition of the thermoregulatory response leads to a delay in compensatory factors, which will not occur until a temperature change of up to 4 °C (Scott, 2012).
The National Institute for Health and Care Excellence (NICE) clinical guideline defines normal body temperature as a core temperature of 36-37.5 °C and recommends a preoperative core temperature of 36.5-37.5 °C (National Collaborating Centre for Nursing and Supportive Care (NCCNSC), 2008; NICE, 2016). Hypothermia is defined as a core temperature below 36 °C. Despite a database search, the authors were unable to find any guidelines relating to recommended peripheral temperatures. National recommendations or guidelines regarding hypothermia do not currently exist in Sweden, hence the use of British guidelines. According to the NICE guideline, interventions should be put in place when a patient's core temperature drops below 36 °C, but it also states that it is better to prevent hypothermia as it is difficult to increase the temperature of an already hypothermic patient (NCCNSC, 2008: 55).
Perioperative hypothermia is one of the main complications for patients undergoing surgery (NCCNSC, 2008). The majority of heat loss occurs during the first hour of surgery (Matsukawa et al, 1995) when redistribution of heat occurs as the core and peripheral temperatures differ (Sessler, 2000; Tansey and Johnson, 2015). A decrease of peripheral temperature prior to surgery has been shown to increase the risk of developing hypothermia (Matsukawa et al, 1995; World Health Organization (WHO), 2009). Apart from discomfort, hypothermia also puts the patient at risk of prolonged hospitalisation with increased costs for society as a result (Kurz et al, 1996; Sessler, 2016). Other complications of hypothermia include coagulopathy, increased bleeding and need for blood transfusions, decreased immune activation with reduced wound healing and increased postoperative infections and pressure ulcers (Scott and Buckland, 2006; Rajagopalan et al, 2008; Billeter et al, 2014; Torossian et al, 2015; Sessler 2016). Risk factors for developing hypothermia include having multiple comorbidities, age over 65 years, and male gender (Billeter et al, 2014; Kim and Yoon, 2014; Wetz et al, 2016).
Interventions for postoperative hypothermia can be made preoperatively (de Brito Poveda et al, 2013; Sessler, 2016). However, reheating the patient intraoperatively to normal body temperature could take many hours, a factor that becomes a problem for the day-surgery patient spending less time in the operating theatre.
There has been a considerable amount of research studying how hypothermia develops during the intraoperative phase and the resulting complications (Rajagopalan et al, 2008; Burger and Fitzpatrick, 2009; Lynch et al, 2010; Horosz and Malec-Milewska, 2013; Billeter et al, 2014). However, research into the prevalence of hypothermia during the preoperative phase is scarce. One study found that the greatest loss of temperature perioperatively was in the preoperative phase, including the induction of the patient (Read et al, 2018). A few other studies measured the body temperature preoperatively, on arrival at the preoperative unit or just prior to induction (Mitchell and Kennedy, 2001; Wetz et al, 2016). No study has been found comparing these measurements to see whether the temperature of the patient declines during the preoperative phase (not including the induction of the patient). Therefore, it cannot be stated that the interventions to preserve normal body temperature are sufficient. Studying temperatures preoperatively may provide early indicators of hypothermia and are therefore vital in the prevention of it. The authors' personal observations of patients during the preoperative phase have given an indication that there may be a risk of the patients' temperature decreasing, the lack of available evidence prompted this study. The results of this research begins to fill that void and significantly contributes to the literature.
Aim
The aim was to study day-surgery patients' peripheral and core temperatures during the preoperative phase. The hypothesis was that the temperature would decrease.
Method
A non-experimental quantitative design was adopted to carry out a prospective observational study (Polit and Beck, 2016). A convenience sample of patients undergoing day surgery at a county hospital in the south of Sweden in February 2019 was used. Inclusion criteria were day-surgery patients above 18 years of age, undergoing surgery and having given oral consent to the study. Exclusion criteria were any patient with a cognitive or mental disorder. Measurements were taken from 58 patients, out of which 50 were included in the study. Eight cases were eliminated because the secondary measurements could not be completed in a similar fashion to the first measurements. Of the 50 participants, 47 were placed in a bed and 3 placed in an armchair waiting to be transported to the operating theatre, all patients received socks and blankets. During the study a total of 174 surgeries were performed at the day-surgery unit, making the sample greater than 28% of the total population, providing a representative sample size for statistical analysis, and therefore increasing the credibility of the results.
Data collection
Measurements were performed twice for each patient: once shortly after the patient's arrival at the day-surgery unit, having just changed into surgical attire, and again as the patient had just been placed on the operating table in the operating theatre. All were conducted according to local guidelines. Measurements of the patient's core and peripheral temperatures were made on both occasions. Because standard clinic procedures entail only measuring patients' core temperature, measurements of peripheral temperatures were performed specifically for this study.
All patients in this study stayed in the same day-surgery unit. The temperature of this ward is centrally controlled and cannot be changed by staff on the unit. It is therefore presumed that all patients were under the same temperature conditions regarding room temperature. The time between the first and second measurement varied from 30 minutes to 3 hours 30 minutes, with a mean of 1 hour 36 minutes.
The reliability of the thermometers was calculated using double measurements before starting data collection. The double measurements were made using the same thermometer on the same patient, twice, directly following each other, and the data compared and statistically validated. The core temperature was measured using an axillary digital thermometer (Terumo brand) in accordance with the NICE guideline (NICE, 2016). The thermometer was set to measure a calculated core temperature. The same thermometer was used for all measurements. The peripheral temperature was measured at four locations (forearm, chest, thigh and calf) using a Mastercool 52224-A infrared thermometer. The thermometer was placed at a right angle towards the point of measurement. To allow for measurements of the same location a 0.5 cm mark was made at each location, which was then removed after the second measurement. To allow for the same distance (3 cm), and therefore area of measurement (2.5 cm x 2.5 cm), a measuring stick was mounted on the thermometer. This allowed the thermometer to be placed in the same location and distance for comparison between the first and second measurement. The measurement cannot be felt on the skin and did not cause any discomfort to the patient.
The same observer (either the first or second author) performed the same type of measurements on the same patient to minimise the risk of bias in measurements.
Data analysis
Data analysis was performed using SPSS software version 25. The Kolmogorov-Smirnov test was used to calculate the probability of normal distribution (Polit and Beck, 2016), where all data were considered normally distributed. Descriptive statistics were used to compare data variables using means, standard deviation, minimum and maximum. A paired t-test was then used to calculate statistical significance using a 95% confidence interval. To explore any covariance, calculations were made for Pearson's correlation coefficient (Polit and Beck, 2016). A test-retest was used to calculate the intraclass correlation coefficient, using a 95% confidence interval, revealing high to very high reliability of the instruments.
Ethical considerations
Permission for the study was granted by the director of the department. According to the Swedish Act regarding the ethical review of research involving humans [SFS 2003:460], no permission from an ethical review board was required due to the fact that no physical impact was made on the patients involved in the study. The ethical processes were in accordance with the World Medical Association (2008) Declaration of Helsinki.
Results
A total of 50 patients (male n=15, 30%; female n=35, 70%) ranging from 19 to 84 years of age participated in the study. Sample demographics are summarised in Table 1.
| Variable | Number of patients | Proportion | |
|---|---|---|---|
| Age (years) | 19–30 | 12 | 24% |
| 31–40 | 4 | 8% | |
| 41–50 | 5 | 10% | |
| 51–60 | 10 | 20% | |
| 61–70 | 8 | 16% | |
| > 70 | 11 | 22% | |
| Gender | Male | 15 | 30% |
| Female | 35 | 70% | |
| Location | Bed | 47 | 94% |
| Armchair | 3 | 6% | |
| TOTAL | 50 | 100% | |
Table 2 and Figure 1 give an overview of the data collected. Measurements showed a significant decrease in temperature on the upper body (forearm and chest). The mean first measurement temperature for these was 30.6 °C and 33.3 °C, respectively. The second measurement mean temperature was 29.5 °C and 33.0 °C. Temperatures decreased by 0.04–1.6 °C. Covariance according to Pearson's correlation coefficient was significant (P<0.05).
| Location of measurement | Mean (°C) | Standard deviation (SD) | Range minimum – maximum (°C) | P value | Direction of change |
|---|---|---|---|---|---|
| Peripheral—forearm 1 | 30.6 | 1.285 | 27.9–33.3 | 0.000 | ⇩ |
| Peripheral—forearm 2 | 29.5 | 1.885 | 23.9–33.6 | ||
| Peripheral—chest 1 | 33.3 | 1.051 | 30.4–35.6 | 0.026 | ⇩ |
| Peripheral—chest 2 | 33.0 | 0.975 | 30.7–35.1 | ||
| Peripheral—thigh 1 | 29.2 | 1.338 | 26.8–32.4 | 0.000 | ⇧ |
| Peripheral—thigh 2 | 31.1 | 1.445 | 28.4–34.8 | ||
| Peripheral—calf 1 | 30.7 | 1.565 | 27.6–33.8 | 0.001 | ⇧ |
| Peripheral—calf 2 | 31.4 | 0.999 | 28.7–34.3 | ||
| Core 1 | 36.6 | 0.459 | 35.4–37.7 | 0.103 | ☐ |
| Core 2 | 36.7 | 0.445 | 35.9–38.1 |
First measurement made when the patient had just arrived at the day-surgery unit
Second measurement made in the operating theatre
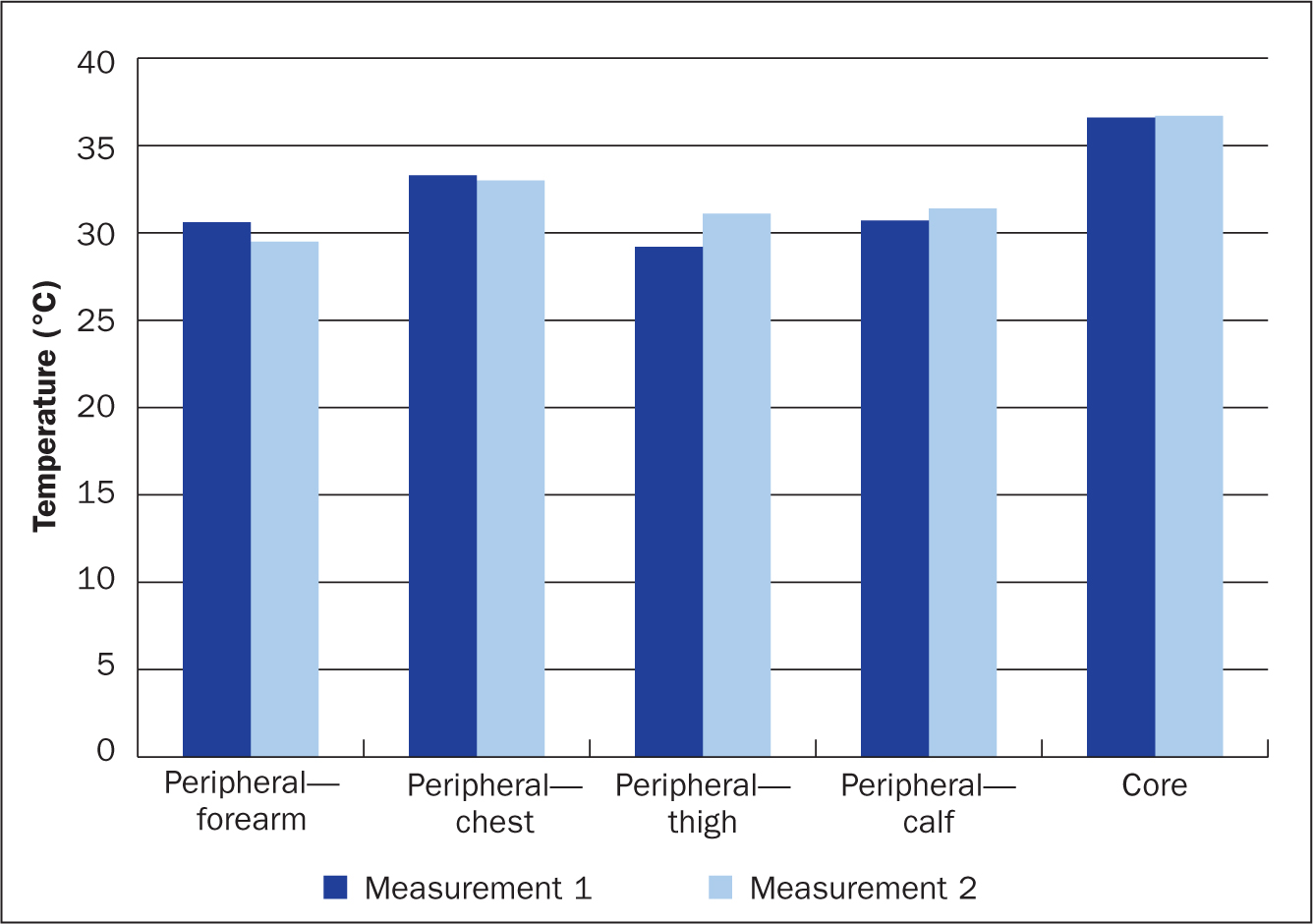
Measurements on the lower body (thigh and calf) showed a significant increase in temperature. The mean first measurement temperature for these was 29.2 °C and 30.7 °C respectively. The second measurement mean temperature was 31.1 °C and 31.4 °C respectively. Temperatures increased by 0.3–2.3 °C. Pearson's correlation coefficient showed a significant covariance (P<0.01).
Measurements of core temperature showed no significant change with a mean temperature of 36.6 °C at the first measurement and 36.7 °C at the second measurement.
A core temperature within preoperative recommendations was maintained for 29 patients at the first measurement and 34 at the second measurement. The number of patients below recommended preoperative core temperature, although not hypothermic, was 16 at the first measurement, and 13 at the second measurement. Seven of these patients (14%) had temperatures below recommended preoperative core temperatures at both measurements. Thus, 28% of patients (13 with temperatures in the range 36.0-36.4 °C and 1 with a temperature below 36 °C), had core temperatures below the recommended core body temperature at the second measurement. See Table 3 for an overview.
| Temperature | Number of patients at first measurement | Number of patients at second measurement | Unchanged temperature level at both measurements |
|---|---|---|---|
| >37.5 °C (hyperthermia) | 1 | 2 | – |
| 36.5–37.5 °C (recommended preoperative core temperature) | 29 | 34 | 24 |
| 36.0–36.4 °C | 16 | 13 | 7 |
| <36 °C (hypothermia) | 4 | 1 | 1 |
Discussion
The aim of this study was to study core and peripheral temperature of day-surgery patients during the preoperative phase. The hypothesis of temperature decreasing during the preoperative phase was partly incorrect. The main finding in this study was that there was no statistically significant difference in core temperature preoperatively. Previous research found that the biggest loss of temperature throughout the perioperative period was in the preoperative phase (Read et al, 2018) something this study was not able to confirm. The reasons for this could be attributed to external factors, such as room temperature, which was not measured in this study, and must be considered a limitation.
The results show a significant decrease in temperature of the upper body and a significant increase in temperature of the lower extremities. The reason for the measuring points on the upper body decreasing while lower extremities increase in temperature can be related to the fact that patients are often more exposed on the upper body, making them more prone to heat loss. The lower extremities were covered by clothing and blankets to a larger extent, providing passive warming for the patient (Bennett et al, 1994). The difference in results on the various measuring points can therefore be related to different prerequisites of the body parts to maintain normal body temperature, something proved in a previous study (Wang et al, 2016).
Although the results of the peripheral measurements proved to be more surprising, the core temperature is still considered the main result as it is more closely controlled, as described previously. It is normal for the peripheral temperature to vary throughout the day, but it will still affect the core temperature when a patient is anaesthetised and the control of temperature is removed (Sessler, 2016).
The results of this study show that mean core preoperative temperature do not change significantly, but they also show that 28% (n=14) of participants were below recommended preoperative temperature and therefore at risk for developing hypothermia. It is not enough for a patient merely not to be hypothermic (<36 °C) to optimise them for surgery. A patient should have a core temperature within the recommended preoperative range (36.5–37.5 °C) (NCCNSC, 2008). According to the perioperative model developed by Tollerud et al (1985), an evaluation of risk factors for hypothermia ought to be made for every patient in order to provide cost-effective, high-quality care. By doing this the nurse is providing person-centred care to each individual according to their needs, physical or psychological.
The results of this study contribute to the existing knowledge regarding perioperative hypothermia; knowledge which is vital for the nurse in charge to be able to evaluate the effect of heat-conserving interventions given preoperatively at a day-surgery unit. A previous study (Boet et al, 2017) showed that lack of feedback about how heat-conserving interventions affected patients' temperature contributed to staff not prioritising interventions for prevention of hypothermia at the surgical unit. The results of this study provide the kind of feedback staff need to notice how heat-conserving interventions affect day-surgery patients. It seems that body parts covered by blankets are better able to maintain temperature. This knowledge could be used in preoperative care of day-surgery patients, with nursing staff ensuring the patient is not exposed more than necessary and thereby increasing the likelihood of better patient outcomes.
In contrast to this study, other similar studies have not had normally distributed data (Mitchell and Kennedy, 2001; Wetz et al, 2016). The reason for these differences may be due to difference in sample size as well as demographics. The reliability of the results of this study is, however, consolidated by the sample size in comparison with the total population, as well as the fact that the analytical process of the result has been reviewed by external expertise (statistician and professional linguists).
Limitations and recommendations
There was a risk of bias in that the presence of the observers could have changed the behaviour of the staff at the day-surgery unit, making them more aware of the patient's temperature, using preventive and heat-conserving methods to a larger extent than they would normally have done. The temperature measurements could also have affected the patients, making them more aware of being cold and therefore using heat-conserving measures. If staff or patients were to use heat-conserving interventions to a larger extent than normal this could affect the validity and reliability of the results (Polit and Beck, 2016). However the researchers noticed no difference in the nurses' or patients' behaviours as a result of the observers' presence. Passive heat-conserving measures were given according to already existing local guidelines, and forced-air heating systems were only used according to guidelines, on patients with a core temperature below 36 °C. Therefore, it can be stated that the risk of bias is insignificant.
A drawback of a cross-sectional study, such as this one, is that data cannot be retrieved over a longer period of time and thereby provide patterns over time (Polit and Beck, 2016). Another limitation is that statistical power was not calculated before the start of the study. However, a relatively large sample has been achieved, which increases the generalisability of the study to a larger population. Based on the chosen method, no causative correlation can be assumed, because assumptions would be made on confounding factors leading to spurious correlations. Avoiding such correlations allows for greater validity and reliability in the results. Reliability is further strengthened by statistically validating the instruments used in the study. Limitations of the study include measurements only being taken from one hospital unit, decreasing the generalisability of a greater population. The time interval between the first and second measurements poses another limitation as it varies and therefore could affect the results.
Due to the fact that no guidelines regarding perioperative hypothermia exist in Sweden at the moment, it is recommended that evidence-based guidelines are created. At present it is standard procedure not to intervene until the patient's core temperature is below 36 °C. This study has added to the evidence regarding preoperative hypothermia by showing that the upper body is prone to becoming cold and it is therefore the authors' recommendation that the upper body of the patient be covered up.
Conclusion
Hypothermia is a common but preventable risk factor of the patient undergoing surgery, and previous research has shown that preoperative decrease in temperature increases the risk for hypothermia. Day-surgery patients are at greater risk due to the short window of time available for them to be reheated. To the authors' knowledge, no previous research has studied whether peripheral and core temperatures of a day-surgery patient change during the preoperative phase. This study has shown a majority of day-surgery patients who are cold on arrival at the day-surgery unit will remain cold throughout the preoperative preparations. Passive and active reheating interventions already exist and should therefore be put to use, to ensure the patient undergoing surgery does not suffer the negative effects of hypothermia. Further research is needed to determine at what point reheating interventions ought to be introduced as well as how day-surgery patients' body temperature fluctuates throughout the perioperative period.