

Events such as the COVID-19 pandemic, the wars in Ukraine and Gaza, and the Black Lives Matter protests have highlighted the need for increased awareness of mental health issues across a broad section of the population: schoolchildren, families, health professionals and other essential workers; even pregnant and birthing women (Choi et al, 2020; Choitz and Wagner, 2021). Never before has there been so much focus on trauma and its effects. The past few years have been traumatic worldwide. There has been racially motivated violence, killings captured and shared on social media, political unrest and widespread protesting (Choitz and Wagner, 2021), all of which can be directly or indirectly traumatising. In England, nearly 50% of all adults have experienced a traumatic event (Bellis et al, 2014), and the World Health Organization reported that 70% of those surveyed experienced lifetime trauma (Kessler et al, 2017). These events provide a unique opportunity to advocate and raise awareness of the need for trauma-informed care (TIC) in multiple settings, including acute care.
According to the Substance Abuse and Mental Health Services Administration (SAMHSA) (2014a), trauma results from an event or series of events experienced by an individual as harmful, either physically, emotionally, or as life-threatening, and has lasting effects on a person's functioning and ability to cope. Trauma can occur at any point in a person's life and can have a lasting impact; it is widespread, crossing all socioeconomic, ethnic, gender or age boundaries (SAMHSA, 2014a; 2014b). Clinicians are familiar with the term post-traumatic stress disorder (PTSD), a psychiatric disorder that may appear in those exposed to a traumatic event such as combat (American Psychiatric Association, 2022).
Trauma falls into the three broad categories of household, community and environment (SAMHSA, 2014b; Choitz and Wagner, 2021). Examples of trauma include experiencing or witnessing domestic violence, terrorism, or violence (for example, seeing someone killed). Trauma also includes experiencing natural disasters (SAMHSA, 2014a). Trauma divides into big ‘T’ and little ‘t’ categories and these would be ‘T’ examples. Little ‘t’ trauma includes bullying, invasive procedures, or cumulative trauma (Wheeler and Phillips, 2021). This list is not exhaustive, but one can see that trauma impacts many people. Trauma is a harmful, extensive and costly public health problem (SAMHSA, 2014a; Tebes et al, 2019; Wheeler and Phillips, 2021), leading to other issues. Exposure to trauma increases the risk of emotional, mental, or behavioural problems and chronic physical illness (Goldstein et al, 2018).
Trauma impacts people in all settings of care delivery. In the past, the focus was on the mental health arena, but it is time for that to change because trauma does not occur in isolation. Rather, it appears in the context of community, and people with trauma histories seek care across multiple domains, requiring a universal precautions approach in care settings (SAMHSA, 2014a; Bassuk et al, 2017; Bruce et al, 2018; Goldstein et al, 2018; Fleishman et al, 2019; Kosman and Levy-Carrick, 2019; Tebes et al, 2019; Wheeler and Phillips, 2021).
Historically, trauma in healthcare used a medical-biological/clinical approach to care, that is, a focus on the physical. More recently, healthcare providers understand trauma also has a psychological component. The psychological impact is what remains after the physical part has been addressed. The mental health consequences may not become apparent until long after the event and the physical wounds have healed (Bruce et al, 2018). Psychological trauma is the experience of negative emotional reactions to a given experience. Those negative emotions can manifest as physical problems.
Background
Trauma does not occur in isolation, but within the context of community and the social determinants of health (SDOH), which includes factors such as economic stability, education, and social and community context (SAMHSA, 2014a; 2014b). The World Health Organization (WHO) (2021) defines SDOH as non-medical factors influencing health outcomes, such as the conditions in which people are born and live. Social determinants of health include an extensive set of systems and forces which shape daily life, for example social policy, political organisations, or economic policies (US Department of Health and Human Services, 2021; Centers for Disease Control and Prevention (CDC), 2021). These SDOHs also cross generations and can traumatise individuals or families (SAMHSA, 2014b) and are shown to be related to adverse childhood events.
Adverse childhood events include physical and emotional abuse, sexual abuse, neglect, divorce, or separation of parents, witnessing violence, living with someone who abused drugs/alcohol, living with someone who had a mental illness, or having a family member in prison (Schulman and Maul, 2019; Choitz and Wagner, 2021; Forkey et al, 2021). Thirty-four million children under 18, or roughly 50% of all children in the USA, have dealt with at least one adverse childhood event (Racine et al, 2020; Choitz and Wagner, 2021; Forkey et al, 2021). These children grow into adults, seeking care in multiple settings.
Adverse childhood events occur at the household, community and environmental levels. When combined with poor SDOH, these events can increase the risk for trauma and traumatisation in adults (SAMHSA, 2014a; Sweeney et al, 2018; Choitz and Wagner, 2021; Emsley et al, 2022). TIC needs to start in childhood since most children experience trauma during their formative years. These traumatic experiences will affect physical, developmental, and emotional health across the lifespan (Purkey et al, 2018; Racine et al, 2020; Forkey et al, 2021).
According to the WHO mental health survey, 70% of those surveyed had experienced lifetime trauma (Kessler et al, 2017; Emsley et al, 2022). If natural disasters are included as traumatic events, 15-17% of adults have experienced at least four adverse childhood events (Choitz and Wagner, 2021). In England, a survey found nearly half of all adults lived through at least one adverse childhood event (Bellis et al, 2014), and a crime survey in England and Wales reported that 29% of women and 13% of men experienced domestic violence in their lifetime (Office for National Statistics, 2020; Emsley et al, 2022). These experiences, whether SDOH or adverse childhood events related, have long-ranging health effects that will be seen in the acute care setting. Traumatic experiences can be expressed as poor coping skills or physical conditions requiring care in healthcare settings, including acute care.
The cost of trauma
A financial and emotional cost is associated with not identifying or addressing trauma. The accumulative effects of trauma increase the body's toxic stress burden. Toxic stress refers to the prolonged activation of the stress response system, which can lead to lasting adverse effects on health. This occurs when the stress response is activated, but the body fails to recover fully, and the accumulative effects increase the body's toxic stress burden. The allostatic overload of toxic stress underlies multiple medical problems, leading to a higher frequency of healthcare use and costs (Stokes et al, 2017; Goldstein et al, 2018; Purkey et al, 2018). In England and Wales, those with four adverse childhood events were two times more likely to see their GP recurrently than those without an adverse childhood event history (Bellis et al, 2017; Emsley et al, 2022). Emsley et al (2022) noted that health service use grew as the number of adverse childhood events increased. Trauma-related toxic stress can result in long-lasting or lifelong physical and mental health impairments (Choitz and Wagner, 2021; Forkey et al, 2021). These experiences have a powerful impact on the arc of life (Yatchmenoff, 2015).
Toxic stress is linked to multiple physical conditions seen in acute care, such as arthritis, chronic pain or headaches, cardiovascular disease, chronic obstructive pulmonary disease, obesity, and immune system dysfunction (SAMHSA, 2014a; 2014b; Bassuk et al, 2017; Leitch, 2017; Bruce et al, 2018; Goldstein et al, 2018; Fleishman et al, 2019; Kosman and Levy-Carrick, 2019; Guest, 2021, Han et al, 2021; Forkey et al, 2021). Mental health issues include, but are not limited to, depression, anxiety, PTSD, and aggression or agitation (SAMHSA, 2014a; Beckett et al, 2017; Wilson et al, 2017; Kosman and Levy-Carrick, 2019; Portman-Thompson, 2020). In the acute care setting, patients presenting with any of the conditions listed may have developed them due to toxic stress. Adverse childhood events are associated with poor cognitive function over the long term. Toxic stress accelerates ageing through hormonal and inflammatory conditions, a higher risk of morbidity or mortality from cardiovascular diseases, and an overall lower quality of life (Nkwata et al, 2022).
Patients with a trauma history have higher health service use rates but less adherence to and compliance with treatment (Fleishman et al, 2019). There is a greater need for awareness of population health, cognisance of racial and ethnic disparities, and the negative impact on overall health and wellbeing (Peterson et al, 2021). In the acute care setting, a lack of guidance or awareness of TIC practices, principles, and related skills leads to poor patient outcomes.
The need for trauma-informed care
Trauma-informed care (TIC) is a way to address the manifestations of trauma within the acute care setting. It is an approach that recognises the widespread impact of trauma and seeks to create supportive, accessible, and appropriate care environments for patients experiencing trauma (Buffalo Center for Social Research, 2019). As a patient-centred approach, TIC focuses on resisting re-traumatisation while building resiliency and coping strategies (SAMHSA, 2014a; 2014b; Fleishman et al, 2019; Buffalo Center for Social Research, 2021). The focal points of TIC are on recovery and healing, building positive relationships, and establishing new coping mechanisms (Bowen and Murshid, 2016; Leitch, 2017; Isobel, 2021; Forkey et al, 2021). Trauma-informed care is not prescriptive, as each patient has unique experiences and cultural backgrounds influencing behaviour (SAMHSA, 2014b; Sweeney et al, 2018; Purkey et al, 2018, Tebes et al, 2019).
In healthcare systems where TIC is incorporated into care and treatment, patients spend less time in the hospital, experience higher discharge rates to lower level care settings, and improved outcomes related to mental health and substance abuse (Stevens et al, 2019). In addition, TIC incorporated into organisations improves therapeutic outcomes and decreases adverse effects for both the patient and the organisation (SAMHSA, 2014b).
Nurses in acute care settings must recognise that many healthcare procedures or activities can be retraumatising for patients under their care. How specific treatments are performed can activate symptoms of PTSD because they are invasive and distressing (Bruce et al, 2018; Stevens et al, 2019). Examples include a rape victim being restrained or having a pelvic exam performed, a sexual abuse survivor under constant observation (one-to-one) requiring surveillance in the bathroom and shower, or staff performing tasks during the night. Although staff may not intentionally retraumatise patients, steps must be taken to decrease the risk through training, and changes in the physical environment, policy, and practice (SAMHSA, 2014a; 2014b; Buffalo Center for Social Research, 2021).
Applying TIC principles requires understanding that the human response to high stress or trauma falls into three categories: fight, flight, or freeze. Behaviourally, fight looks like aggression, hostility, or intimidation. Flight is demonstrated through social isolation, emotional withdrawal, and avoidance. Finally, feelings of numbness, anxiety and disassociation are ways freeze manifests (SAMHSA, 2014b; Sweeney et al, 2018; Fleishman et al, 2019; Levenson, 2020). Healthcare providers need to understand these behaviours are, in fact, coping mechanisms, albeit not productive or healthy ones. Trauma-informed care reframes the behaviours from a focus on ‘What is wrong with you?’ to ‘What happened to you?’ and understands these coping mechanisms are the best the person could do given the circumstances (SAMHSA, 2014a, Stokes et al, 2017; Purkey et al, 2018; Sweeney et al, 2018; Portman-Thompson, 2020; Forkey et al, 2021).
Trauma-informed care practices and interventions
Using TIC interventions in healthcare leads to better outcomes. For instance, Oral et al (2020) noted shifting to a TIC approach avoids negative long-term health issues, thus reducing healthcare costs. Additionally, staff themselves benefit through improved health, resilience, and proficiency in providing quality care. Hales et al (2019) identified an increase in patient satisfaction and the belief staff were better able to resolve problems they (the patients) were facing when TIC was used. Finally, Stevens et al (2019) demonstrated patients in organisations with TIC spent less time hospitalised, had better rates of discharge to lower levels of care, and improved mental health and substance use outcomes.
Trauma-informed care practices are needed at the individual nurse level to reduce re-traumatisation and support recovery and growth in those under their care (Becker-Blease, 2017). Trauma-informed care falls within the scope of nursing practice; it is an evidence-based approach to care and treatment that requires incorporation into nursing care and procedures (Isobel and Edwards, 2017; Cilia Vincenti et al, 2022). Each caregiver is encouraged to review practices through a trauma-informed lens, being aware of both the influence of trauma and the principles of TIC (Yatchmenoff et al, 2017). Schulman and Menschner (2018) point out foundational steps are a good place to start, even if an organisation is not ready for full adoption of TIC.
To begin, nurses must be aware of the ‘four Rs’ (see Figure 1) (SAMHSA, 2014a; 2014b; Leitch, 2017; Purkey et al, 2018; Sweeney et al, 2018; Tebes et al, 2019; Guest, 2021). Primary interventions are needed for staff to incorporate into day-to-day activities and behaviours to decrease the risk of retraumatising someone and improve patient wellbeing and outcomes (Figure 2). These are safety, choice, collaboration, trustworthiness and empowerment (SAMHSA, 2014a; 2014b; Beckett et al, 2017; Leitch 2017; Stokes et al, 2017; Purkey et al, 2018; Sweeney et al, 2018; Fleishman et al, 2019; Levenson, 2020; Walsh and Benjamin, 2020).

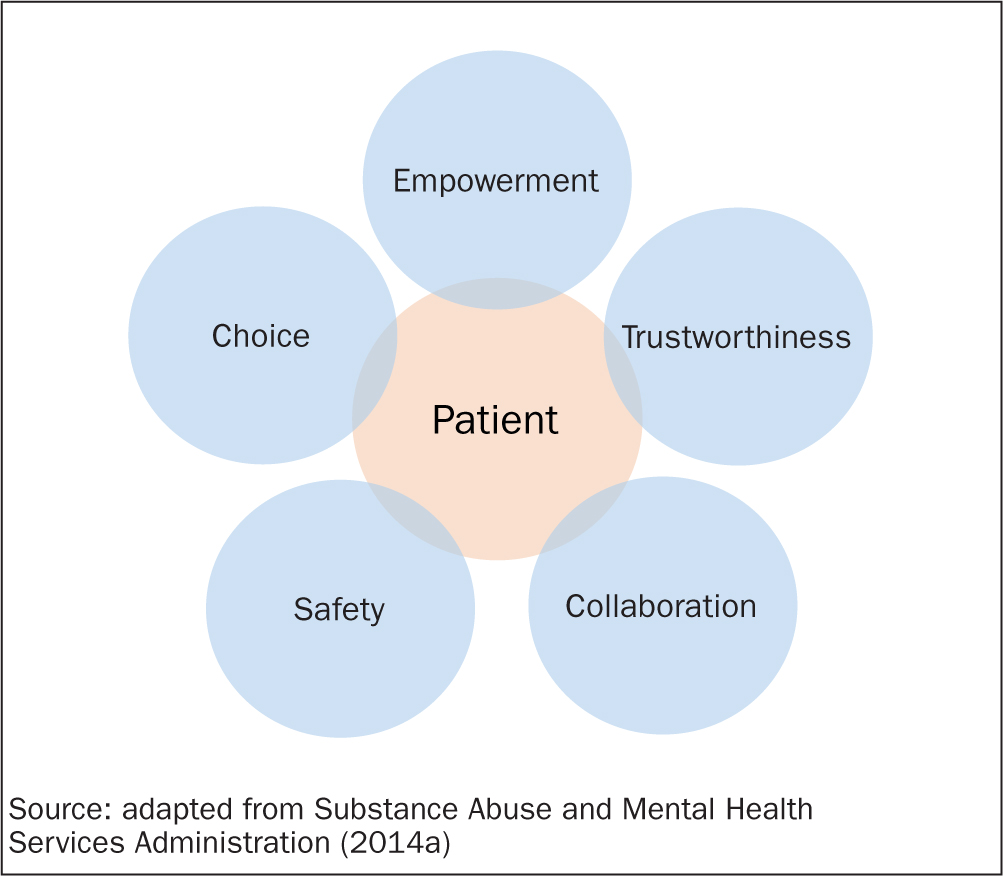
In daily practice, the aim is to ensure that everyone (staff and patients) is physically and emotionally safe and the employees are warm and welcoming, as are common areas. As set out in Figure 2, the following areas are important:
- Safety, especially psychological safety, is vital for patients to share their thoughts and feelings without fear of judgement or reprisal
- Choice involves the patient having choice and control. Staff can ensure patient choice by asking permission to take vital signs, touch the patient, or ask questions. All staff must clearly understand that the patient can say no and that the ‘no’ must be honoured
- Collaboration ensures the patient's voice is heard in treatment planning and priorities. It is a mindset of ‘doing with’ instead of ‘doing to’ the person in the nurse's care
- Trustworthiness has to do with the consistency of staff in applying rules or regulations. Trustworthiness requires employees to be transparent about how or why decisions are made. Staff should be clear when communicating, maintain boundaries, and be respectful towards clients under their care. The consistency and dependability demonstrated in trustworthiness of staff allow patients with a trauma history to feel safe. Often in situations of abuse, there is no consistency and no sense of security, leading to higher states of anxiety and hypervigilance in patients
- Empowerment is concerned with validating patient feelings and experiences while assisting the individual to build new skills and coping strategies (SAMHSA, 2014a; 2014b; Bowen et al, 2016; Beckett et al, 2017; Isobel and Edwards, 2017; Stokes et al, 2017; Unick et al, 2019; Kosman and Levy-Carrick 2019; Isobel et al, 2021; Levenson, 2020; Oral et al, 2020; Portman-Thompson, 2020; Walsh and Benjamin, 2020; Isobel, 2021; Buffalo Center for Social Research, 2021).
Nursing care already incorporates some of these principles, and Jean Watson's Theory of Human Caring further guides the practice with ‘caritas’ factors (Watson Caring Science Institute, 1979). Nurses collaborate with those under their care, model appropriate skills, and interactions, and educate and support patients through a trauma-informed, non-judgemental, patient perspective lens (Wilson et al, 2017; Stokes et al, 2017; Isobel and Delgado, 2018; Wei et al, 2019; Rossillo et al, 2020; Isobel et al, 2021; Portman-Thompson, 2020). Collaboration is accomplished by meeting the patient where they are instead of where the staff thinks they should be (Wei et al, 2019; Rossillo et al, 2020). Establishing profound, caring nurse-patient relationships increases patient satisfaction and quality of care, factors tied to reimbursement in healthcare organisations that are funded by health insurance, as in the USA (Rossillo et al, 2020).
Nurses can also use the four Cs described by Machtinger et al (2019):
- Calm. Remain grounded, calm, and focused when caring for trauma survivors. This behaviour can make interactions productive and healing through emotional regulation
- Contain the interaction. Obtaining a detailed trauma history is unnecessary to being compassionate and helpful. Keep the interaction manageable emotionally for both you and the patient
- Care for the patient. Remember to be non-judgmental and destigmatise the patient's response to trauma, such as drug use, depression, or overeating. Shame and guilt are common reactions to traumatic experiences
- Coping. Focus on the patient's resiliency and strengths. Identify and use their coping skills from the past that could be helpful in the present. Build on their past successes.
Advocacy for policy and practice change
There has been a focus on policy and practice change in the past, but it has primarily focused on reducing restraint use (Sweeney et al, 2018). A consistent national framework is essential to ensure the effective implementation of TIC across healthcare settings. Within the UK, no nationally recognised strategy, consistent terminology, or framework exists to address trauma at the organisation, local government or NHS level (Emsley et al, 2022). Although TIC is endorsed at some levels, there is little follow-through. For example, the NHS Five Year Forward View (NHS England/NHS Improvement, 2014) recommends increasing shared decision-making, choice, improved recovery rates, and improved patient satisfaction with care. The identified goals could be met by incorporating TIC practices into care delivery (Sweeney et al, 2018). However, most documents related to the five-year plan mention TIC in passing; there are no definitions or details (Emsley et al, 2022). At the local level, the implementation of TIC practices is fragmented; driven primarily by impassioned leaders at a given organisation or local authority. This piecemeal approach does not function long-term. There needs to be a united vision for implementing the high-level recommendations (Emsley et al, 2022). TIC is necessary at the individual, organisational, and policy levels if there are to be long-term positive change (Becker-Blease, 2017).
Conclusion
Trauma is a widespread public health issue affecting many acute care patients with physical and psychological presentations. Nurses need to remember the four Rs and adopt a universal precautions approach, providing care as if the person has a trauma history, even if there is no reported or known trauma history. Incorporating the principles of safety, trustworthiness, collaboration, choice, and empowerment into daily interactions will help build caring relationships that support patients and increase satisfaction for both the nurse and the patient, leading to better patient outcomes and improved quality of life. These primary interventions are a holistic approach to care, falling within the scope of nursing practice. Nurses also need to advocate for policy and practice change at the organisational, local, and national levels if they want to improve the lives and health of those under their care.
KEY POINTS
- Psychological trauma impacts the majority of patients receiving care
- The effects of trauma can present as physical or psychological issues and will be seen in all practice areas
- Trauma-informed care is an evidence-based practice that falls within the nursing scope of care
- A universal precautions approach is best when interacting with patients with unknown trauma histories
- Trauma-informed care must be part of policy and practice at the individual, system, and national levels
CPD reflective questions
- Think about your practice setting. Which elements of trauma-informed care do you or your team already practise? Which features do you need to develop and why?
- Which social determinants of health impact the patients you care for? In what way?
- Recall a patient you have cared for with a trauma history. What would you do differently after reading this article?