
Leukaemia is a type of cancer derived from any of the blood-forming cells of the bone marrow tissue, most commonly those forming into white blood cells (National Institute for Health and Care Excellence (NICE), 2016). The most common types of childhood leukaemia are acute lymphoblastic leukaemia (ALL) and acute myeloid leukaemia (AML) (Hoffbrand and Moss, 2015). Children can also be affected by chronic leukaemias such as chronic myeloid leukaemia, although this occurs far less commonly and is not addressed further in this article.
Leukaemia can present with a range of non-specific symptoms, but it can also often mimic other common and less serious self-limiting childhood conditions (Scowcroft, 2013). Thus, maintaining a suspicion, along with a focused approach, is pertinent in preventing a missed diagnosis of childhood cancer (Clarke et al, 2016). A diagnosis of childhood cancer has a significant impact on the entire family, and it is often a time of great anxiety, distress and uncertainty (Children's Cancer and Leukaemia Group, 2014a). The role of the nurse for the child and family starts with recognising the child with leukaemia, delivering high-quality care throughout their ongoing treatment, managing complications, and providing long-term support and information.
This article will focus on the identification and basic management of two principle diagnoses in paediatric haemato-oncology: ALL and AML. Also included is an illustrative case study to highlight some of the challenges that nurses working in different clinical set-ups may come across in their clinical practice.
Epidemiology
Approximately 1850 children are newly diagnosed with cancer in the UK each year, based on 2014-2016 statistics (Cancer Research UK, 2019a). Overall, children in their first 15 years of life have a cumulative risk of being diagnosed with cancer of 1 in 412 for boys and 1 in 472 for girls, with the highest incidence occurring in those under the age of 5 years (Public Health England (PHE), 2018).
Leukaemia is the most common cancer diagnosed in children, accounting for a third of all childhood malignancies. It is the most commonly diagnosed malignancy in those aged less than 5 years (Public Health England, 2018). On average, 412 new cases of leukaemia in children are diagnosed each year in the UK. The 5-year survival rates have improved from 83% in 2001–2005 to 88% in 2011–2015 (PHE, 2015; 2018). Although leukaemia has a good prognosis, it still accounts for the joint largest cause of death from childhood cancers, along with brain tumours (Cancer Research UK, 2017).
An emergency or late diagnosis of leukaemia can significantly impact patient outcomes, including survival rates (Leukaemia Care, 2018). There is limited data available on the extent of diagnostic delays for children with leukaemia. A survey conducted in the UK involving 20 families whose children had a confirmed diagnosis of cancer, found that parents recognised there was something wrong with their child early, often due to a change in mood or behaviour, but this was often discounted by clinicians (Dixon-Woods et al, 2001). This can potentially cause mistrust of health professionals and impair the patient–doctor relationship in the ongoing treatment of the child.
Another UK study involving 21 parents of 18 children with a new diagnosis of acute leukaemia found reasons for diagnostic delay may include patients presenting with non-specific symptoms, a general disregard for parents' initial concerns and a lack of continuity of care in general practice (Clarke et al, 2014). These studies highlight that atypical symptom presentations and parental anxieties regarding their child, such as something being ‘not right’ should be considered seriously and investigated appropriately.
Risk factors
There are several recognised risk factors for the development of leukaemia in children. Nevertheless, it is considered to be a complex interplay of genetics, environmental factors and immune response, which yet remains to be fully understood (Belson et al, 2007). Furthermore, family history plays a role, and should increase the clinical suspicion. Siblings of patients diagnosed with acute leukaemia are at an increased risk, with identical twins running a risk of 1 in 5 (American Cancer Society, 2019a). Likewise, there are a number of genetic conditions (Box 1) that increase the likelihood of developing leukaemia in childhood. An example of this would be a patient with Down's syndrome, representing a 20-fold increased risk (Mitchell et al, 2009).
Classification
Leukaemia is classified by a combination of histological and genetic characteristics of the cell line that it is derived from. Classifying the specific type of leukaemia is an important stage of diagnosis, as it enables the child to receive the correct treatment regimen. The classification of acute leukaemia is depicted in Figure 1 (American Cancer Society, 2019b).
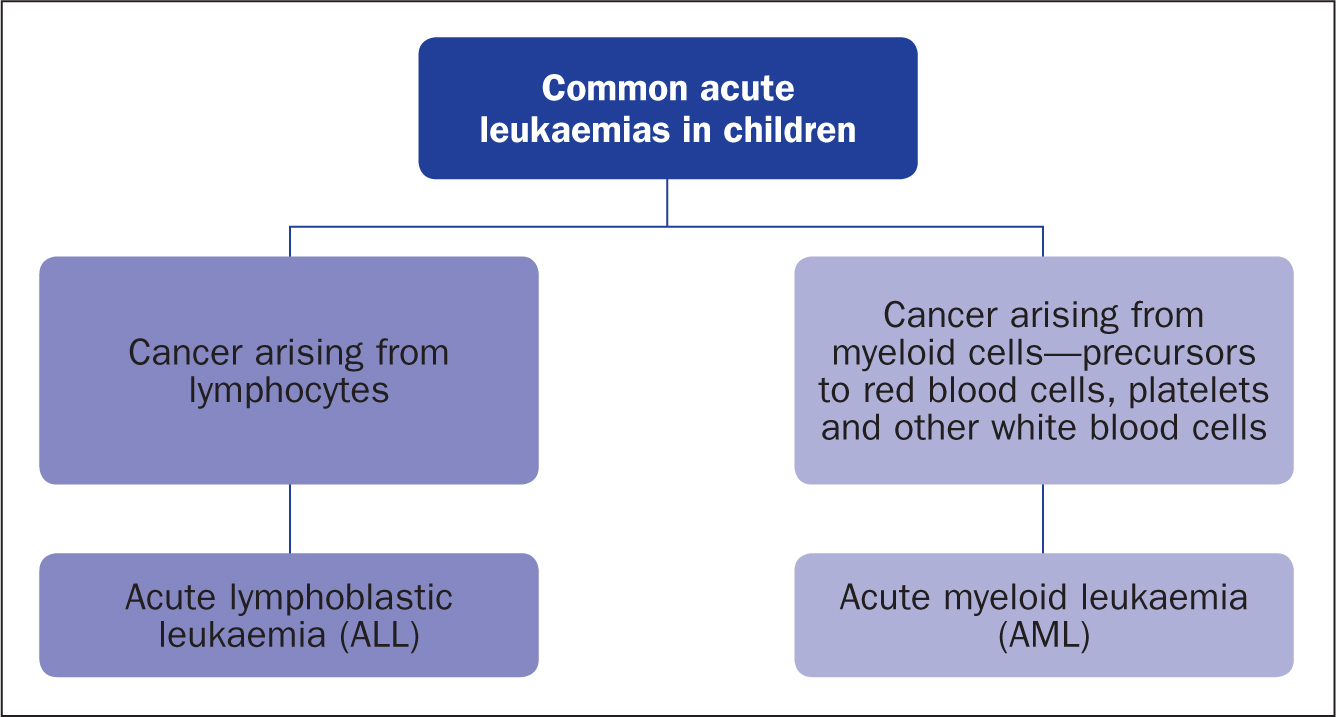
Symptoms at presentation are often overlapping and it can be hard to differentiate between AML and ALL. Both can present with symptoms of dysfunctional or low platelets, red blood cells or white blood cells. Specific symptoms including gum hypertrophy, skin infiltration and extreme weakness and fatigue may be more characteristic of AML, whereas lymphadenopathy is more likely to be seen in ALL (American Cancer Society 2019c).
Clinical presentation
The signs and symptoms of childhood leukaemia can be difficult to distinguish from other less serious and common childhood illnesses, due to the child often presenting with non-specific signs. Concerning features are symptoms that persist without an explanation or ‘red flag’ symptoms such as bleeding and bruising easily. Nonetheless, the presentation can vary considerably; therefore it is essential that health professionals review each body system fully (Scowcroft, 2013).
The presenting symptoms are principally due to three pathological processes: bone marrow infiltration and the subsequent pancytopenia, blast cell infiltration into other tissues, and the systemic effects of cytokine release. This is summarised in Table 1 (Mitchell et al, 2009).
| Systemic effects of cytokines | ||
|---|---|---|
| Generalised symptoms | Malaise | Fever |
| Fatigue | Pruritus | |
| Nausea | Night sweats | |
| Bone marrow Infiltration | ||
| Anaemia | Pallor | Dizziness |
| Lethargy | Palpitations/chest pain | |
| Reduced exercise tolerance | ||
| Thrombocytopenia | Petechiae | Ecchymosis |
| Mucous membrane bleeding | ||
| Neutropaenia | Recurrent or severe infections | Fever |
| Unusual infections such as candidiasis | ||
| Marrow infiltration | Bone and joint pain | Limp |
| Reticuloendothelial infiltration | Hepatosplenomegaly | Lymphadenopathy |
| Mediastinal mass, expiratory wheeze, stridor, cough, orthopnoea | ||
| Other organ infiltration | ||
| Central nervous system | Headaches | Vomiting |
| Cranial nerve palsies | Seizures | |
| Testes | Testicular enlargement | |
| Leucostasis | Headache | Stroke |
| Shortness of breath | Heart failure | |
A systematic review by Clarke et al (2016), which included 33 studies and collectively included 3084 children, described more than 95 common presenting symptoms at diagnosis. The key points demonstrated were that, in children, abdominal and musculoskeletal symptoms were relatively common, in addition to the classical symptoms of abnormal bleeding, bruising and prolonged fever. Furthermore, 6% of children were asymptomatic at diagnosis and many of these children presented with persistent non-specific symptoms mimicking the common, self-limiting childhood illnesses (Clarke et al, 2016). Health professionals should therefore remain aware of risk factors for developing leukaemia, listen to parental concerns carefully and take a full history and complete a thorough examination, to decide whether invasive haematological tests are required.
Less commonly, a child can present as an emergency (Table 2) due to complication(s) arising from the malignancy. Depending on the presentation, they can display a diverse range of symptoms (Theis, 2014). The management of these emergencies are addressed in a later section.
| Airway | Mediastinal mass and superior vena cava obstruction causing acute airway obstruction |
| Breathing | Shortness of breath from anaemia, lower respiratory tract infection, wheeze, acute pulmonary oedema from leucostasis |
| Circulation | Heart failure, low urine output from tumour lysis syndrome, sepsis, leucostasis, major haemorrhage from thrombocytopenia, electrolyte disturbances |
| Disability | Stroke, seizures, raised intracranial pressure, facial nerve palsies |
Differential diagnoses
The differential diagnoses vary widely, dependent on the presenting complaints of the child; the possible diagnoses will vary for the child presenting with joint pains compared to a petechial rash, for example. Table 3 provides the classifications of the major groups of disorders that can mimic leukaemia (Mitchell et al, 2009).
| Infective | Infectious mononucleosis |
| Parvovirus B19 | |
| Viral infections: HIV, cytomegalovirus, influenza | |
| Osteomyelitis | |
| Tuberculosis | |
| Malignancy | Other types of cancer, for example lymphoma or neuroblastoma |
| Autoimmune | Systemic lupus erythematosus |
| Juvenile idiopathic arthritis | |
| Sarcoidosis | |
| Haematological | Non-malignant haematological disorders |
An important differential diagnosis not to miss is non-accidental injury (NAI) in children who can present with bleeding and bruising as an initial symptom. A UK-based review article discussed the difficulties in distinguishing between accidental and inflicted injuries causing bleeding and bruising (Minford and Richards, 2010). Frequent, prolonged, bilateral epistaxis is more likely to be a symptom of leukaemia or another haematological pathology compared to NAI. The location of the bruising may help to raise suspicions of NAI such as those seen on the buttocks, ears and medial thighs, compared to bruising found on elbows and shins (Anderst et al, 2013).
Although this may be a useful guide, this is not absolute and all bruising should be evaluated fully. Where clinical uncertainty remains, a full clinical history should be taken from the patient (where age appropriate) and family, and haematological investigations should be considered. It is important that ALL/AML is considered in the initial stages of a child presenting with extensive unexplained bruising because there have been a number of families where early stages of safeguarding enquiry and assessment may have delayed their diagnosis of a malignancy (Laposata and Laposata, 2005). This inadvertent delay adds to the time to diagnosis and leads to highly distressed parents compounding mistrust in health professionals. Haematological investigations, including a clotting profile and full blood count, should therefore be undertaken early in these presentations to expedite or rule out the diagnosis of leukaemia (Laposata and Laposata, 2005).
Clinical history and examination
A systematic approach, comprising a thorough but focused history and examination, is essential for recognising the child with leukaemia (Raab and Gartner, 2009). The clinical history should include specific and relevant clinical questions (Box 2), the child's past medical history, including predisposing genetic conditions, a thorough social history and an assessment of their growth and development.
Children presenting with unexplained illness require a comprehensive ‘head to toe’ clinical examination to detect clinical signs associated with malignancy. Clinical examination of the child is usually performed by medical professionals or advanced nurse practitioners. However a child presenting with unexplained petechiae, hepatomegaly or splenomegaly should be immediately assessed by a senior paediatrician as recommended by NICE (2017) guidance. The clinical examination should include a thorough abdominal examination, testicular examination in male patients, examination for lymphadenopathy including axillary and inguinal chain, and close inspection of the skin for abnormal rashes or bruising (Clarke et al, 2016).
In a meta-analysis of 3084 children by Clarke et al (2016), 64% of children had a palpable liver and 61% a palpable spleen at the time of diagnosis, thus assessing for hepatosplenomegaly is essential. In pre-pubertal children it is important to palpate for the spleen starting from the left groin as the spleen enlarges in this direction, whereas in adults examination of the spleen should start from the right lower abdominal quadrant.
Investigations
Investigations can be divided into initial and specialist. If malignancy is suspected the suggested first-line investigations are a full blood count (FBC) and a peripheral blood film. Both investigations are sensitive for detecting cytopaenia in addition to peripheral blast cells. However, a normal blood count can occur, especially in the early stages of the disease, if blast cells are restricted to the bone marrow and suppression is yet to occur (Mitchell et al, 2009). NICE (2017) guidance suggests that children who present with one of the stated symptoms (Box 3) should have an urgent FBC within 48 hours, and if a GP (or practice nurse) is concerned they should discuss it with a senior paediatrician (NICE, 2017).
Other initial investigations are done to assess how the leukaemia is affecting the functioning of the body, and can aid in identifying any areas for acute management. Further tests would include assessing renal function to identify any derangement to the electrolytes or acute kidney injury, increased uric acid and phosphate levels to assess for tumour lysis syndrome, a clotting profile to exclude coagulopathy, and a cross-match sample when a transfusion of blood product is considered necessary (Horton et al, 2017).
Children should also undergo a baseline chest radiography to exclude a mediastinal mass or lymphadenopathy in the chest, especially if there are signs of orthopnoea (difficulty in breathing while lying flat on the bed) (Horton et al, 2017).
Specialist tests usually include a bone marrow aspirate and biopsy, which remains the gold standard diagnostic test for leukaemia. Bone marrow will be sent for cytogenetics and immunophenotyping, to classify the type of cancer further to individualise the child's chemotherapy regimen (O'Brien, 2007). A lumbar puncture is usually performed to exclude spread of the malignancy to the cerebrospinal fluid. Box 4 provides an illustrative case study.
Management
Initial management
Initial management focuses on treating any complications caused by the malignancy and stabilising the child before starting specific therapy. The airway, breathing, circulation, disability, exposure (ABCDE) approach, with an emphasis on resuscitation and stabilisation, needs to be undertaken simultaneously while arranging for urgent transfer to a specialist paediatric oncology centre (Theis, 2014).
For a child with airway compromise, immediate escalation to a senior clinician and anaesthetist is required. The child should be positioned upright if there is orthopnoea to keep them comfortable, given supplemental oxygen and administration of sedation should be avoided. If a child is displaying signs of respiratory distress, a non-rebreathe mask with high-flow oxygen should be placed. If shock is present, intravenous access should be obtained, and intravenous fluid bolus(es) should be given. Common causes could include sepsis or haemorrhage and these should be treated specifically. Regular monitoring and recording of paediatric early warning score (PEWS) is suggested, while other specific treatment is administered (Gold et al, 2014).
Chemotherapy
Chemotherapy is the mainstay of leukaemia treatment and is based on pharmacological agents. The chemotherapy regimen will depend on the specific diagnosis: AML or ALL. Treatment is divided into three phases, (Mitchell et al, 2009):
The time needed to complete the full course of treatment is usually a prolonged one for patients to achieve optimal outcomes. This will have an impact on the family, and the social and educational aspects of the child's life. The precise regimen for individual patients is further specified through the use of risk stratification, based on demographic characteristics, cytogenetics and, most importantly, the response to induction treatment. A newer approach through assessment for minimum residual disease (MRD) values has further enabled precise risk stratification, ensuring that children receive the appropriate treatment (Children with Cancer UK, 2017a). MRD is determined by assays to detect very small amounts of residual leukaemia in bone marrow that would not be detectable by simple morphological examination under the microscope (Childhood Leukaemia Clinicians Network, 2016).
Based on their risk, patients are categorised for the consolidation phase of their treatment (Childhood Leukaemia Clinicians Network, 2016). This varies for ALL and AML and is dependent on use of cytogenetic and molecular abnormalities and MRD values to categorise patients into low- or standard-, intermediate-, high- and very-high-risk groups. An example would be a very-high-risk patient whose response to initial treatment has remained poor and who would be considered for haemopoieitic stem cell transplant (HSCT) (Mitchell et al, 2009). Further detailed discussion regarding the categorisation of risk stratification or specifics of treatment is beyond the scope of this article.
Chemotherapy circulates in the body through the bloodstream. In some cases of acute leukaemia, cancer cells may have spread to the cerebral spinal fluid (CSF) where intravenous chemotherapy drugs cannot reach. Intrathecal chemotherapy is therefore administered to prevent the spread/treat cancer cells present in the CSF. The number of intrathecal chemotherapy doses will depend on the presence or absence of blast cells in the CSF made at the time of diagnosis (Childhood Leukaemia Clinicians Network, 2016).
Central venous access
Obtaining early central venous access is important for the long-term delivery of chemotherapy. Most children will receive either a tunnelled central line (Hickman) or a portacath device (Gallieni et al, 2008). Ensuring that the central line is used by a nurse with up-to-date training and necessary expertise can aid in reducing the rate of complications such as infection, chemotherapy extravasation, and line migrations. Health professionals should execute safe principles of managing the line through frequent checks and an aseptic technique (Damani, 2014).
Referral to a tertiary centre
NHS guidance stipulates that once a child has been diagnosed with a cancer they should be referred to a principal treatment centre that specialises in paediatric oncology (Children's Cancer and Leukaemia Group, 2014b). The specialist centre is linked with specific units in the region, usually located in district general hospitals and is designated as a ‘shared care centre’, where the child can continue their ongoing care after initial treatment.
Management of adverse effects of chemotherapy regimes
Leukaemia itself can cause life-threatening or emergency presentations; however, there are also potential emergency clinical presentations that may occur due to the adverse effects of the chemotherapy agents (Table 4).
| Drug | Side effects |
|---|---|
| Vincristine | Peripheral neuropathy, extravasation, rash, syndrome of inappropriate antidiuretic hormone secretion |
| Doxorubicin | Cardiotoxicity, alopecia, loss of appetite, cough, malaise, nausea |
| Cytarabine | Hepatotoxicity, ocular irritation, alopecia, diarrhoea, dysarthria, vasculitis |
| L-asparaginase | Hypercoagulability leading to clots, angioedema, hyper/hypoglycaemia, pancreatitis |
| Methotrexate | Neurotoxicity, necrotising demyelinating leukoencephalopathy, fever, headache |
| Cyclophosphamide | Sterile haemorrhagic cystitis, mucosal abnormalities, progressive multifocal leukoencephalopathy |
| Prednisolone | Increased appetite, fluid retention and weight gain, anxiety, electrolyte imbalances |
Neutropenic sepsis is an important recognised medical emergency in patients receiving chemotherapy. It is defined as a temperature of >38ºC or clinical signs significantly suggestive of sepsis and a neutrophil count of <0.5 x 109/L (NICE, 2012). Sepsis can also lead to other complications, including disseminated intravascular coagulation (Mitchell et al, 2009). Patients who meet this criteria should be admitted and started on piperacillin with tazobactam (if not contraindicated) with close monitoring of vital signs and recording of PEWS (NICE, 2012). A delay in administering the first dose of antibiotics in neutropenic sepsis of more than 1 to 2 hours may cause serious morbidity or mortality (Mitchell et al, 2009).
Tumour lysis syndrome is a life-threatening complication of both the leukaemia itself and its treatment. It causes high levels of potassium, phosphate and uric acid and low levels of calcium in the circulating blood stream. These imbalances can cause cardiac arrhythmias and acute kidney injury (London Cancer, 2014). If the child has tumour lysis syndrome, intravenous hyper-hydration will need to be initiated with accurate monitoring of fluid balance and urine output, and regular monitoring of their biochemistry. Most children will need some intravenous (IV) fluid and prophylactic drugs to protect from tumour lysis syndrome such as allopurinol or rasburicase (Bailey and Skinner, 2010).
Other common side effects of chemotherapy include oral candidiasis and mucositis (Valéra et al, 2015). These can be managed through regular oral rinses with non-alcohol containing solution eg 0.9% sodium chloride and oral moistening with small sponges soaked in water. Longer term serious side effects of specific chemotherapy agents include hepatotoxicity (cytarabine), peripheral neuropathy (vincristine) and cardiotoxicity (doxorubicin), although many children experience few or none of these (Mitchell et al, 2009). Table 4 discusses the side-effects of the most commonly used chemotherapy agents in acute childhood leukaemia.
Role of nurses working in different clinical set-ups in managing children with leukaemia
Nurses play a vital role in the early identification and management of childhood cancers, many of which are summarised in Table 5. In the community setting, nurses may be the first health professional to identify children presenting with symptoms of leukaemia and later be a part of the team managing the child in the community and helping them with reintegration back into the school environment.
| School and community nurses | Early identification and referral if suspected malignancy in a child |
| Raise suspicion if a child has recurrent school absences with unexplained febrile illnesses, easy bruising and breathlessness | |
| Provide support with returning to school after a diagnosis | |
| Ensure any relevant medications are administered appropriately | |
| Practice nurses | Early identification and referral of an unwell child |
| Raise suspicion if a child has recurrent school absences with unexplained febrile illnesses, easy bruising and breathlessness | |
| Ensure siblings are up to date with immunisations | |
| Emergency department nurses | Triage children, identify and escalate any ‘red flag’ symptoms |
| Regular observations and assessment to recognise the deteriorating child using paediatric early warning score (PEWS) | |
| Administration of emergency treatment such as IV antibiotics in febrile neutropenia | |
| Support stabilisation and time-critical transfer to specialist centres of acutely unwell children with suspected malignancies | |
| Providing regular updates and support to parents | |
| Children's nurses | Regular observations including PEWS to recognise if child is deteriorating |
| Communication of concerns if identification of ‘red flags’ of malignancy to clinical team | |
| Ongoing clinical care of child with cancer: IV antibiotics, blood transfusions, pain management, administration of chemotherapy | |
| Parental support and updates | |
| Advanced paediatric nurse practitioners/specialist cancer nurses | Autonomous assessment of children presenting to oncology units, including history and examination |
| Care of central venous access devices | |
| Administration of chemotherapy in inpatient and day-care settings | |
| Identification of unwell child and referral to medical team | |
| Parental support and education | |
| Education of other healthcare providers on core principles of paediatric oncology care | |
| Liaising with oncology multidisciplinary team and secondary care team to plan ongoing management | |
| Provide guidance to parents on applying for disability living allowance | |
| Visit patients in their homes to avoid unnecessary hospital visits, provide direct visits to support schools, and signpost to psychology, social and welfare teams | |
| Health visitors | Early referral to a medical professional if concerned about malignancy in a child |
| Provide support to families following diagnosis | |
| Ensure missed vaccinations are arranged when the patient is not immunosuppressed | |
| Provide support to family and signpost them to support groups |
Clear communication is a key part of successfully managing a child with a diagnosis of leukaemia. Informing a family that their child has cancer is one of the most difficult conversations a health professional will have. It is important that the healthcare team breaking the bad news has the appropriate experience, knowledge and communication skills to do so sensitively but informatively. The principles of giving bad news, available from the Royal College of Nursing (RCN), should be applied with preparation, communication, follow-up and planning. Providing regular updates keeps families well informed; however, it is important, in the early phases, that communication remains reassuring but noncommittal in regard to prognosis (RCN, 2013).
Increasingly, families are taking a more active role in the care of their child, with a shift from inpatient to community care. As a result, parental education before discharge from hospital is of vital importance. This is usually done by the paediatric oncology clinical nurse specialist. Key points to discuss with parents are: how to contact specialist centres, how to liaise with the child's school and how to correctly look after central lines (Aburn and Gott, 2011). Another key point is ‘safety netting’, particularly for when acute medical attention may be required. Patients and their parents should be provided with a written plan and be made aware of the potential complications and adverse outcomes, including an emphasis on neutropenic sepsis. They should be told exactly what to do and who they should contact in an emergency (Bate et al, 2013).
Furthermore, signposting families to support available from specialist groups can help in providing information, social and psychological support. Support groups available include CLIC Sargent, a children and young people's cancer charity (https://www.clicsargent.org.uk/) and Macmillan Cancer Support (https://www.macmillan.org.uk/).
Clinical trials
Most children with a diagnosis of leukaemia will be enrolled on a clinical trial. A key role of the nurse specialist in the paediatric oncology multidisciplinary team is recruitment, monitoring, long-term follow up and parental education about the process, and team coordination (Coulson and Phelan, 2000). A few clinical trials are currently in progress or have completed recruiting, the results of which may provide further direction to some of the unresolved management issues discussed in the article.
Most children with ALL were recruited in a clinical trial called UKALL 2011, which is comparing slightly different methods of delivering the same chemotherapy regimens and measuring whether the same outcomes can be obtained while reducing side effects (Bloodwise, 2010). Results from this trial are likely to be available in the near future.
Another example of a UK-based clinical trial is the MyeChild01 trial, supported by Cancer Research UK. This trial is looking at improving chemotherapy regimens in children with AML, and recruitment for the project remains open until November 2021 (Cancer Research UK, 2019b).
Prognosis
When combined, all types of childhood leukaemia have an 87% 10-year survival rate, which is higher than average for other childhood cancers—this has increased tremendously from 27% recorded in 1971–1975 (Cancer Research UK, 2017). Nevertheless, both the morbidity and mortality differ between ALL and AML, with ALL having a more favourable outcome. For 5-year survival, ALL has a rate of 92% compared to AML at 69% (Children with Cancer UK, 2017b). Adverse prognostic factors in acute leukaemia include age of diagnosis (<2 years or >10 years), male gender and unfavourable cytogenetics (Hoffbrand and Moss, 2015).
Both treatment- and disease-associated long-term effects differ between ALL and AML. For children treated for AML in particular, cardiac abnormalities and subsequent malignancies later in life are increased risks (Leung et al, 2000). Both diagnoses can cause infertility, and visual changes, in particular early cataracts, neurocognitive deficits and endocrine abnormalities such as growth delay. Secondary cancers can affect patients with a diagnosis of leukaemia. A Japanese study of 2807 children with a diagnosis of ALL found that the cumulative incidence of secondary malignancies was 1.0% after 10 years and 2.4% after 20 years (Ishida et al, 2014). In this study, secondary cancers included AML, non-Hodgkin's lymphoma, brain tumours and myelodysplastic syndrome.
In addition to these, there are long-term psychological and social impacts of undergoing treatment for cancer. Children affected by cancer are more likely than their peers to experience changes in mood such as depression or develop post-traumatic stress disorder later in life (Leukaemia and Lymphoma Society, 2019). Support for the psychosocial impact of the disease should be provided and/or signposted by the nurses involved in the patient's care.
Conclusions
The presentation of childhood leukaemia is diverse, and therefore a high index of suspicion is required for any child presenting with persistent or abnormal symptoms. A thorough assessment of the child can aid in identifying clinical signs associated with malignancy such as lymphadenopathy and hepatosplenomegaly. Recognising that abdominal and musculoskeletal symptoms are common in children presenting with leukaemia can enable earlier investigation. It is important that parental concerns about their child's symptoms or a parent's feeling that ‘something is wrong’ should not be dismissed as this is often a key theme in delayed diagnosis. Thus if presenting in the community or emergency department, an early referral to a paediatrician is required.