

The preparation of intravenous (IV) medication is risky and the more steps that are involved, the more opportunities there are for error (Sutherland et al, 2020).
Studies indicate that the incidence of errors in prescribing, preparing and administering injectable medicines is about 101 per 1000 procedures (Sutherland et al, 2020). Common types of error include using the wrong drug, incorrect calculations, inaccurate measurement of volumes, wrong diluent/carrier fluid and poor aseptic technique (Sutherland et al, 2020).
In addition to medication errors, a critical risk for nurses is needlestick injury (NSI), also called sharps injury. A recent survey of more than 7500 Royal College of Nursing (RCN) members showed that 15% had experienced a sharps injury in 2020 compared to 10% in 2008 (RCN, 2020).
In practical terms, injuries to the hands and fingers can cause considerable distress, discomfort and inconvenience and workflow can be interrupted as additional time is taken to assess, cleanse and protect the wound (Hambridge et al, 2022). To minimise these risks, the Safety (Sharp Instruments in Healthcare) Regulations 2013 in the UK and EU directive 2010/32 require employers to ensure that the use of sharps is avoided ‘so far as is reasonably practicable’ or that safer alternatives are used.
In addition, there can be hidden costs from drug wastage with current systems. A commonly followed procedure in the UK is for nurses to use a needle and syringe to draw up a diluent (usually water for injections) which is then injected into the drug vial to reconstitute the medication, which is in the form of a dry powder. The resulting solution is then drawn up and added to the carrier fluid in a small-volume IV bag. Although IV guidelines emphasise the importance ensuring that IV doses are correctly labelled at all times (RCN, 2016), if a nurse is interrupted during preparation, for example by an emergency call on the ward, there is a risk that unlabelled syringes and bags can get mixed up or can no longer be identified with certainty. Anecdotal reports suggest that nurses are aware of this risk and, when there is doubt about the contents of syringes or bags, the normal procedure is to discard them and start again. This protects the patient but is time consuming, causes unnecessary waste and incurs additional expense for the hospital.
The risks involved in mixing and dissolution are frequently overlooked. Antibiotic powders often have to be tapped and rolled repeatedly to prevent the powder from sticking to the vial surface and failing to dissolve. Consequently, reconstitution can take several minutes. If reconstitution is not performed carefully, patients can be underdosed or undissolved drug particles can be administered.
The preparation of antibiotic injections accounts for a significant proportion of nurse time. The provision of just the top 12 antimicrobial medicines as ready-to-use doses would release the time of over 4000 whole-time nurses in England, according to a recent report (Department of Health and Social Care (DHSC), 2020). The estimated saving was based on a nurse time input of 11.5 minutes to prepare an IV dose (no preparation time is needed with a ready-to-use dose). However, establishing the regional and hospital infrastructure required to deliver this saving will take time and investment.
If IV fluid containers with dual connection ports (Ecoflac® plus) and dedicated needle-free transfer devices (Ecoflac Connect) were used for this process, several steps would be eliminated (Table 1) (Figures 1 and 2).
Table 1. Comparison of steps involved in reconstitution of intravenous drugs using a needle and syringe and an Ecoflac Connect device
| Needle and syringe: 18 steps | Ecoflac Connect: 12 steps |
|---|---|
|
|


The Ecoflac Connect needle-free transfer device forms a closed system in combination with the Ecoflac plus IV container, minimising the risk of microbial contamination and ensuring that the drug being administered is clearly identifiable at all times. Furthermore, transfers are needle free, thereby avoiding the risk of NSI.
Previously, under test conditions, a comparison of the two procedures showed that using the needle-and-syringe method took 50 seconds longer to prepare and label an IV dose (B. Braun, 2020). Therefore, in the present study, the researchers designed a test with experienced nurses to test the acceptability of the needle-free transfer device and to determine the time saving achievable under more realistic conditions in an NHS simulation centre.
Leyhausen Research was commissioned to carry out the study on behalf of B. Braun.
Handling study
Method
To obtain a representative sample, a minimum of 80 nurses were required. To be eligible for the study, nurses had to fulfil the following criteria:
- Have experience in drug preparation using a needle and syringe
- Be preparing drugs using a needle and syringe at least 10 times per week
- Have experience of working with the Ecoflac plus IV container
- Have at least two years' nursing experience.
Nurses were contacted from a database of nurse contact details held by Leyhausen Research. Nurses from hospitals across England were invited to participate in the study. Once the recruitment target had been met, active recruitment was stopped, resulting in 83 nurses taking part, with 31 from university hospitals, 48 from non-university NHS hospitals, and four from private hospitals.
Each participant was asked to prepare two IV antibiotic doses (amoxicillin 500 mg, Wockhardt), the first with the usual needle-and-syringe method and the second by using Ecoflac Connect. On each occasion, the procedure was timed, starting when the nurse picked up the vial and stopping when the dose was ready for labelling. Before using the Ecoflac Connect, participants were shown a poster with handling instructions and allowed one trial run before their timed attempt. The handling tests were performed in the clinical skills and simulation centre at the Royal Brompton Hospital, London, over 7–11 March 2022.
Immediately after completing the preparation task, participants were asked a series of standard questions about their general immediate impressions of Ecoflac Connect, ease of handling, ergonomics, contamination risk and time-saving benefits.
The questions were asked by a neutral observer. Perceptions for each domain were rated on a five-point Likert scale, with 1 indicating that Ecoflac Connect was ‘much worse’ than the standard needle-and-syringe method, and 5 indicating it was ‘much better’.
For the question asking about risk of contamination, 5 indicated that the risk was ‘much lower’ and 1 indicated that it was ‘much higher’ than the needle-and-syringe method.
Each Likert scale was accompanied by a free-text field where participants could elaborate on their rating; these free-text responses were then coded into general themes. These questions were asked immediately after the handling tests to ensure responses were representative of nurses' perceptions of the two methods.
Timing data were tested for normality and analysed using SPSS version 27.0.
Results
A total of 83 nurses participated in the study. Their experience ranged from 2 to 27 years. About 50% (n=42) were senior nurses with >5 years' experience and the remainder were junior nurses with 2-5 years' experience. The majority (95%) of them worked in NHS hospitals, with 89% working in large (>150 beds) hospitals.
The mean preparation time using the needle-and-syringe method was 110.0 (SD 34.6; 95% CI (102.6–117.4)) seconds compared with 73.6 (SD 25.0; 95% CI (68.2–79.0)) seconds when using Ecoflac Connect, giving a difference of 36.6 seconds (P<0.001).
Perceptions after handling
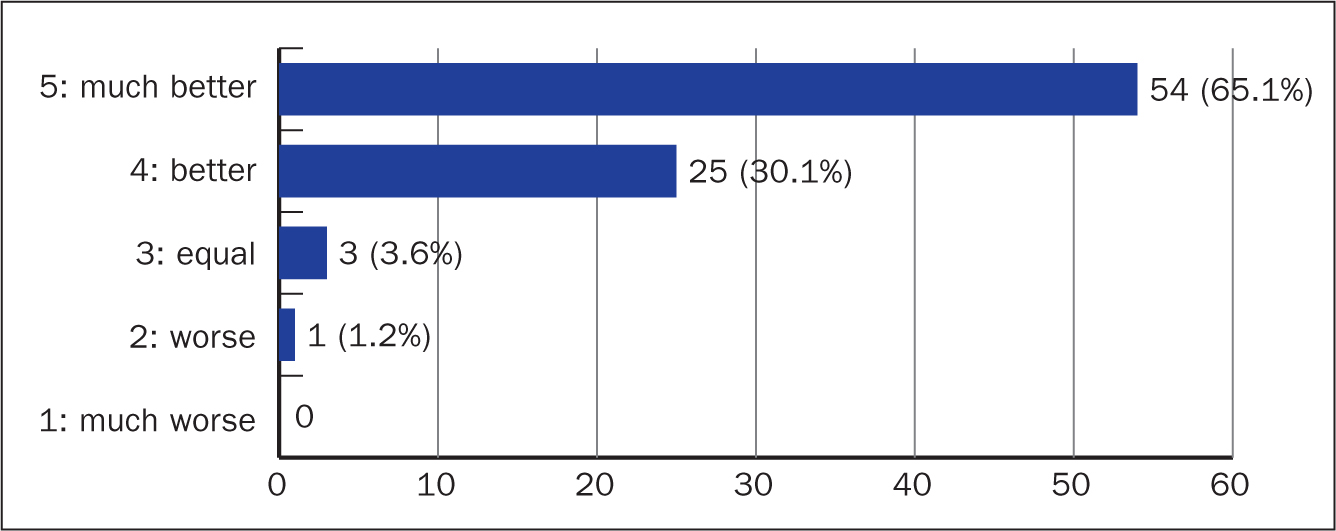
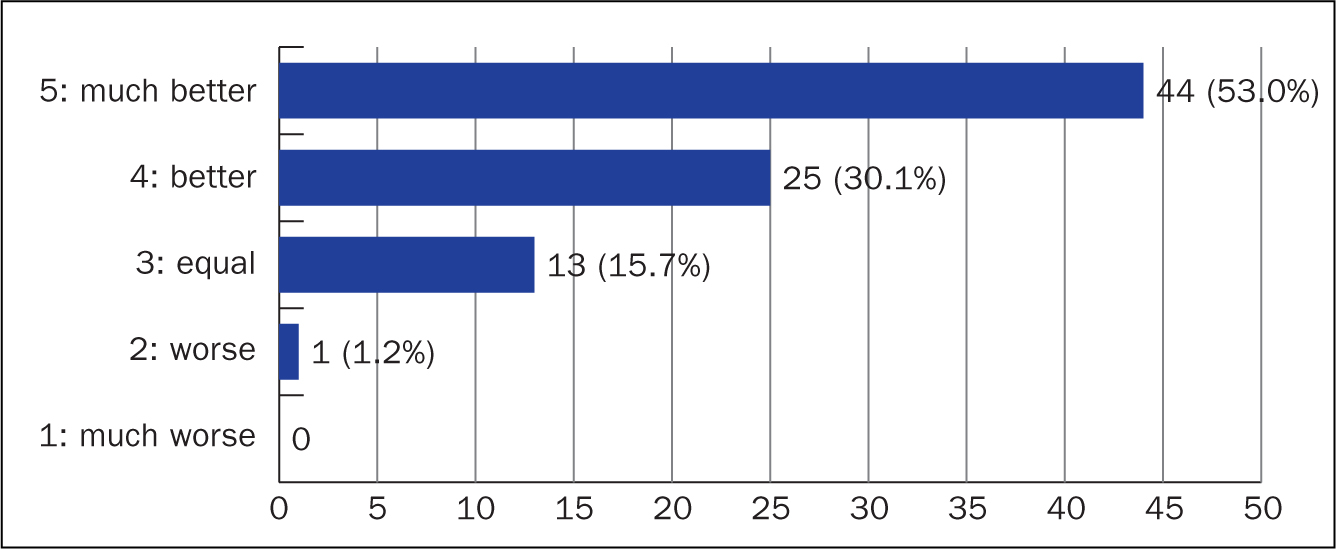
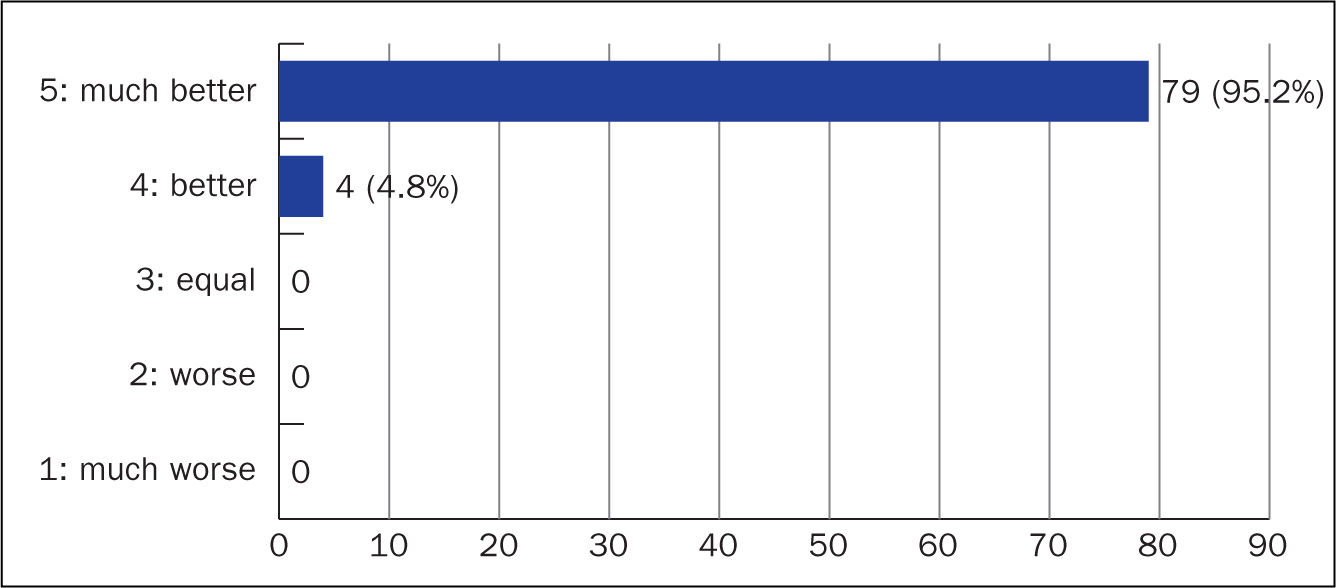
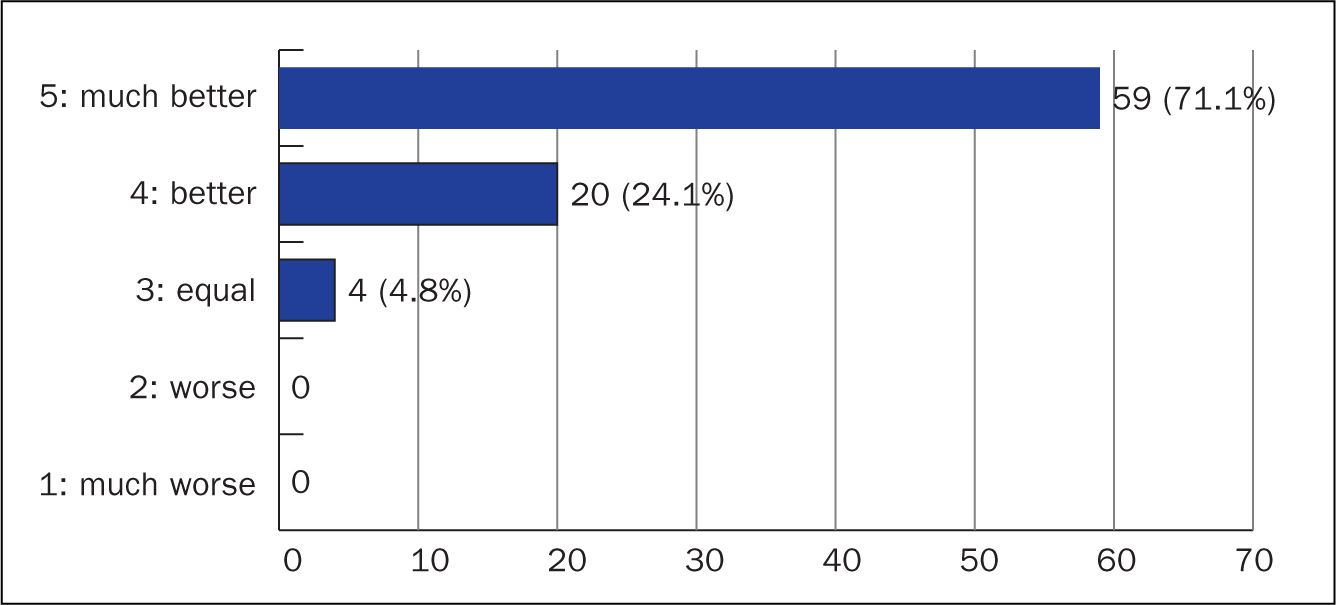
The vast majority of nurses (95%) rated ease of handling with Ecoflac Connect as ‘better’ or ‘much better’ than the needle-and-syringe method (Figure 3). For this question, only one nurse rated handling as ‘worse’ than the needle-and-syringe method but said this would improve with practice. A majority (83%) of nurses rated the time saving benefit as being ‘better’ or ‘much better’ with Ecoflac Connect than with current practice (Figure 4). All respondents rated Ecoflac Connect's ergonomics as ‘much better’ (95%) or ‘better’ (5%) than for this needle and syringe (Figure 5). Similarly, 95% of participants rated the risk of contamination with Ecoflac Connect as ‘much lower’ or ‘lower’ (Figure 6).
When asked about their general perceptions, participants highlighted ‘no risk of needlestick injury’, ‘safe and secure’ and ‘user friendly’ as handling benefits of Ecoflac Connect.
Similarly, the majority (71%) commented that Ecoflac Connect was quicker to use and saved time, with a minority (12%) saying that with more practice they could become proficient in its use, highlighting the potential for further benefit with practice. These 12% of participants comprised equal numbers of junior and senior nurses.
Commenting on ergonomics, 52% of participants said that Ecoflac Connect was easy or simple to handle. Some 25% also noted that there were fewer items to unpack, and less plastic waste was generated than from the needle-and-syringe method. A minority said more practice was needed and a few (6%) found the device heavy or difficult to connect.
All participants commented on the reduction in contamination risk. Almost all nurses (89%), especially senior nurses, perceived there were risks with procedures currently used when reconstituting IV doses. The major area of concern was NSI, raised by 54% of nurses overall, with equal proportions of junior and senior nurses mentioning this. One in five (20%) of participants specifically said the closed system was a benefit of Ecoflac Connect.
Discussion
Time saving
Antibiotics and anti-infectives account for the majority of all IV doses prepared by nurses on wards. For this reason, the DHSC (2020) based its calculations of potential benefits on the usage numbers for the top 12 antimicrobial medicines in NHS hospitals. Some products take longer than others to dissolve. Amoxicillin was chosen for this study because it is in the middle ground, being neither the most difficult nor the easiest to dissolve. In the UK, the most commonly used container is a 100 ml flexible IV bag rather than semi-rigid containers such as the Ecoflac plus.
The results of this study show that a 33% time saving on the central elements of the preparation process could be made by adopting Ecoflac Connect in place of the traditional needle-and-syringe system. The time saving was the same for both senior and junior nurses so was not affected by levels of experience. This is likely to be an underestimate of the possible time saving because the nurses who took part in the study were experienced in the needle-and-syringe method and had only one trial run of the Ecoflac Connect before making a single test preparation.
It is possible that once nurses become adept at using Ecoflac Connect, larger time savings could be achieved. A previous comparison of the two procedures under test conditions showed that the use of Ecoflac Connect by an experienced user was associated with a time saving of 50 seconds; the process took 60 seconds using Ecoflac Connect compared to 110 seconds using a needle and syringe – a 45% time difference (B. Braun, 2020).
The present study focused on the central elements of the IV dose preparation process, rather than the whole procedure. As such, it disregarded other aspects such as collecting the ingredients and equipment, preparing the sterile field, label preparation, clearing up and disposal of items such as empty containers and sharps. This accounts for the large time difference. All these issues had been factored into the real-life estimates of nurse time required for preparation of IV dose that were used in the DHSC calculation.
While many of these processes are common to both methods, there may be additional time savings when using Ecoflac Connect because fewer items have to be assembled, a benefit mentioned by 25% of participants in this study, and correspondingly fewer items have to be unwrapped before the procedure and disposed of afterwards, resulting in potential environmental and financial benefits around the costly disposal of sharps and other items in clinical waste streams.
Where wards are understaffed, the time saved could be critical, increasing available time for patient care. A recent report (DHSC, 2020) estimated that some 40 million doses of antibiotics were prepared annually by nurses in England, equivalent to 4000 full-time nurses only making antibiotic doses. Transferring preparation to pharmacy aseptic units and providing ready-to-administer doses to the wards could save £123 million. However, the infrastructure required may take years to put into place.
In the meantime, some of the burden of IV dose preparation could be relieved by using the Ecoflac Connect. Based on the figures given in the DHSC report (2020), the overall amount of nurse time freed up by implementation of the Ecoflac Connect would be equivalent to a minimum of 200-300 full-time nurses in England or a financial saving of £6.15 million-£9.23 million. For individual hospitals in England, this equates to an average of 8.1 days per trust for amoxicillin alone. In practice, this means that this amount of nursing time would then be freed up for direct patient care.
Safety
Almost all nurses (89%), especially senior nurses, perceived risks with current procedures for reconstitution of IV doses. The most commonly mentioned area of concern was NSI. Furthermore, there is evidence that NSIs are often not reported so the true frequency may be appreciably higher (RCN, 2020). As mentioned above, finger and hand injuries can cause considerable distress, discomfort and inconvenience, with interruptions to workflow as time is taken to assess and treat the wound (Hambridge, 2022).
Ecoflac Connect eliminates the risk of NSI. As mentioned above, regulations in England call for employers to ensure that the use of sharps is avoided ‘so far as is reasonably practicable’ or that safer alternatives are used. Given that the majority of IV doses are prepared on wards by nurses using the needle-and-syringe method, there is considerable scope for improvement.
Another important safety issue is clear labelling of IV admixtures. Because the drug vial is locked in the Ecoflac Connect needle-free transfer device during administration, it is possible to identify the medication that is being administered at all times. This also means that if a nurse is interrupted during the preparation process, there is no risk of an unlabelled syringe or IV bag being left unattended, and the drug can still be identified in cases of shift changes or missing documentation. Nurses report that when this happens now, the contents are usually discarded and the process started again. The permanent connection is also helpful for products that are slow to dissolve.
Resource waste
The introduction of Ecoflac Connect reduces the number of waste products and the time required to sort and dispose of them. Currently, waste products include needles, syringes and often also glass or plastic vials of water for injections.
Limitations and caveats
The recorded time saving was over half a minute per dose of amoxicillin. However, the researchers believe there are additional savings in time and resources that could not be captured by the scope of this study.
Training would be essential to ensure that drugs are completely dissolved and the full dose is drawn or drained back into the IV container.
This Ecoflac Connect/Ecoflac plus is suitable only for situations where the whole dose in a vial is used. When smaller doses or dilutions are required, the risk of calculation errors is greater and doses should be prepared in a pharmacy aseptic unit.
Further research is needed to conduct a cost comparison of the two systems. To be useful in supporting decision making, this would need to factor in: the frequency of sharps injuries and the cost-benefits of avoiding them; the time required for routine disposal of needles, syringes and additional containers; the cost of sharps disposal; and the frequency and cost of part-prepared doses having to be discarded because the contents cannot be identified with certainty.
Conclusion
The introduction of IV fluid containers and dedicated needle-free transfer devices like Ecoflac Connect would allow rapid reconstitution of IV antibiotic doses on the spot, as needed, without the need for investment in centralised aseptic facilities.
Based on the average time-saving of 36.6 seconds per preparation, the direct saving in nurse time for amoxicillin alone could free up an average of 8.1 days each year per hospital for patient care. There would also be indirect savings through avoidance of NSI and reductions in waste could offset the costs of the devices.
KEY POINTS
- Preparing intravenous antibiotic doses is a time-consuming activity that uses time that could otherwise be spent on direct patient care
- It is estimated that the provision of the top 12 antimicrobial medicines as ready-to-use injectable doses would release the time of 4000 whole-time nurses in England
- Preparing intravenous antibiotic doses using the needle-and-syringe method exposes nurses to the risk of needlestick injury
- The use of the Ecoflac Connect needle-free connector saved 36.6 seconds per dose prepared
- If Ecoflac Connect were used for amoxicillin injections alone, an average of 8.1 days of nurse time per hospital per year could be released
CPD reflective questions
- How could the process of preparation and administration of intravenous medication be made safer for nurses and patients?
- How much time is spent in your clinical setting preparing intravenous doses?
- Which products would you most like to see provided as ready-to-use injections?