
The Christie NHS Foundation Trust—the largest single-site cancer centre in Europe—is a tertiary specialist cancer centre based in Manchester, serving a population of approximately 3 million people, treating all types of solid tumours and haematologic cancers in adults (The Christie NHS Foundation Trust, 2020). The Christie is a leader in adapting patient care in response to treatment advances and policy changes, developing models for the evolving NHS, and responding to patient-centred care and efficiency initiatives (NHS England, 2016; Vanguard Innovation, 2020).
In 2015, nurses at Christie outpatient clinics began to report extended on-the-day waiting times for patients due to an increase in numbers needing treatment. As a result, The Christie began to explore ways to adapt its services to improve clinic capacity and patient experience; around this time, expanding out-of-hospital care was targeted as a priority for NHS England (2014), and homecare was predicted to have wide-ranging benefits, including reduced pressure on hospitals and improved adherence to therapies, quality of life, and patient engagement with treatment (Outram et al, 2015). As such, the team identified homecare as a service that could potentially reduce pressure on clinics, and would also provide a financial benefit via a value-added tax (VAT) saving because homecare medicines are exempt from VAT (Hackett, 2011). The resulting VAT saving would then help cover the cost of resources needed to run the homecare service (Hackett, 2011). Trastuzumab, a targeted therapy for breast cancer, was already being delivered at home, and this offered a platform for the expansion of treatment site options by The Christie.
The Christie outreach service, which covers the Greater Manchester and Cheshire area in the UK, includes 11 sites (eg local hospitals, health centres and hospices) that allow nurses to provide systemic anticancer therapy (SACT) closer to patients' homes (The Christie NHS Foundation Trust, 2020). As predicted, the homecare service complemented the outreach programme by simultaneously increasing clinic capacity and improving patient access to service. Additional treatments have been added to the homecare service as the success of the programme continues to expand. Recently, eribulin, an intravenous, second-line-or-later therapy (in the European Union—third-line or later in the USA; prior treatments should include a taxane and an anthracycline in the adjuvant or metastatic setting) for locally advanced (European Union) or metastatic breast cancer (USA and European Union) (Eisai Ltd, 2015; Eisai Inc, 2017), was added to the list of agents that could be delivered by the Christie at Home service.
The incidence of cancer and disease-related mortality are growing rapidly around the world (Torre et al, 2016; Bray et al, 2018). In response to the increasing number of patients needing therapeutic interventions and long-term care, the importance of developing an oncology homecare service has been recognised (Tralongo et al, 2011); as such, studies in several countries have demonstrated the potential benefit of homecare systems (Raphaël et al, 2005; Tralongo et al, 2011; Lüthi et al, 2012; Handley and Bekelman, 2019). This article provides an overview of the development of the Christie at Home service, using the example of administering eribulin for breast cancer treatment, with the hope that this may help guide the development of additional oncology homecare services both in the UK and abroad.
Developing a home SACT service: Christie at Home
Overview of criteria, scope, and treatments
Candidate therapies for the Christie at Home service typically meet three criteria. The therapies should have:
The service team classify administration risk based on the likelihood of a patient experiencing sensitivity to a particular drug and the likelihood of damage caused by extravasation; as such, nonvesicant drugs have been used for homecare to help reduce the risk of administration issues. Additionally, the team recommend giving a patient at least 2 cycles of treatment in a hospital setting before referring the patient for the home service; if a patient experiences any adverse event, they will be treated in the hospital rather than in the home. The preferred treatment duration of 1 hour or less enables each visiting nurse to treat enough patients in a day to make the service viable. Finally, although high-value drugs maximise VAT savings (and thereby provide financial support for homecare), there is no lower limit for drug cost–any therapy can be considered for use in the service on the basis of an improvement in the patient experience.
To date, The Christie's homecare service provides patients with subcutaneous (SC), intramuscular (IM), and intravenous (IV) SACT (including targeted agents, cytotoxics, and immunotherapies), as well as additional supportive therapy. Specific treatments successfully delivered include IM fulvestrant and SC denosumab (since July 2015), SC trastuzumab (since April 2016), IV eribulin (since April 2018), and IV nivolumab (since January 2019).
Resources for the service
Table 1 summarises the resources necessary for the Christie at Home service, along with standards, and efficiency points required for a successful homecare service. Briefly, a senior sister (lead nurse) oversees the day-to-day operation, manages the nursing team, and is responsible for the clinical governance of the home service (eg risks, incidents). Additional trained, senior SACT nurses are responsible for running the service on a day-to-day basis; these nurses prepare in advance for treatment visits, complete a clinical risk assessment for new patients, plan the visit schedule, carry out telephone and face-to-face assessments, and visit patients to administer the treatments. Senior nurses who are trained to administer SACT and are familiar with The Christie protocols are typically employed for these tasks because the role requires a level of experience, confidence, skill set, and knowledge to work autonomously in the community.
| Resources |
|---|
|
|
| Equipment |
|
|
| Quality and standards |
|
|
| Efficiency |
|
|
GPS=global-positioning system; IM=intramuscular; IT=information technology; IV=intravenous; SACT=systemic anticancer treatment; SC=subcutaneous
In addition to qualified nurses, home services benefit from an administrator/scheduler to book appointments, address telephone queries, and communicate with the patients. At The Christie, administrators also contact newly referred patients who are joining the service, check patient details, explain the service, and assess environmental risk over the phone.
Finally, a dedicated pharmacy team consisting of one pharmacist and two pharmacy technicians provide daily support for the service by clinically screening prescriptions and coordinating with the hospital pharmacy and courier service. They also liaise with clinicians to maintain a safe supply of medicines. Home service pharmacists are trained to check SACT prescriptions and they have played an important role in advising the nursing team about the overall development of the home service. Pharmacy technicians are needed to collate a daily treatment delivery list for home appointments and to coordinate the supply of drugs. These technicians liaise with third-party couriers to ensure that all necessary drugs are delivered in advance of the nurse's home visit and that the cold-storage chain is maintained (ie the courier must have a refrigerated vehicle). Technicians also help to adapt delivery schedules depending on which drug is being administered—some drugs can be delivered several days ahead of a nurse's home visit, whereas others may need to be delivered on the day of the visit.
The importance of pharmacy involvement and the implementation of robust General Data Protection Regulation (GDPR)-compliant processes for prescribing, clinical screening, dispensing, and delivery cannot be overstated—especially given the involvement of third party/external providers (eg couriers). Of note, the Royal Pharmaceutical Society (2013), the National Clinical Homecare Association (2015), and the National Homecare Medicines Committee (2018) have developed professional standards for homecare services, with the overarching goal of achieving a consistent quality of homecare services that will prevent avoidable harm while optimising outcomes. Although these associations do not oversee The Christie, the team strives to achieve and surpass the industry standard of care.
Potential pitfalls for any at-home service can be avoided with a special focus on procurement, packaging and storage, and communication. Although some drugs are purchased from a standard wholesaler, eribulin and others must be compounded before dispensing. This is often an unusual process for a dispensing pharmacy, so processes must be robust enough to ensure that there is no interruption to treatment. All parties involved (dispensary, courier, and patient) must also adhere to guidance on drug storage to ensure that the cold-storage chain is maintained up to administration and safe storage is sustained in the home. Therefore, communication must be good between different teams within the organisation (oncology clinicians and homecare team), as well as with external service providers (eg couriers with GDPR-compliant processes), to ensure the smooth running of the service.
Equipment for ‘Christie at Home’ service
The equipment for the Christie at Home service is summarised in Table 1. Briefly, nurses require a 4G-enabled laptop to access medical notes and prescriptions and to document care in real time; additionally, nurses are given a mobile telephone to reach each other and communicate with personnel at the hospital, if necessary. Because nurses typically work alone, safety is of paramount importance—to facilitate their safety, a GPS-enabled security device is provided to each nurse for emergencies. Lastly, a fleet of cars has been leased for the Christie at Home service because nurses can drive over 80 miles daily to cover The Christie's patient catchment area.
Success of the service
Christie at Home activity has continued to grow since its inception in 2015 (Figure 1): there have been 11 906 Christie at Home treatments between 2015 and 2019 (Figure 1A) and the breakdown by therapy of Christie at Home treatments in 2018 is detailed in Figure 1B. In general, the treatments administered most frequently (ie breast cancer treatments) have been used in the home service for the longest period of time; however, all treatment numbers are expected to increase as more patients are referred and awareness of the home service spreads throughout The Christie.
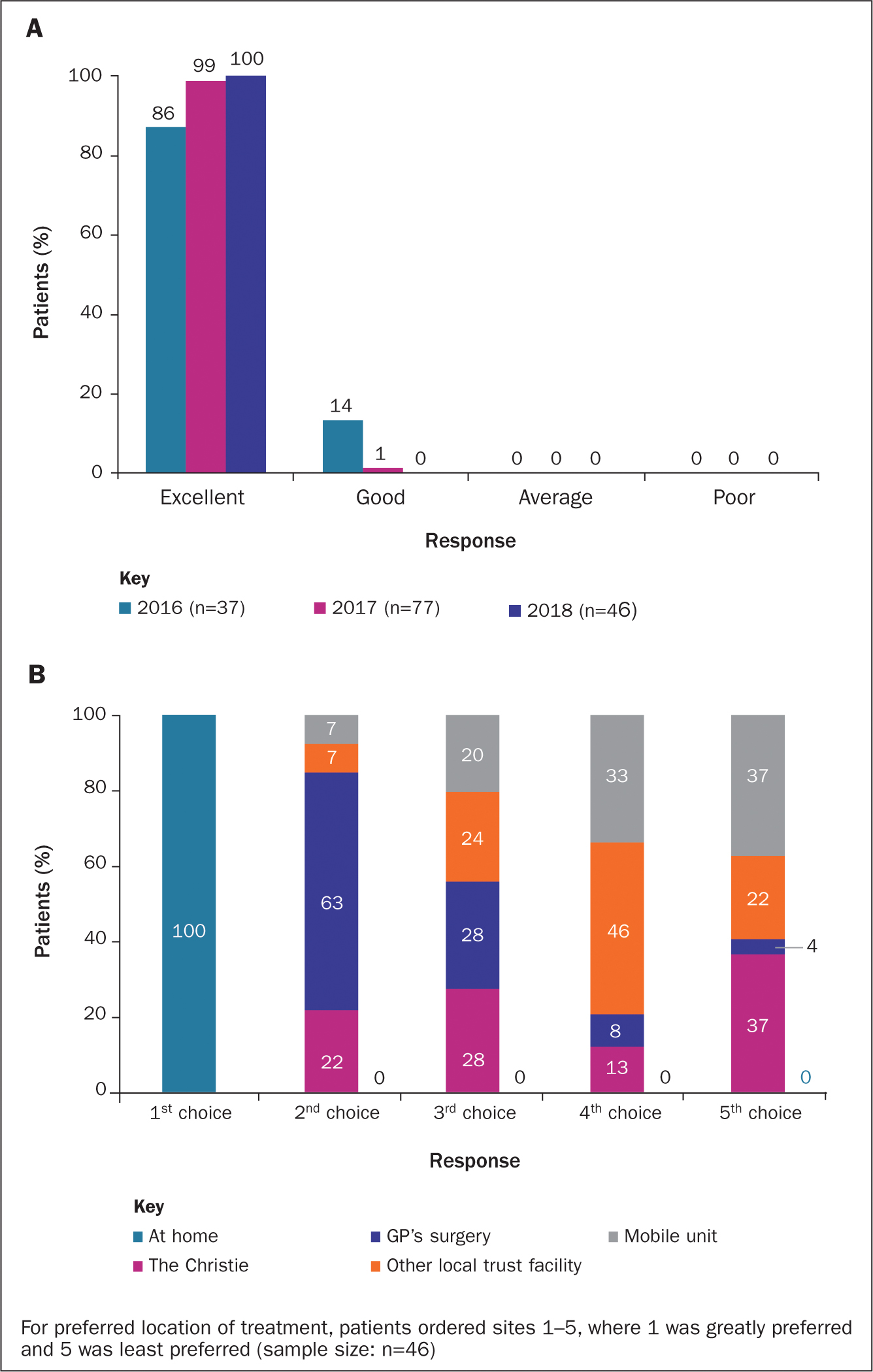
The patient-rated standard of care among those who have participated in the Christie at Home service has been high from the onset (Figure 2): in 2018, 100% of surveyed patients receiving home service rated the standard of care as ‘excellent’ (Figure 2A), and patients indicated that treatment at home was desired over any other location (Figure 2B). Improvements in homecare over time can likely be attributed to the effort that The Christie has put into the continued development of its service; such developments have included the recruitment of a senior sister and a dedicated pharmacy technician to the service, the addition of nurses experienced in SACT, and administrative and pharmacy support. Over time, experience has translated into improved processes and an efficient service.
Challenges of homecare services
Current challenges with homecare are centred around working alone (ie risk, safety, and support), working in a home environment (ie space, equipment, spillage), wasting of drugs (ie, spoilage due to patient fridge failure, albeit rare, or where a drug is delivered and treatment stopped before it is administered), and the complex needs of the patient group. To date, it has not been possible to eliminate waste because most treatments are delivered in advance; however, as the service develops this will be monitored closely and steps will be taken to reduce waste wherever possible.
Future challenges could arise in the event of changing VAT rules, the availability of biosimilar/generic medications, and with emerging needs of an already complex patient group. Although imminent VAT changes are not anticipated, any such changes would require an assessment of impact on the homecare service; similarly, the introduction of biosimilar medicines, which tend to carry a lower financial burden, could reduce savings.
Despite these potential challenges, cost is only one aspect of home service to consider—a positive patient experience is the key driver for The Christie. As an expanding list of treatment types (such as immunotherapy) is deemed suitable for delivery in the home, and as side-effects and holistic needs of patients will continue to change, the team will be challenged to recognise and adapt to patients' developing needs.
Christie at Home service: focus on eribulin
Findings from the EMBRACE phase 3 clinical trial showed that eribulin significantly improves overall survival relative to treatment of physician's choice in patients with heavily pretreated metastatic breast cancer (hazard ratio, 0.81; 95% CI: 0.66, 0.99; P=0.041) (Cortes et al, 2011). Moreover, eribulin demonstrated a manageable safety profile (Cortes et al, 2011). A Christie audit of 75 eribulin-treated patients had similar outcomes and patients had no unexpected toxicities; as such, these results show the effectiveness of eribulin in a real-world setting.
Eribulin was selected for the Christie at Home outreach service because it met all the criteria for homecare drugs. Specifically, based on The Christie's experience with eribulin at the main hospital, eribulin (a nonvesicant drug) was considered well tolerated, carrying a low risk of hypersensitivity/infusion reactions. Moreover, it has a short administration time (ie, 30-minute infusion) and is considered a high-cost agent. Patient feedback suggested a need to improve the patient experience for this group of patients, who were often travelling 2 out of every 3 weeks to the main treatment site from far away to receive a 30-minute infusion. From April 2018 to January 2019, there have been 58 IV eribulin treatments at home compared with 643 IV hospital treatments. In addition to reducing unnecessary trips to the hospital for these patients, providing eribulin at home has afforded the main hospital extra capacity to administer other treatments that cannot be delivered elsewhere.
Details regarding important steps for successful eribulin treatment at home are highlighted in Table 2. As eribulin is ‘high cost’ and requires compounding, it is referred to as an ‘on hold’ drug, meaning that the compounding partners require a request to be made, which first relies on blood results and a review of the patient no more than 48 hours ahead of treatment, as set out in The Christie's protocol. These product-specific issues translate into a short turnaround time for compounding, dispensing and delivery before treatment. Accordingly, eribulin must be delivered on the day of treatment instead of 2 days before (as is typically done for other treatments provided by the home service); as such, a greater level of coordination between the courier and the nursing staff is necessary to ensure delivery in time for treatment.
| Day-2 |
|
| Day-1 |
|
| Day 0 |
|
Future directions and global implications
As the incidence of cancer continues to rise globally (Jemal et al, 2011; Bray et al, 2018), models to improve cancer care will need to be implemented (Tralongo et al, 2011). Specifically, homecare, which has been used for the treatment of various diseases, is being recognised as an important model for oncology throughout the world (Handley and Bekelman, 2019).
A recent article discussing the possibility of implementing oncology homecare in the USA (Handley and Bekelman, 2019) presented three challenges that must be met for the successful implementation of a homecare service. These were patient selection; staffing, monitoring and resource allocation; and reimbursement. Notably, the Christie at Home model of homecare service provides an adequate solution to all three of these challenges, although reimbursement would be notably different in the USA versus the UK. The experience at The Christie has also shown that patients prefer to receive treatment at home and that patients treated at home are satisfied with the care they receive—a finding that is supported by other homecare studies (Rischin et al, 2000; Hall and Lloyd 2008;).
Centres providing cancer treatment should consider the benefits of homecare for their patients. As the concept of homecare gains popularity, it may be helpful for The Christie to conduct detailed comparisons of the patient experience at different locations to continue to make necessary adjustments to improve patient care and satisfaction. Moreover, ongoing review of treatments/procedures that may be suitable for home administration will allow The Christie to continue to meet patient needs. To date, the homecare service is administering five therapies that are available through the SACT outreach service. In the future, the hope is to expand the Christie at Home services to encompass other treatments and aspects of care, including short transfusion time (≤30 minutes), low-risk, IV infusions (30 minutes), haematology drugs, hormonal therapies, IV antibiotics, phlebotomy services, and patient assessments.
Summary
The Christie has developed, implemented, and maintained a homecare service for delivery of SACT to patients with cancer. The team believe this model is one that other clinics/hospitals in the UK and abroad can make use of as they begin to develop their own homecare services.